You might also like
- Effects of Risperidone and Olanzapine Dose Reduction On Cognitive Function in Stable Patients With SchizophreniaDocument6 pagesEffects of Risperidone and Olanzapine Dose Reduction On Cognitive Function in Stable Patients With Schizophreniawen zhangNo ratings yet
- Low-Dose Quetiapine in Schizophrenia: Meta-Analysis High-: The Psychiatrist OnlineDocument5 pagesLow-Dose Quetiapine in Schizophrenia: Meta-Analysis High-: The Psychiatrist OnlineMichael CoxNo ratings yet
- Ajp 156 5 702Document8 pagesAjp 156 5 7029 PsychologyNo ratings yet
- 08 Aj 0844Document11 pages08 Aj 0844kenikirkucing2No ratings yet
- Ajp.161.10.1837 2Document11 pagesAjp.161.10.1837 2HKANo ratings yet
- Olanzapine For Schizophrenia Refractory To Typical and Atypical Antipsychotics: An Open-Label, Prospective TrialDocument6 pagesOlanzapine For Schizophrenia Refractory To Typical and Atypical Antipsychotics: An Open-Label, Prospective TrialLeslie CitromeNo ratings yet
- CHORHostility CITROME PsychServ2001Document5 pagesCHORHostility CITROME PsychServ2001Leslie CitromeNo ratings yet
- Clozapine Alone Versus Clozapine and Risperidone With Refractory SchizophreniaDocument11 pagesClozapine Alone Versus Clozapine and Risperidone With Refractory SchizophreniawardahNo ratings yet
- Farmacológico AutismoDocument9 pagesFarmacológico AutismoArmando GalvanNo ratings yet
- New Developments in Antidepressant TherapyDocument5 pagesNew Developments in Antidepressant TherapyDoyin AwodeleNo ratings yet
- Clozapine and Haloperidol in ModeratelyDocument8 pagesClozapine and Haloperidol in Moderatelyrinaldiapt08No ratings yet
- Effect of Aripiprazole Augmentation of Clozapine in SchizophreniaDocument28 pagesEffect of Aripiprazole Augmentation of Clozapine in SchizophreniaamaldutaNo ratings yet
- Freudenreich 2002Document8 pagesFreudenreich 2002citra kurnia pratiwiNo ratings yet
- Tianeptine Combination For Partial or Non-Response To Selective Serotonin Re-Uptake Inhibitor MonotherapyDocument9 pagesTianeptine Combination For Partial or Non-Response To Selective Serotonin Re-Uptake Inhibitor MonotherapyJosuéNo ratings yet
- Appi Ajp 2015 14101251Document8 pagesAppi Ajp 2015 14101251sarahNo ratings yet
- Trial of Psilocybin Versus Escitalopram For Depression: Original ArticleDocument10 pagesTrial of Psilocybin Versus Escitalopram For Depression: Original ArticleCristina Duran GarcíaNo ratings yet
- Clozapine Augmented With Risperidone in The Treatment of Schizophrenia: A Randomized, Double-Blind, Placebo-Controlled TrialDocument8 pagesClozapine Augmented With Risperidone in The Treatment of Schizophrenia: A Randomized, Double-Blind, Placebo-Controlled TrialIga Faldini GazaliNo ratings yet
- Atypical Antipsychotics in Autism TreatmentDocument14 pagesAtypical Antipsychotics in Autism TreatmentEliana RieraNo ratings yet
- Revisión AntipsicóticosDocument6 pagesRevisión AntipsicóticosManel EMNo ratings yet
- Update 2015 Tratament AutismDocument9 pagesUpdate 2015 Tratament AutismamaandreiNo ratings yet
- Potkin2002 QTP+ Hal Risp Thiridazine RCTDocument10 pagesPotkin2002 QTP+ Hal Risp Thiridazine RCTIulia CiocotisanNo ratings yet
- Alzheimer PicoDocument6 pagesAlzheimer PicoRaja Friska YulandaNo ratings yet
- A Comparative Study of The Efficacy and Safety of Mirtazapine Versus Amitriptyline in The Treatment of Major DepressionDocument6 pagesA Comparative Study of The Efficacy and Safety of Mirtazapine Versus Amitriptyline in The Treatment of Major DepressionSyarif MaulanaNo ratings yet
- Shared Psychotic Disorder Case ReportDocument25 pagesShared Psychotic Disorder Case ReportPramelia Gereldina PalembanganNo ratings yet
- Serum Monitoring of Antipsychotic Drug Levels During Concomitant Administration of Sertraline and Antipsychotic MedicationDocument4 pagesSerum Monitoring of Antipsychotic Drug Levels During Concomitant Administration of Sertraline and Antipsychotic MedicationIulia CiocotisanNo ratings yet
- Ann Pharmacother 2011 Owenby 95 100Document6 pagesAnn Pharmacother 2011 Owenby 95 100Mahmud AnshoriNo ratings yet
- 174 Full PDFDocument7 pages174 Full PDFAsyha KantifaNo ratings yet
- Aripiprazol vs Quetiapine for Acute PsychosisDocument4 pagesAripiprazol vs Quetiapine for Acute PsychosisAsti DwiningsihNo ratings yet
- Brexpiprazole: A Review of A New Treatment Option For Schizophrenia and Major Depressive DisorderDocument6 pagesBrexpiprazole: A Review of A New Treatment Option For Schizophrenia and Major Depressive DisorderLuis Pablo HsNo ratings yet
- Ketamine Augmentation Rapidly Improves Depression Scores in Inpatients With Treatment-Resistant Bipolar DepressionDocument6 pagesKetamine Augmentation Rapidly Improves Depression Scores in Inpatients With Treatment-Resistant Bipolar DepressionNfaleNo ratings yet
- Dose Reduction of Risperidone and Olanzapine Can Improve Cognitive Function and Negative Symptoms in Stable Schizophrenic PatientsDocument9 pagesDose Reduction of Risperidone and Olanzapine Can Improve Cognitive Function and Negative Symptoms in Stable Schizophrenic PatientsEmerson Serafim G. MonteiroNo ratings yet
- Efecto de Dextrometorfano - Bupropion en Ttno Depresivo MayorDocument10 pagesEfecto de Dextrometorfano - Bupropion en Ttno Depresivo MayorLina MariaNo ratings yet
- Clozapin RisperidonDocument7 pagesClozapin RisperidonAnonymous 2LcGdsRNo ratings yet
- Cannabis and ShizoDocument2 pagesCannabis and ShizoFarah MuthiaNo ratings yet
- BrexpiprazolDocument11 pagesBrexpiprazolastrogliaNo ratings yet
- Clozapine: SchizophrenicDocument8 pagesClozapine: SchizophrenicVictoria FellowsNo ratings yet
- Research PaperDocument13 pagesResearch PaperMirudhu BaasiniNo ratings yet
- PindolDocument1 pagePindolSaloua El fakirNo ratings yet
- ParanoiaDocument1 pageParanoiaFedericoFornariNo ratings yet
- Activity and Onset of Action of Reboxetine and Effect of Combination With Sertraline in An Animal Model of DepressionDocument10 pagesActivity and Onset of Action of Reboxetine and Effect of Combination With Sertraline in An Animal Model of DepressionIsaac Saucedo FloresNo ratings yet
- Atypical Antipsychotic Augmentation in Major Depressive DisorderDocument13 pagesAtypical Antipsychotic Augmentation in Major Depressive DisorderrantiNo ratings yet
- Articles: BackgroundDocument13 pagesArticles: BackgroundBianca AlinaNo ratings yet
- Clotiapine - Another Forgotten Treassure in PsychiatryDocument1 pageClotiapine - Another Forgotten Treassure in PsychiatryJuan IgnacioNo ratings yet
- A Selective Summary of Psychopharmacology Research Published in Second Half of 2015Document9 pagesA Selective Summary of Psychopharmacology Research Published in Second Half of 2015gion.nandNo ratings yet
- Tohen 2003Document9 pagesTohen 2003Francisco VillalonNo ratings yet
- Lap Chak 2003Document6 pagesLap Chak 2003Zahra NisaNo ratings yet
- 070674370805300610Document6 pages070674370805300610kak fulanNo ratings yet
- Escitalopram in Post Traumatic Stress DisorderDocument11 pagesEscitalopram in Post Traumatic Stress DisorderVivekNo ratings yet
- Risperdal Tablets and Solution PiDocument27 pagesRisperdal Tablets and Solution PiIzam M. FalahNo ratings yet
- Comparison Between Clozapine, An Atypical Antipsychotic Agent and Haloperidol, A Conventional Agent Used To Treat SchizophreniaDocument6 pagesComparison Between Clozapine, An Atypical Antipsychotic Agent and Haloperidol, A Conventional Agent Used To Treat SchizophreniaLonkesNo ratings yet
- Aripiprazole Maintains Clinical Improvements in Bipolar ManiaDocument12 pagesAripiprazole Maintains Clinical Improvements in Bipolar ManiaSherly VeronicaNo ratings yet
- Antipsychotic augmentation vs. monotherapy meta-analysisDocument13 pagesAntipsychotic augmentation vs. monotherapy meta-analysisvanfafiafiaNo ratings yet
- Antipsychotic Augmentation vs. Monotherapy in Schizophrenia: Systematic Review, Meta-Analysis and Meta-Regression AnalysisDocument13 pagesAntipsychotic Augmentation vs. Monotherapy in Schizophrenia: Systematic Review, Meta-Analysis and Meta-Regression AnalysisvanfafiafiaNo ratings yet
- Kane1988 PDFDocument8 pagesKane1988 PDFRavi KumarNo ratings yet
- DBT PharmacotherapyDocument3 pagesDBT PharmacotherapyMadNo ratings yet
- A Randomized, Double-Blind, Placebo-Controlled Study of Citalopram in Adolescents With Major Depressive Disorder - Von Knorring 2006Document5 pagesA Randomized, Double-Blind, Placebo-Controlled Study of Citalopram in Adolescents With Major Depressive Disorder - Von Knorring 2006Julio JuarezNo ratings yet
- SAGE 217 Nuevo Tratamiento para La DepresionDocument9 pagesSAGE 217 Nuevo Tratamiento para La DepresionRodolfo Diaz VelizNo ratings yet
- Paroxetine Personality 2Document9 pagesParoxetine Personality 2PrissTinkNo ratings yet
- LurasidoneDocument1 pageLurasidoneRaju Teach KapsNo ratings yet
- Second and Third Generation Antipsychotics: A Comprehensive HandbookFrom EverandSecond and Third Generation Antipsychotics: A Comprehensive HandbookRating: 5 out of 5 stars5/5 (1)
- TriazolamProductLabel 1019 PDFDocument13 pagesTriazolamProductLabel 1019 PDFLeslie CitromeNo ratings yet
- See Full Prescribing Information For Complete Boxed WarningDocument14 pagesSee Full Prescribing Information For Complete Boxed WarningLeslie CitromeNo ratings yet
- ZolpidemProductLabel 0819 PDFDocument7 pagesZolpidemProductLabel 0819 PDFLeslie CitromeNo ratings yet
- RamelteonProductLabel 1218 PDFDocument18 pagesRamelteonProductLabel 1218 PDFLeslie CitromeNo ratings yet
- DoxepinSleepProductLabel 0310 PDFDocument4 pagesDoxepinSleepProductLabel 0310 PDFLeslie CitromeNo ratings yet
- DoxepinSleepProductLabel 0310 PDFDocument4 pagesDoxepinSleepProductLabel 0310 PDFLeslie CitromeNo ratings yet
- WhatIsTranscranialMagneticStimulation CITROME KlineLine1999Document1 pageWhatIsTranscranialMagneticStimulation CITROME KlineLine1999Leslie CitromeNo ratings yet
- TriazolamProductLabel 1019 PDFDocument13 pagesTriazolamProductLabel 1019 PDFLeslie CitromeNo ratings yet
- RamelteonProductLabel 1218 PDFDocument18 pagesRamelteonProductLabel 1218 PDFLeslie CitromeNo ratings yet
- CATIENNTEditorialRegardingCITROME KERWIN IntJClinPract2006Document2 pagesCATIENNTEditorialRegardingCITROME KERWIN IntJClinPract2006Leslie CitromeNo ratings yet
- Restoril™ (Temazepam) Capsules USP RX Only Warning: Risks From Concomitant Use With OpioidsDocument14 pagesRestoril™ (Temazepam) Capsules USP RX Only Warning: Risks From Concomitant Use With OpioidsLeslie CitromeNo ratings yet
- ZolpidemProductLabel 0819 PDFDocument7 pagesZolpidemProductLabel 0819 PDFLeslie CitromeNo ratings yet
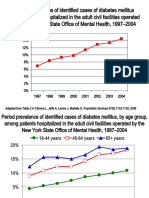
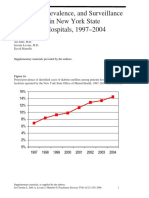
- IncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster CITROME NCDEU2006Document1 pageIncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster CITROME NCDEU2006Leslie CitromeNo ratings yet
- See Full Prescribing Information For Complete Boxed WarningDocument14 pagesSee Full Prescribing Information For Complete Boxed WarningLeslie CitromeNo ratings yet
- IncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster For Distribution CITROME CINP2006Document1 pageIncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster For Distribution CITROME CINP2006Leslie CitromeNo ratings yet
- IncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster For Distribution CITROME CINP2006Document1 pageIncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster For Distribution CITROME CINP2006Leslie CitromeNo ratings yet
- Diabetes prevalence trends in NY mental hospitalsDocument8 pagesDiabetes prevalence trends in NY mental hospitalsLeslie CitromeNo ratings yet
- Sscchhiizzoopphhrreenniiaa: Ccuurrrreenntt Ttrreeaattm Meenntt CcoonnssiiddeerraattiioonnssDocument4 pagesSscchhiizzoopphhrreenniiaa: Ccuurrrreenntt Ttrreeaattm Meenntt CcoonnssiiddeerraattiioonnssLeslie CitromeNo ratings yet
- Ziprasidone efficacy against hostility in schizophreniaDocument1 pageZiprasidone efficacy against hostility in schizophreniaLeslie CitromeNo ratings yet
- INTRODUCTION (Continued)Document1 pageINTRODUCTION (Continued)Leslie CitromeNo ratings yet
- Incidence and Prevalence of Diabetes in NY Psychiatric Hospitals 1997-2004Document5 pagesIncidence and Prevalence of Diabetes in NY Psychiatric Hospitals 1997-2004Leslie CitromeNo ratings yet
- NR330 Efficacy of Ziprasidone Against Hostility in SchizophreniaDocument1 pageNR330 Efficacy of Ziprasidone Against Hostility in SchizophreniaLeslie CitromeNo ratings yet
- OlanzapineHighDoseRCTHGLFPoster KINON CINP2006Document19 pagesOlanzapineHighDoseRCTHGLFPoster KINON CINP2006Leslie CitromeNo ratings yet
- QuetiapineAntiaggressiveAgentCaseReport CITROME JCP2001Document1 pageQuetiapineAntiaggressiveAgentCaseReport CITROME JCP2001Leslie CitromeNo ratings yet
- Catechol-O-methyltransferase and Monoamine Oxidase-A Polymorphisms and Treatment Response To Typical and Atypical NeurolepticsDocument3 pagesCatechol-O-methyltransferase and Monoamine Oxidase-A Polymorphisms and Treatment Response To Typical and Atypical NeurolepticsLeslie CitromeNo ratings yet
- ReducingInpatientAggressionPayingAttentionPaysOffPoster NOLAN APA2006Document1 pageReducingInpatientAggressionPayingAttentionPaysOffPoster NOLAN APA2006Leslie CitromeNo ratings yet
- DiabetesSchizophreniaInterview CITROME BehavHealthCare2006Document8 pagesDiabetesSchizophreniaInterview CITROME BehavHealthCare2006Leslie CitromeNo ratings yet
- Benefits of A Second Dose of Intramuscular (IM) Aripiprazole To Control Agitation in Patients With Schizophrenia or Bipolar I DisorderDocument1 pageBenefits of A Second Dose of Intramuscular (IM) Aripiprazole To Control Agitation in Patients With Schizophrenia or Bipolar I DisorderLeslie CitromeNo ratings yet
- OlanzapineEarlyPredictorsWeightGainBipolarDisorder LIPKOVICH JClinPsychopharm2006Document5 pagesOlanzapineEarlyPredictorsWeightGainBipolarDisorder LIPKOVICH JClinPsychopharm2006Leslie CitromeNo ratings yet
- MedicalTrainingUnitedStatesAddendum CITROME CMAJ1992Document2 pagesMedicalTrainingUnitedStatesAddendum CITROME CMAJ1992Leslie CitromeNo ratings yet
- Accepted ManuscriptDocument41 pagesAccepted ManuscriptArgenis SalinasNo ratings yet
- Fatality Report WolskiDocument17 pagesFatality Report Wolskiedmontonjournal100% (1)
- 1998 - Metaphor in Psychotherapy - CloseDocument296 pages1998 - Metaphor in Psychotherapy - CloseElena Draghici100% (3)
- International Journal of Nursing Studies Volume 60 - Effects of Nurse-Led Child - and Parent-Focused Violence InterventioDocument12 pagesInternational Journal of Nursing Studies Volume 60 - Effects of Nurse-Led Child - and Parent-Focused Violence InterventioAndika FahruroziNo ratings yet
- Biopsychosocial2 Bangloy Baniqued BaratetaDocument4 pagesBiopsychosocial2 Bangloy Baniqued BaratetaPrince Robert ChuaNo ratings yet
- The Discriminative Capacity of CBCLDSM5 ScalesDocument8 pagesThe Discriminative Capacity of CBCLDSM5 ScalesIsabel BelisaNo ratings yet
- Integrating Health and Mental Health Services - A Past and Future HistoryDocument6 pagesIntegrating Health and Mental Health Services - A Past and Future HistoryPedro ReyesNo ratings yet
- The Mayo Clinic Experience With Psychogenic Purpura (Gardner-Diamond Syndrome)Document10 pagesThe Mayo Clinic Experience With Psychogenic Purpura (Gardner-Diamond Syndrome)AlejandraNo ratings yet
- Systemic Sex Therapy, 3rd EditionDocument321 pagesSystemic Sex Therapy, 3rd EditionOrshanetz88% (8)
- Intellectual Disabilities in of Mice of MenDocument3 pagesIntellectual Disabilities in of Mice of Menapi-457162411No ratings yet
- Adhd - Apa PDFDocument27 pagesAdhd - Apa PDFzoranmunkNo ratings yet
- DSM and AddictionsDocument10 pagesDSM and AddictionsNilsa RoblesNo ratings yet
- Case Study Demi Lovato Bipolar DisorderDocument5 pagesCase Study Demi Lovato Bipolar DisorderYzar Velasco0% (1)
- Alanna Bailey PosterDocument1 pageAlanna Bailey PosterAlexander TegarNo ratings yet
- Falling in Love With Love Oedipal and Postoedipal Manifestations of Idealization, Mourning, And Erotic MasochismέΑΦThe Ghost of Masochism in the Queer SubjectDocument22 pagesFalling in Love With Love Oedipal and Postoedipal Manifestations of Idealization, Mourning, And Erotic MasochismέΑΦThe Ghost of Masochism in the Queer SubjectΘελξινόη ΘελξινοηNo ratings yet
- Fall 2015 Disorientation GuideDocument32 pagesFall 2015 Disorientation GuideharoldNo ratings yet
- UT Dallas Syllabus For Psy4343.001.09f Taught by Marion Underwood (Undrwd)Document5 pagesUT Dallas Syllabus For Psy4343.001.09f Taught by Marion Underwood (Undrwd)UT Dallas Provost's Technology GroupNo ratings yet
- E.2 Bipolar PPT 2017Document42 pagesE.2 Bipolar PPT 2017abrihamNo ratings yet
- A. Human BehaviorDocument8 pagesA. Human BehaviorSilver LisingNo ratings yet
- Autismo - PBE - Naturalistic Intervention - FactsheetDocument2 pagesAutismo - PBE - Naturalistic Intervention - FactsheetmaximilianogaeteNo ratings yet
- College of Arts and Sciences Introduction To Clinical Psychology Midterm Exam ESSAY. Answer The Following Questions As DirectedDocument4 pagesCollege of Arts and Sciences Introduction To Clinical Psychology Midterm Exam ESSAY. Answer The Following Questions As DirectedParvez MohamedNo ratings yet
- Case PresentationDocument25 pagesCase PresentationGaurav TanwarNo ratings yet
- Clinical Cases in PsychiatryDocument161 pagesClinical Cases in PsychiatryAna Roman100% (35)
- Psychiatric Case History NotesDocument8 pagesPsychiatric Case History NotesTysle100% (1)
- Improving General Hospital Care For People With Dementia: Why, How and With Whom?Document14 pagesImproving General Hospital Care For People With Dementia: Why, How and With Whom?rowanpurdyNo ratings yet
- The Clinical NeuropsychologistDocument13 pagesThe Clinical NeuropsychologistPriscila FreitasNo ratings yet
- Chronic Traumatic EncephalopathyDocument5 pagesChronic Traumatic EncephalopathyEdson Mota Aguilera50% (2)
- BibliopocDocument4 pagesBibliopocKarlo ReyesNo ratings yet
- Skillstreaming Research (Annotated Bibliography)Document17 pagesSkillstreaming Research (Annotated Bibliography)jeff_helgesenNo ratings yet
- History of Nursing Development Worldwide and in IndonesiaDocument15 pagesHistory of Nursing Development Worldwide and in IndonesiaRaditio Bismo Prabowo II100% (2)