You might also like
- Florence Tamagne A History of Homosexuality in Europe PDFDocument473 pagesFlorence Tamagne A History of Homosexuality in Europe PDFCarlos Alberto Barzani100% (1)
- Homework-1 Fall 2021Document1 pageHomework-1 Fall 2021Elif HalıcıNo ratings yet
- Polycystic Ovarian Syndrome (PCOS) : ComplicationsDocument1 pagePolycystic Ovarian Syndrome (PCOS) : ComplicationsSahnia Uli SilitongaNo ratings yet
- Pharmacy Education Article Page 107Document42 pagesPharmacy Education Article Page 107Cristine ChubiboNo ratings yet
- Finance Dissertation TopicsDocument2 pagesFinance Dissertation Topicsmonabiswas100% (1)
- Tonetti Et Al-2018-Journal of Periodontology TDocument14 pagesTonetti Et Al-2018-Journal of Periodontology TJonathan Meza MauricioNo ratings yet
- Age Specific References For IgDDocument8 pagesAge Specific References For IgDBassem AhmedNo ratings yet
- The 2022 Update of IUIS Phenotypical Classifcation For Human Inborn Errors of ImmunityDocument13 pagesThe 2022 Update of IUIS Phenotypical Classifcation For Human Inborn Errors of ImmunitygabrielNo ratings yet
- 1 s2.0 S1198743X14607667 MainDocument15 pages1 s2.0 S1198743X14607667 MainiisisiisNo ratings yet
- 07 Intravenous Immunoglobulin Replacement Therapy in Children With Primary Immunodeficiency Diseases A Nurse S GuideDocument9 pages07 Intravenous Immunoglobulin Replacement Therapy in Children With Primary Immunodeficiency Diseases A Nurse S GuidekiminoooNo ratings yet
- Eur J Immunol - 2020 - Hanitsch - Treatment and Management of Primary Antibody Deficiency German InterdisciplinaryDocument15 pagesEur J Immunol - 2020 - Hanitsch - Treatment and Management of Primary Antibody Deficiency German InterdisciplinaryRSU Trijaya medical centerNo ratings yet
- Virus y M. Pneumoniae Son Los Ppales Agentes Etiologicas de NAC en Pacientes Hospitalizados en EspañaDocument11 pagesVirus y M. Pneumoniae Son Los Ppales Agentes Etiologicas de NAC en Pacientes Hospitalizados en EspañaFernando FernándezNo ratings yet
- Intravenous Immunoglobulin Immunotherapy For Coronavirus Disease-19 (COVID-19)Document6 pagesIntravenous Immunoglobulin Immunotherapy For Coronavirus Disease-19 (COVID-19)my accountNo ratings yet
- Journal Homepage: - : IntroductionDocument5 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Allergy - 2022 - Farraia - Allergen Immunotherapy For Asthma Prevention A Systematic Review and Meta Analysis ofDocument17 pagesAllergy - 2022 - Farraia - Allergen Immunotherapy For Asthma Prevention A Systematic Review and Meta Analysis ofpedrotiagosilvaNo ratings yet
- Intravenous ImmunoglobulinDocument6 pagesIntravenous ImmunoglobulinAnastasia TjanNo ratings yet
- The EuroFlow PID Orientation Tube For Flow Cytometric Diagnostic Screening of Primary Immunodeficiencies of The Lymphoid SystemDocument11 pagesThe EuroFlow PID Orientation Tube For Flow Cytometric Diagnostic Screening of Primary Immunodeficiencies of The Lymphoid SystemLiliana SolariNo ratings yet
- Pedsos 1Document7 pagesPedsos 1RizalMarubobSilalahiNo ratings yet
- Antibiotics 11 01664Document15 pagesAntibiotics 11 01664Ottofianus Hewick KalangiNo ratings yet
- Effect of An Intervention To Improve The Prescription of Antifungals in Pediatric Hematology-OncologyDocument8 pagesEffect of An Intervention To Improve The Prescription of Antifungals in Pediatric Hematology-Oncologygema putraNo ratings yet
- SEOM GEICO Clinical Guidelines On Endometrial CancerDocument10 pagesSEOM GEICO Clinical Guidelines On Endometrial CancerJose Richard Tenazoa VillalobosNo ratings yet
- 10 1016@j Jpeds 2021 05 008Document10 pages10 1016@j Jpeds 2021 05 008Irvin AlfaroNo ratings yet
- IVIG Guiding PrinciplesDocument7 pagesIVIG Guiding PrinciplesSomaiaNo ratings yet
- Mekanisme IVIGDocument13 pagesMekanisme IVIGSebilah Sabil NoerNo ratings yet
- Cardona Et Al 2018 AllergyDocument5 pagesCardona Et Al 2018 AllergydregleavNo ratings yet
- Treatment With Tocilizumab or Corticosteroids For COVID 2021 Clinical MicroDocument9 pagesTreatment With Tocilizumab or Corticosteroids For COVID 2021 Clinical MicroSusanyi ErvinNo ratings yet
- RARE & Orphan Diseases - Epidemiology & Public HealthDocument1 pageRARE & Orphan Diseases - Epidemiology & Public HealthMichael John AguilarNo ratings yet
- Martin 13 Dec 2022Document11 pagesMartin 13 Dec 2022Manuel MendozaNo ratings yet
- 20220115-8166-4705cj Ivermectin Prophylaxis Used For COVID-19Document25 pages20220115-8166-4705cj Ivermectin Prophylaxis Used For COVID-19Hansley Templeton CookNo ratings yet
- Multicenter Evaluation of The Panbio™ COVID-19 Rapid Antigendetection Test For The Diagnosis of SARS-CoV-2 InfectionDocument5 pagesMulticenter Evaluation of The Panbio™ COVID-19 Rapid Antigendetection Test For The Diagnosis of SARS-CoV-2 InfectionamyNo ratings yet
- What Is The Role of Technology in Improving Patient Safety? A French, German and UK Healthcare Professional PerspectiveDocument6 pagesWhat Is The Role of Technology in Improving Patient Safety? A French, German and UK Healthcare Professional PerspectiveTricia Jane OpinaldoNo ratings yet
- Antibiotic Prescriptions and Prophylaxis in Italian Children. Is It Time To Change? Data From The ARPEC ProjectDocument14 pagesAntibiotic Prescriptions and Prophylaxis in Italian Children. Is It Time To Change? Data From The ARPEC ProjectEfan Stiawan100% (1)
- Mini Review Laboratory Diagnosis For Covid-19: A Mini-ReviewDocument5 pagesMini Review Laboratory Diagnosis For Covid-19: A Mini-ReviewwellaNo ratings yet
- Risks of 23 Speci Fic Malformations Associated With Prenatal Exposure To 10 Antiepileptic DrugsDocument14 pagesRisks of 23 Speci Fic Malformations Associated With Prenatal Exposure To 10 Antiepileptic DrugsLuthfiyyaNo ratings yet
- Jurnal MPIDocument4 pagesJurnal MPIMarini TaslimaNo ratings yet
- Non Kepi Vaccines RevisedDocument28 pagesNon Kepi Vaccines Revisedokwadha simionNo ratings yet
- 10 1111@aas 13453Document8 pages10 1111@aas 13453medicnanaNo ratings yet
- Guideline - Diagnosis - Genetic - Pheochromocytomas 2021Document25 pagesGuideline - Diagnosis - Genetic - Pheochromocytomas 2021mehidimed1889No ratings yet
- Multidisciplinary Practice Guidelines For The Diagnosis, Genetic Counseling and Treatment of Pheochromocytomas and ParagangliomasDocument19 pagesMultidisciplinary Practice Guidelines For The Diagnosis, Genetic Counseling and Treatment of Pheochromocytomas and ParagangliomasLaura Marina IlincaNo ratings yet
- 43 Sangeetha EtalDocument3 pages43 Sangeetha EtaleditorijmrhsNo ratings yet
- Eclinicalmedicine: Research PaperDocument8 pagesEclinicalmedicine: Research PaperEl LitoralNo ratings yet
- Efficacy+of+IgM+Rich+Immunoglobin+for+Bacterial+Sepsis (Case Control)Document6 pagesEfficacy+of+IgM+Rich+Immunoglobin+for+Bacterial+Sepsis (Case Control)Tristiani UtariNo ratings yet
- Oby 23014Document22 pagesOby 23014FatimaNo ratings yet
- Ann Clin Transl Neurol - 2022 - Lee - The Safety and Efficacy of Intravenous Immunoglobulin in Autoimmune EncephalitisDocument12 pagesAnn Clin Transl Neurol - 2022 - Lee - The Safety and Efficacy of Intravenous Immunoglobulin in Autoimmune EncephalitisJohanna ValentinaNo ratings yet
- Clasificacion Fenotipica de ID 2015 PDFDocument12 pagesClasificacion Fenotipica de ID 2015 PDFEnrico Emilio LatorracaNo ratings yet
- Allergy - 2020 - Pfaar - Placebo Effects in Allergen Immunotherapy An EAACI Task Force Position PaperDocument19 pagesAllergy - 2020 - Pfaar - Placebo Effects in Allergen Immunotherapy An EAACI Task Force Position PaperKohinoorKohinoorNo ratings yet
- The 2017 IUIS Phenotypic Classification For PrimarDocument15 pagesThe 2017 IUIS Phenotypic Classification For PrimarAna Lucia Baeza DuranNo ratings yet
- Solowska Et Al DX and MGT of COVID Vaccine ReactionsDocument31 pagesSolowska Et Al DX and MGT of COVID Vaccine ReactionsJoshua TamayoNo ratings yet
- 2015 Consensus Document On The Approach To Children With Allergic Reactions After Vaccination or Allergy To Vaccine ComponentsDocument22 pages2015 Consensus Document On The Approach To Children With Allergic Reactions After Vaccination or Allergy To Vaccine ComponentsamallullaNo ratings yet
- Impaired Type I Interferon Activity and Exacerbated Inflammatory Responses in Severe Covid-19 PatientsDocument31 pagesImpaired Type I Interferon Activity and Exacerbated Inflammatory Responses in Severe Covid-19 PatientsSusana PaçoNo ratings yet
- Estudio Serología Covid Del LaboratoriDocument8 pagesEstudio Serología Covid Del LaboratoriJorge TriforceNo ratings yet
- Casa Bonne 2016Document11 pagesCasa Bonne 2016Jose Angel AbadíaNo ratings yet
- 14 Practica+clinica+6Document19 pages14 Practica+clinica+6Yilianeth Mena DazaNo ratings yet
- ESCMID Guideline For The Diagnosis and Management of Candida Diseases 2012: Diagnostic ProceduresDocument10 pagesESCMID Guideline For The Diagnosis and Management of Candida Diseases 2012: Diagnostic ProceduresiisisiisNo ratings yet
- Convalescent Plasma Therapy in Patients With COVID-19: ConcisereviewDocument7 pagesConvalescent Plasma Therapy in Patients With COVID-19: ConcisereviewendaNo ratings yet
- Wagner2022 Article EfficacyAndSafetyOfIntravenousDocument13 pagesWagner2022 Article EfficacyAndSafetyOfIntravenoustito reddyNo ratings yet
- 431 2022 Article 4703Document11 pages431 2022 Article 4703Naylen MedinaNo ratings yet
- Q1.IMG Vs IMGL+Corticoides. Sin ResultadosDocument10 pagesQ1.IMG Vs IMGL+Corticoides. Sin ResultadosMari Carmen GrandasNo ratings yet
- Immunoglobulin Treatment of Immunodeficient Patients: Yıldız CamcıoğluDocument24 pagesImmunoglobulin Treatment of Immunodeficient Patients: Yıldız Camcıoğlukj185No ratings yet
- Summary of The Evidence For Ivermectin in COVID-19Document3 pagesSummary of The Evidence For Ivermectin in COVID-19Kent CheeNo ratings yet
- Eficacia InmunoglobulinasDocument10 pagesEficacia InmunoglobulinasDanisse RoaNo ratings yet
- DDocument31 pagesDIgnacioNo ratings yet
- The Surveillance of Antibiotics Resistance in Indonesia: A Current ReportsDocument6 pagesThe Surveillance of Antibiotics Resistance in Indonesia: A Current ReportsRahmanu ReztaputraNo ratings yet
- Allergy - 2021 - Muraro - EAACI Guidelines Anaphylaxis 2021 UpdateDocument21 pagesAllergy - 2021 - Muraro - EAACI Guidelines Anaphylaxis 2021 Updatemuhammad rizka hidayatNo ratings yet
- Clinically Relevant Mycoses: A Practical ApproachFrom EverandClinically Relevant Mycoses: A Practical ApproachElisabeth PresterlNo ratings yet
- CH 9 ArticulationsDocument40 pagesCH 9 ArticulationsRobin ToneyNo ratings yet
- Sci4 ST2 Q3Document2 pagesSci4 ST2 Q3KayelNo ratings yet
- Early Development in BirdsDocument53 pagesEarly Development in BirdsMuqaddas NadeemNo ratings yet
- Lipedema Giving Smarter GuideDocument41 pagesLipedema Giving Smarter GuideThuaret100% (1)
- Sanctuaries and National Parks - Environmental LawsDocument17 pagesSanctuaries and National Parks - Environmental LawsSuman SharmaNo ratings yet
- Topic 3 - Crisis Management PolicyDocument10 pagesTopic 3 - Crisis Management PolicyArjay JulianNo ratings yet
- Neurologist Deborah Boland, D.O., MSPT, Named "Physician of The Year"Document3 pagesNeurologist Deborah Boland, D.O., MSPT, Named "Physician of The Year"PR.comNo ratings yet
- December 2013 NLE Room Assignments - Davao CityDocument150 pagesDecember 2013 NLE Room Assignments - Davao CityjamieboyRNNo ratings yet
- Plant Pathology McGrawDocument865 pagesPlant Pathology McGrawAnjali OjhaNo ratings yet
- MODULE 3 ActivityDocument5 pagesMODULE 3 ActivityEricka Mae AbreaNo ratings yet
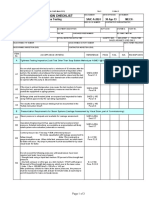
- SAIC-A-2024 Rev 6 Leakness Tightness TestDocument3 pagesSAIC-A-2024 Rev 6 Leakness Tightness Testpookkoya thangalNo ratings yet
- A Study On Reclosing of Asaluyeh-Isfahan 765 KV TL Considering The Effect of Neutral Reactor in Reducing Resonant VoltagesDocument5 pagesA Study On Reclosing of Asaluyeh-Isfahan 765 KV TL Considering The Effect of Neutral Reactor in Reducing Resonant VoltagesCarlos Lino Rojas AgüeroNo ratings yet
- Digital AddictionDocument3 pagesDigital AddictionTefroy DimayalNo ratings yet
- Compressed Gases PDFDocument21 pagesCompressed Gases PDFCarlos Ramón Plazaola LorioNo ratings yet
- Gloria Macapagal ArroyoDocument14 pagesGloria Macapagal ArroyoJefferyl BagalayosNo ratings yet
- Parasitology Study GuideDocument16 pagesParasitology Study GuideesraaNo ratings yet
- DHCC Exam - Dubai (Dubai Healthcare City Authority)Document14 pagesDHCC Exam - Dubai (Dubai Healthcare City Authority)Maha TayyabNo ratings yet
- Patulot v. PeopleDocument11 pagesPatulot v. PeopleNeil SubacNo ratings yet
- Case ScenarioDocument4 pagesCase ScenarioAl TheóNo ratings yet
- A4 Case Study Design 5 2Document7 pagesA4 Case Study Design 5 2Bautista JunNo ratings yet
- 13B1X00277000096 A 01 14.ja - enDocument2 pages13B1X00277000096 A 01 14.ja - enRadiology SolutionsNo ratings yet
- Chicken Parties ND3 Project - 010249 - 122914Document68 pagesChicken Parties ND3 Project - 010249 - 122914blessingNo ratings yet
- CM692 Im6129 Yh135 PDFDocument90 pagesCM692 Im6129 Yh135 PDFmoises100% (1)
- National Economics University Advanced Educational Program: 3. Should Working Mums Be Given Special Privileges?Document4 pagesNational Economics University Advanced Educational Program: 3. Should Working Mums Be Given Special Privileges?Dương Nguyễn ThuỳNo ratings yet
- BlackRock Global Investor Pulse Core ReleaseDocument3 pagesBlackRock Global Investor Pulse Core ReleaseJoshua MaherNo ratings yet