You might also like
- Comparison of Characteristics of Stroke-Associated Pneumonia in Stroke Care Units in Indonesia and JapanDocument6 pagesComparison of Characteristics of Stroke-Associated Pneumonia in Stroke Care Units in Indonesia and JapanMaulana DimasNo ratings yet
- The Benefit of Dysphagia Screening in Adult Patients With Stroke A Meta-AnalysisDocument61 pagesThe Benefit of Dysphagia Screening in Adult Patients With Stroke A Meta-AnalysisAlexandreNo ratings yet
- Content ServerDocument8 pagesContent ServerG. Araya MoraNo ratings yet
- The Paradoxical Protective Effect of Liver Steatosis On Severity and Functional Outcome of Ischemic StrokeDocument7 pagesThe Paradoxical Protective Effect of Liver Steatosis On Severity and Functional Outcome of Ischemic StrokewinnerfromparisNo ratings yet
- Book StrokeDocument196 pagesBook Strokemadalena limaNo ratings yet
- Prevalence of Dyslipidemia in Ischemic StrokeDocument6 pagesPrevalence of Dyslipidemia in Ischemic StrokeiglesiasowenNo ratings yet
- Lakunar and Outcome StrokeDocument11 pagesLakunar and Outcome StrokesitialimahNo ratings yet
- SR Si ImaDocument6 pagesSR Si ImaZulkifli PomalangoNo ratings yet
- Head Position in Acute Stroke Trial Statistical Analysis PlanDocument5 pagesHead Position in Acute Stroke Trial Statistical Analysis PlanNurul AzmiyahNo ratings yet
- Clinico Radiological Risk Factors AssociDocument4 pagesClinico Radiological Risk Factors AssociMartha OktaviaNo ratings yet
- Medi 97 E10919Document4 pagesMedi 97 E10919oktaviaNo ratings yet
- International Journal of Gerontology: Gwo-Chi Hu, Yi-Min ChenDocument5 pagesInternational Journal of Gerontology: Gwo-Chi Hu, Yi-Min Chenluthfia ayu az zahraNo ratings yet
- Population-Based Study of Incidence, Risk Factors, Outcome, and Prognosis of Ischemic Peripheral Arterial EventsDocument11 pagesPopulation-Based Study of Incidence, Risk Factors, Outcome, and Prognosis of Ischemic Peripheral Arterial EventsIrina NeamtuNo ratings yet
- BallDocument8 pagesBallAllan Alejandro SevillaNo ratings yet
- Anticoagulacion Temprana Vs Tardia en ACV Con FADocument11 pagesAnticoagulacion Temprana Vs Tardia en ACV Con FACesar Mauricio Daza CajasNo ratings yet
- MNJ ToastDocument4 pagesMNJ ToastRichard SuherlimNo ratings yet
- Higher Prevalence of Diabetes in Pontine Infarction Than inDocument8 pagesHigher Prevalence of Diabetes in Pontine Infarction Than inMarshall ThompsonNo ratings yet
- E1512 FullDocument16 pagesE1512 Fullamilkar morunoNo ratings yet
- Sacks2018 PDFDocument13 pagesSacks2018 PDFJonathan Paucar ArévaloNo ratings yet
- nihms271845Document17 pagesnihms271845Andres Mauricio MuñozNo ratings yet
- Journal Review BobbyDocument7 pagesJournal Review BobbybobbyNo ratings yet
- Annals of Neurology - 2017 - Espay - Deconstructing Normal Pressure Hydrocephalus Ventriculomegaly As Early Sign ofDocument11 pagesAnnals of Neurology - 2017 - Espay - Deconstructing Normal Pressure Hydrocephalus Ventriculomegaly As Early Sign ofErika PérezNo ratings yet
- ANNALS DementiaDocument16 pagesANNALS DementiaewbNo ratings yet
- Analysis of Risk Factors For Different Subtypes of Acute Coronary SyndromeDocument12 pagesAnalysis of Risk Factors For Different Subtypes of Acute Coronary SyndromeAfrial ImamNo ratings yet
- Neshige 2015Document5 pagesNeshige 2015belleswanNo ratings yet
- Jurnal Kedokteran Dan Kesehatan IndonesiaDocument11 pagesJurnal Kedokteran Dan Kesehatan IndonesiaZefqy Wahyu MardianaNo ratings yet
- Edlow 2018Document15 pagesEdlow 2018arianaNo ratings yet
- FCVM 09 1022658Document20 pagesFCVM 09 1022658francogarciaramirez1No ratings yet
- Epidemiology, Risk Profile, Management, and Outcome in Geriatric Patients With Atrial Fibrillation in Two Long Term Care HospitalsDocument9 pagesEpidemiology, Risk Profile, Management, and Outcome in Geriatric Patients With Atrial Fibrillation in Two Long Term Care HospitalsGrupo A Medicina UAEMNo ratings yet
- Constipation in Stroke PatiensDocument6 pagesConstipation in Stroke PatiensfatmawatiNo ratings yet
- Practice Guideline Summary: Sudden Unexpected Death in Epilepsy Incidence Rates and Risk FactorsDocument10 pagesPractice Guideline Summary: Sudden Unexpected Death in Epilepsy Incidence Rates and Risk FactorsB NadyaNo ratings yet
- 00235-2020 FullDocument9 pages00235-2020 FullM Ibnu Rahman SyahNo ratings yet
- Association Between Poststroke Epilepsy and Death: A Nationwide Cohort StudyDocument7 pagesAssociation Between Poststroke Epilepsy and Death: A Nationwide Cohort StudybelleswanNo ratings yet
- brb3 1291Document9 pagesbrb3 1291meyvitasNo ratings yet
- Stroke - Severity - Modified - The - Effect - of - Chronic.66 TromboliziraniDocument5 pagesStroke - Severity - Modified - The - Effect - of - Chronic.66 TromboliziraniM StojanovskaNo ratings yet
- Artigo 2Document20 pagesArtigo 2ANDREZA ALMEIDANo ratings yet
- Identificacion Choque Cardiogenico ERDocument9 pagesIdentificacion Choque Cardiogenico ERZai RojasNo ratings yet
- PFO-AHA Guidelines 2020 PDFDocument11 pagesPFO-AHA Guidelines 2020 PDFsdfasdfasdfadfsNo ratings yet
- Cholesterol Levels Are Associated With 30-Day Mortality From Ischemic Stroke in Dialysis PatientsDocument9 pagesCholesterol Levels Are Associated With 30-Day Mortality From Ischemic Stroke in Dialysis PatientsRay HannaNo ratings yet
- Ischemic Cerebrovascular Accident and Its Secondary Renal ImpairmentDocument5 pagesIschemic Cerebrovascular Accident and Its Secondary Renal ImpairmentAditya Angela AdamNo ratings yet
- 1 s2.0 S0741521417303932 Main PDFDocument9 pages1 s2.0 S0741521417303932 Main PDFDzulRizkaNo ratings yet
- Risk Factors and Mechanisms of Stroke in Young Adults: The FUTURE StudyDocument11 pagesRisk Factors and Mechanisms of Stroke in Young Adults: The FUTURE StudyRizka FebrianaNo ratings yet
- Prediction and Verification of The Effect of Psoriasis On Coronary 2022 HeliDocument6 pagesPrediction and Verification of The Effect of Psoriasis On Coronary 2022 HeliMixa TekluNo ratings yet
- 828 FullDocument7 pages828 FullMayra LoeraNo ratings yet
- Annals of Neurology - 2021 - Polymeris - Oral Anticoagulants in The Oldest Old With Recent Stroke and Atrial FibrillationDocument11 pagesAnnals of Neurology - 2021 - Polymeris - Oral Anticoagulants in The Oldest Old With Recent Stroke and Atrial FibrillationJavier RamirezNo ratings yet
- Jurnal Carolin SidhartaDocument13 pagesJurnal Carolin SidhartaCaroline SidhartaNo ratings yet
- Newly Diagnosed Anemia Linked to Higher Parkinson's Disease RiskDocument7 pagesNewly Diagnosed Anemia Linked to Higher Parkinson's Disease Riskdiah_budiarti_1No ratings yet
- Frontiers Neutrophil-to-Lymphocyte Ratio As A Predictive Biomarker For Stroke Severity and Short-Term Prognosis in Acute IscheDocument1 pageFrontiers Neutrophil-to-Lymphocyte Ratio As A Predictive Biomarker For Stroke Severity and Short-Term Prognosis in Acute IscheDeepika devasenaNo ratings yet
- Posterior Circulation Stroke: Advances in Understanding and ManagementFrom EverandPosterior Circulation Stroke: Advances in Understanding and ManagementJong S. KimNo ratings yet
- Physician Screening Tool Evaluates Dysphagia in Stroke PatientsDocument10 pagesPhysician Screening Tool Evaluates Dysphagia in Stroke PatientsIgnacio AndresNo ratings yet
- Jamaneurology Topcuoglu 2017 Oi 170047Document8 pagesJamaneurology Topcuoglu 2017 Oi 170047LadycherryNo ratings yet
- Accepted Manuscript: 10.1016/j.neuint.2017.01.005Document42 pagesAccepted Manuscript: 10.1016/j.neuint.2017.01.005Irvin MarcelNo ratings yet
- Prognostic Factors of Functional Outcome in Post-Acute Stroke in The Rehabilitation UnitDocument9 pagesPrognostic Factors of Functional Outcome in Post-Acute Stroke in The Rehabilitation UnitIda Ayu Trisna DewiNo ratings yet
- Eye Acupuncture Treatment For Stroke A SystematicDocument11 pagesEye Acupuncture Treatment For Stroke A SystematicIngdrawati TjiangNo ratings yet
- JamdaDocument9 pagesJamdaw5rh7kqg6pNo ratings yet
- Journal 4Document7 pagesJournal 4Denys PutraNo ratings yet
- Alteraciones Adultos MayoresDocument12 pagesAlteraciones Adultos MayoresGabriel Zúñiga MartinezNo ratings yet
- Evaluation_of_clinical_spectrum_and_risk_factors_iDocument9 pagesEvaluation_of_clinical_spectrum_and_risk_factors_imeenakshi.r.agrawalNo ratings yet
- Ts Jurnal Batak SarapDocument6 pagesTs Jurnal Batak SarapAdityaNo ratings yet
- Consequences of OSADocument11 pagesConsequences of OSAhammodihotmailcomNo ratings yet
- Top 21 Largest EMS Companies in WorldDocument22 pagesTop 21 Largest EMS Companies in WorldjackNo ratings yet
- XR5 9 Element 5 Band Yagi 20-17-15-12-10MDocument16 pagesXR5 9 Element 5 Band Yagi 20-17-15-12-10Msboonuy331No ratings yet
- Gen Ed Answer Key (A)Document7 pagesGen Ed Answer Key (A)Antonette Escarpe TorcinoNo ratings yet
- Computational Models For Trunk Trajectory Planning and Load Distribution: A Test-Bed For Studying Various Clinical Adaptation and Motor Control Strategies of Low Back Pain PatientsDocument13 pagesComputational Models For Trunk Trajectory Planning and Load Distribution: A Test-Bed For Studying Various Clinical Adaptation and Motor Control Strategies of Low Back Pain PatientsOTorresGonzalezNo ratings yet
- Yanmar Mechnical PumpDocument16 pagesYanmar Mechnical Pump송성훈100% (9)
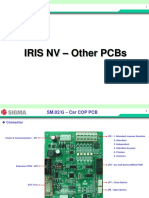
- 07 IRIS NV PCB OtherDocument15 pages07 IRIS NV PCB OtherArnaldo cordovaNo ratings yet
- 1 Proforma of Allotment LetterDocument32 pages1 Proforma of Allotment LetterGovind SandhaNo ratings yet
- 5988-4082EN Designers GuidDocument82 pages5988-4082EN Designers GuidAndreaNo ratings yet
- New Patient Needing Continuous Renal Replacement Therapy (CRRT)Document9 pagesNew Patient Needing Continuous Renal Replacement Therapy (CRRT)sergey_1972No ratings yet
- Binzel - Katalog MAGDocument64 pagesBinzel - Katalog MAGAdrian KustraNo ratings yet
- Foreign Body Airway ObstructionDocument6 pagesForeign Body Airway ObstructionReeja RajeshNo ratings yet
- Rules For The CertificationDocument84 pagesRules For The CertificationhdelriovNo ratings yet
- Mobile Network Optimization MapDocument1 pageMobile Network Optimization MapShahzad Farooq100% (1)
- Hydromechanical Piercing Perforation: Oil Service Innovation TechnologiesDocument8 pagesHydromechanical Piercing Perforation: Oil Service Innovation TechnologiesЕлена ПаниотNo ratings yet
- Wood Plastic and CompositesDocument5 pagesWood Plastic and CompositesBenjie LatrizNo ratings yet
- Fit For WashingDocument85 pagesFit For WashingIyaka YoeNo ratings yet
- SK716 Pengintegrasian Mekanisme Nilai Karbon (English)Document13 pagesSK716 Pengintegrasian Mekanisme Nilai Karbon (English)Isti HanifahNo ratings yet
- Welcome Students!: Week 8 (3 Quarter)Document28 pagesWelcome Students!: Week 8 (3 Quarter)Erika Lloren Luyun-GaliaNo ratings yet
- Pak AgingDocument34 pagesPak AgingDavid LopezNo ratings yet
- A History of The Jewish People in The Time of Jesus Christ (1891) Index Schürer, Emil, 1844-1910Document132 pagesA History of The Jewish People in The Time of Jesus Christ (1891) Index Schürer, Emil, 1844-1910David Bailey100% (2)
- Bentley Bentayga BrochureDocument9 pagesBentley Bentayga BrochureGerry CalàNo ratings yet
- Essotherm 500 PDFDocument8 pagesEssotherm 500 PDFdonyaNo ratings yet
- Gem EscortingDocument7 pagesGem Escortingsuman sutharNo ratings yet
- EU Food Label GuidanceDocument99 pagesEU Food Label GuidanceMunteanu CristianNo ratings yet
- Acute Severe Asthma Hospital ManagementDocument1 pageAcute Severe Asthma Hospital ManagementItharshan IndreswaranNo ratings yet
- 2a CTRL DecDocument75 pages2a CTRL Decramanathan balamoorthyNo ratings yet
- Guillain Barre 3Document6 pagesGuillain Barre 3YON LEANDRO VILLAMIL ROJASNo ratings yet
- 5 Variable K-MapDocument15 pages5 Variable K-MapBen SewellNo ratings yet
- Air release plug and lifting lug details for 15 MVA 66/11.55 kV transformer radiatorDocument1 pageAir release plug and lifting lug details for 15 MVA 66/11.55 kV transformer radiatorshravan Kumar SinghNo ratings yet
- Meralco Bill 330370940102 04142023Document2 pagesMeralco Bill 330370940102 04142023Jha CruzNo ratings yet