You might also like
- Dental Caries FinalDocument40 pagesDental Caries FinalSimran KathuriaNo ratings yet
- Pediatric Dentistry Lab Manual and Clinical GuideDocument99 pagesPediatric Dentistry Lab Manual and Clinical GuideJames MonroeNo ratings yet
- 08-The Heritability of Malocclusion-Part 2 The Influence of Genetics in Malocclusion PDFDocument9 pages08-The Heritability of Malocclusion-Part 2 The Influence of Genetics in Malocclusion PDFFadi Al Hajji100% (1)
- Alfred Gysi1929Document25 pagesAlfred Gysi1929Eduardo Basañez RiveraNo ratings yet
- Development of Dentition and Occlusion: Sujina.SDocument214 pagesDevelopment of Dentition and Occlusion: Sujina.SsathyaNo ratings yet
- Vertical dimension orthodontic possibilitiesDocument32 pagesVertical dimension orthodontic possibilitiesRehabilitación OralNo ratings yet
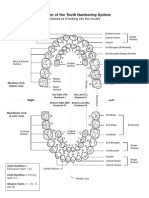
- Diagram of The Tooth Numbering SystemDocument1 pageDiagram of The Tooth Numbering Systemsaleh900No ratings yet
- Permanent Maxillary Molars: Form and FunctionDocument35 pagesPermanent Maxillary Molars: Form and FunctionpadmineekrishnanNo ratings yet
- Development of OcclusionDocument98 pagesDevelopment of OcclusionDrNidhi Krishna100% (2)
- Single Complete Denture FinalDocument15 pagesSingle Complete Denture FinalVikas AggarwalNo ratings yet
- Torque in OrthodonticsDocument157 pagesTorque in OrthodonticsVasundhra Mittal93% (15)
- Caries PPT - ppt11Document109 pagesCaries PPT - ppt11dr parveen bathlaNo ratings yet
- Research TOC: Dental DeductionsDocument29 pagesResearch TOC: Dental DeductionsÉrikaOrtsacNo ratings yet
- HeadgearDocument62 pagesHeadgearAmanda Rosy RoneyNo ratings yet
- Roth's Prescription / Orthodontic Courses by Indian Dental AcademyDocument64 pagesRoth's Prescription / Orthodontic Courses by Indian Dental Academyindian dental academy100% (1)
- 6 Elements 1 PDFDocument6 pages6 Elements 1 PDFdocbraun100% (1)
- Second Molars ExtractionDocument13 pagesSecond Molars ExtractionSyed Mohammad Osama AhsanNo ratings yet
- Fundamentals of Tooth Preparations For Cast Metal and Porcelain Restorations PDFDocument369 pagesFundamentals of Tooth Preparations For Cast Metal and Porcelain Restorations PDFnutacosmyn100% (3)
- Endodontic TherapyDocument243 pagesEndodontic TherapyRadu FuseaNo ratings yet
- Impacted Maxillary CaninesDocument7 pagesImpacted Maxillary CaninesAly OsmanNo ratings yet
- Variability in Tooth Size Between Four Human GroupsDocument24 pagesVariability in Tooth Size Between Four Human GroupsvaleroyNo ratings yet
- Scot 1988Document28 pagesScot 1988Freddy Campos SotoNo ratings yet
- Intertooth Patterns of Hypoplasia Expression: Implications For Childhood Health in The Classic Maya CollapseDocument15 pagesIntertooth Patterns of Hypoplasia Expression: Implications For Childhood Health in The Classic Maya CollapseNancy MoralesNo ratings yet
- Rehabilitacion de La Denticion Desgastada - Johansson Et Al - JOR 2008Document19 pagesRehabilitacion de La Denticion Desgastada - Johansson Et Al - JOR 2008Pablo BenitezNo ratings yet
- Marija B. Radovic Starinar 62Document10 pagesMarija B. Radovic Starinar 62Milena VasiljevicNo ratings yet
- Talon Cusp Affecting Primary Dentition in Two Siblings: A Case ReportDocument3 pagesTalon Cusp Affecting Primary Dentition in Two Siblings: A Case ReportUniversity Malaya's Dental Sciences ResearchNo ratings yet
- Characteristics and Distribution of Dental Anomalies in Patients with CleftDocument9 pagesCharacteristics and Distribution of Dental Anomalies in Patients with CleftcareNo ratings yet
- Efek Hypophospatasia Terhadap Gigi PermanenDocument6 pagesEfek Hypophospatasia Terhadap Gigi PermanenHafra AminiNo ratings yet
- Pnas.201316052 - Mandibal Variayion and The Categorization of Anthropologixal ManDocument6 pagesPnas.201316052 - Mandibal Variayion and The Categorization of Anthropologixal ManPGIndikaNo ratings yet
- Unlocking The Past: The Role of Dental Analysis in ArchaeologyDocument13 pagesUnlocking The Past: The Role of Dental Analysis in ArchaeologyaliinacristinaNo ratings yet
- HypoplasiaDocument7 pagesHypoplasiaSOMVIR KUMARNo ratings yet
- Early Development of The Lower Deciduous Dentition and Oral Vestibule in Human EmbryosDocument9 pagesEarly Development of The Lower Deciduous Dentition and Oral Vestibule in Human EmbryosMaria IvanaNo ratings yet
- Cysts of The Jaws in Pediatric Population: A 12-Year Institutional StudyDocument6 pagesCysts of The Jaws in Pediatric Population: A 12-Year Institutional StudyAndreas SimamoraNo ratings yet
- Orthodontic Therapy and Gingival Recession, A Systematic Review PDFDocument15 pagesOrthodontic Therapy and Gingival Recession, A Systematic Review PDFJose CollazosNo ratings yet
- Dentoskeletal Features Associated With Unilateral or Bilateral Palatal Displacement of Maxillary CaninesDocument8 pagesDentoskeletal Features Associated With Unilateral or Bilateral Palatal Displacement of Maxillary Canineskh jhNo ratings yet
- stone age mans dentition3 ajo1954Document14 pagesstone age mans dentition3 ajo1954BeniyaNo ratings yet
- Tooth Damage in Captive Orcas (Orcinus Orca)Document10 pagesTooth Damage in Captive Orcas (Orcinus Orca)Jeffrey Ventre MD DC0% (1)
- Teeth, Genes, and GenealogyDocument4 pagesTeeth, Genes, and GenealogyPablo BenitezNo ratings yet
- 2011 On The Evolution of Human Jaws and Teeth A ReviewDocument11 pages2011 On The Evolution of Human Jaws and Teeth A ReviewbaridinoNo ratings yet
- Crombie2009, Aetiology of Molar-Incisor Hypomineralization A Critical ReviewDocument11 pagesCrombie2009, Aetiology of Molar-Incisor Hypomineralization A Critical ReviewMairen RamirezNo ratings yet
- Pre Eruptive Intracoronal ResortionDocument5 pagesPre Eruptive Intracoronal ResortionAndres Mera VergaraNo ratings yet
- Hipoplasia EstatusDocument15 pagesHipoplasia EstatusAleida Cetina BastidaNo ratings yet
- Dental Age Estimation Methods for PaleodontologyDocument6 pagesDental Age Estimation Methods for PaleodontologyMeris JugadorNo ratings yet
- Multifactorial Etiology of Torus Mandibularis: Study of TwinsDocument6 pagesMultifactorial Etiology of Torus Mandibularis: Study of TwinskcsaputraNo ratings yet
- Pone 0080771Document10 pagesPone 0080771Wilmer Yanquen VillarrealNo ratings yet
- 10 0000@m Pnas Org@m@early@2017@09@19@1708023114Document6 pages10 0000@m Pnas Org@m@early@2017@09@19@1708023114DaviydNo ratings yet
- Etiology of Maxillary Canine Impaction A ReviewDocument11 pagesEtiology of Maxillary Canine Impaction A ReviewMiltonfcc100% (1)
- AJPA 2010 Alqahtani Atlas of Human Tooth DevelopmentDocument10 pagesAJPA 2010 Alqahtani Atlas of Human Tooth DevelopmentRodrigo MictlanNo ratings yet
- Periodontology 2000 La Controversia Endodoncia PeriodonciaDocument8 pagesPeriodontology 2000 La Controversia Endodoncia PeriodonciaEdos De la Barra100% (2)
- Prevalence of Enamel Pearls in Teeth From A Human Teeth BankDocument4 pagesPrevalence of Enamel Pearls in Teeth From A Human Teeth BankDoddy KondarNo ratings yet
- Roentgenographic StudyDocument15 pagesRoentgenographic StudyAndres CoboNo ratings yet
- Forensic Dentistry Final Report on Dental Identification MethodsDocument5 pagesForensic Dentistry Final Report on Dental Identification Methodsزيد العراقيNo ratings yet
- The Prevalence and Distribution of Dental Caries in Four Early Medieval Non-Adult Populations of Different Socioeconomic Status From Central EuropeDocument1 pageThe Prevalence and Distribution of Dental Caries in Four Early Medieval Non-Adult Populations of Different Socioeconomic Status From Central EuropeSOMVIR KUMARNo ratings yet
- Review ArticleDocument14 pagesReview Article謎超人No ratings yet
- Genetic Basis of Tooth AgenesisDocument23 pagesGenetic Basis of Tooth Agenesissümeyra akkoçNo ratings yet
- DA Vol 19 3Document36 pagesDA Vol 19 3Silvana Flores CastilloNo ratings yet
- Gingival Recession: P. J. C. WatsonDocument7 pagesGingival Recession: P. J. C. WatsonPerla Cristina Rios RiosNo ratings yet
- 424-Article Text-1272-1-11-20170906Document13 pages424-Article Text-1272-1-11-20170906Ortodoncia UNAL 2020No ratings yet
- Enamel Defects in Permanent First Molars and Incisors in Individuals With Cleft Lip And/or PalateDocument5 pagesEnamel Defects in Permanent First Molars and Incisors in Individuals With Cleft Lip And/or PalatefatimahNo ratings yet
- SCANNING ELECTRON MICROSCOPIC STUDY OF AMELOGENESIS IMPERFECTA (SEM OF AIDocument12 pagesSCANNING ELECTRON MICROSCOPIC STUDY OF AMELOGENESIS IMPERFECTA (SEM OF AIRatheesh Kumar SNo ratings yet
- stone age mans dentition2 ajo1954Document11 pagesstone age mans dentition2 ajo1954BeniyaNo ratings yet
- Dental Crowing and Its Relationship To Mesiodistal Crown Diameters and Arch DimensionsDocument7 pagesDental Crowing and Its Relationship To Mesiodistal Crown Diameters and Arch DimensionsMafe SalazarNo ratings yet
- Etiology, Diagnosis, Consequences and Treatment of Infraoccluded Primary MolarsDocument6 pagesEtiology, Diagnosis, Consequences and Treatment of Infraoccluded Primary MolarsEvelin CastilloNo ratings yet
- Sexual Dimorphism in Permanent Teeth of Modern GreeksDocument8 pagesSexual Dimorphism in Permanent Teeth of Modern GreeksPutri Zeahan Ramadhini YedismanNo ratings yet
- Palubeckaite Etal 06Document11 pagesPalubeckaite Etal 06Sol Plaza VareaNo ratings yet
- Development of The Curve of SpeeDocument9 pagesDevelopment of The Curve of SpeeMirnaLizNo ratings yet
- Oral Myofunctional and Articulation Disorders in Children With Malocclusions - A Systematic ReviewDocument16 pagesOral Myofunctional and Articulation Disorders in Children With Malocclusions - A Systematic Reviewalba farran martiNo ratings yet
- stone age mans dentition1 ajo1954Document15 pagesstone age mans dentition1 ajo1954BeniyaNo ratings yet
- Racial Characteristics of Human Teeth With Special Emphasis On The Mongoloid DentitionDocument7 pagesRacial Characteristics of Human Teeth With Special Emphasis On The Mongoloid DentitionRidwan FajiriNo ratings yet
- Vast Ardis 2000Document7 pagesVast Ardis 2000ludovicoNo ratings yet
- The Genetics of Human Tooth AgenesisDocument7 pagesThe Genetics of Human Tooth Agenesissümeyra akkoçNo ratings yet
- Prevalence of malocclusion in Chinese youthDocument8 pagesPrevalence of malocclusion in Chinese youthLuis SarmientoNo ratings yet
- Updated Guidelines To The Standards For Recording Human RemainsDocument66 pagesUpdated Guidelines To The Standards For Recording Human RemainsDarlene WestonNo ratings yet
- Backwell & D'ericco 2001-Swartkrans-TermitiDocument6 pagesBackwell & D'ericco 2001-Swartkrans-TermitiMarija KreckovicNo ratings yet
- A 017627Document8 pagesA 017627Marija KreckovicNo ratings yet
- Parcak, Site Survey in EgyptologyDocument24 pagesParcak, Site Survey in EgyptologyMarija KreckovicNo ratings yet
- Tree Ring DatingDocument33 pagesTree Ring DatingMarija KreckovicNo ratings yet
- 3 B. Holly Broadbent October, 94: YR. YR. YRDocument4 pages3 B. Holly Broadbent October, 94: YR. YR. YRAlberto MinanoNo ratings yet
- Extraction ForcepsDocument3 pagesExtraction ForcepsShift UallNo ratings yet
- Good Occlusal Practice in Restorative DentistryDocument3 pagesGood Occlusal Practice in Restorative DentistryCarmen Breban CirțiuNo ratings yet
- Methods of Gaining SpaceDocument25 pagesMethods of Gaining SpaceMaitreyi LimayeNo ratings yet
- Discussion of Begg's Attritional Occlusion Vol 11 No 3 Mar 1990Document5 pagesDiscussion of Begg's Attritional Occlusion Vol 11 No 3 Mar 1990Saravanan KanagavelNo ratings yet
- Development and Morphology of The Primary TeethDocument86 pagesDevelopment and Morphology of The Primary Teethceudmd3dNo ratings yet
- Ideal For Combined Restorations Vivid Individual Esthetics: Neo - LignDocument6 pagesIdeal For Combined Restorations Vivid Individual Esthetics: Neo - LignDumitru CrîşmariNo ratings yet
- Mandibular Second Premolar AnatomyDocument13 pagesMandibular Second Premolar Anatomyxmarty.fazilNo ratings yet
- Permanent Mandibular Lateral IncisorsDocument2 pagesPermanent Mandibular Lateral IncisorsSafura IjazNo ratings yet
- BP DevelopdentitionDocument18 pagesBP DevelopdentitionShakh ShakhNo ratings yet
- Premolar Root Number Variation in Hominoids: Genetic Polymorphism vs. Functional SignificanceDocument12 pagesPremolar Root Number Variation in Hominoids: Genetic Polymorphism vs. Functional SignificanceDarshilNo ratings yet
- Rehabilitative and Esthetics Dentistry: Case 1: PedoDocument101 pagesRehabilitative and Esthetics Dentistry: Case 1: PedoMauriceNo ratings yet
- Conservative Restoration of The Worn Dentition - The Anatomically Driven Direct Approach (ADA)Document34 pagesConservative Restoration of The Worn Dentition - The Anatomically Driven Direct Approach (ADA)Jessi RecaldeNo ratings yet
- Giulian 1 TradusDocument5 pagesGiulian 1 TradusGiulian SabinNo ratings yet
- SK Tim Teknis PPK 2019-1Document24 pagesSK Tim Teknis PPK 2019-1MargaNo ratings yet
- 1 - Kanno - J Oral Rehab - 2006 CópiaDocument13 pages1 - Kanno - J Oral Rehab - 2006 CópiaYvelisse LoraNo ratings yet
- Occlusal Consideration For Mandibular Implant OverdenturesDocument12 pagesOcclusal Consideration For Mandibular Implant OverdenturesFrancisca Dinamarca Lama100% (1)