You might also like
- Severe Fungal Cervicofacial Cellulitis From Otogenic Mucuromycosis Origin A Case ReportDocument4 pagesSevere Fungal Cervicofacial Cellulitis From Otogenic Mucuromycosis Origin A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Malignant Otitis External: Our ExperienceDocument4 pagesMalignant Otitis External: Our ExperienceSuci PramadianiNo ratings yet
- Jurnal P.acnesDocument4 pagesJurnal P.acnesFazlicha SyaradilaNo ratings yet
- PDIA Art 17695-10Document6 pagesPDIA Art 17695-10faniaNo ratings yet
- Rhinocerebral Mucormycosis Case ReportDocument3 pagesRhinocerebral Mucormycosis Case ReportYani ManuelNo ratings yet
- Pi Is 0278239103007407Document5 pagesPi Is 0278239103007407tengoplatita2008No ratings yet
- Case ReportDocument5 pagesCase Reportyudhi kurniawanNo ratings yet
- Case Report: Mucormycosis of Mandible With Unfavorable OutcomeDocument5 pagesCase Report: Mucormycosis of Mandible With Unfavorable OutcomeDr.Sudarsan SenNo ratings yet
- Post Covid 19 Mucoromycosis of MandibleDocument5 pagesPost Covid 19 Mucoromycosis of MandibleDr Yamuna RaniNo ratings yet
- MUCORMYCOSISDocument4 pagesMUCORMYCOSISipe.jacobNo ratings yet
- World Journal of Oral and Maxillofacial SurgeryDocument4 pagesWorld Journal of Oral and Maxillofacial SurgeryRemedyPublication3No ratings yet
- Rhino Maxillary Mucormycosis During The Covid-19 Third Wave A Case ReportDocument4 pagesRhino Maxillary Mucormycosis During The Covid-19 Third Wave A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Oral Management of Idiopathic Thrombocytopenic Purpura Patient: Case ReportDocument5 pagesOral Management of Idiopathic Thrombocytopenic Purpura Patient: Case ReportNauroh NaurohNo ratings yet
- Mucormycosis of The Hard Palate A Case ReportDocument3 pagesMucormycosis of The Hard Palate A Case ReportrgumralNo ratings yet
- Pragesh Mucor ArticalDocument6 pagesPragesh Mucor ArticalShobhitNo ratings yet
- Proptosis UnilateralDocument5 pagesProptosis UnilateralCarlos NiveloNo ratings yet
- TMP 103 EDocument4 pagesTMP 103 EFrontiersNo ratings yet
- Acute Fungal Sinusitis Natural History and The Role of Frozen SectionDocument8 pagesAcute Fungal Sinusitis Natural History and The Role of Frozen SectionwitariNo ratings yet
- Jced 9 E319Document6 pagesJced 9 E319sorayahyuraNo ratings yet
- 108 Orbitorhinocerebral MucormycosisDocument10 pages108 Orbitorhinocerebral MucormycosisrgumralNo ratings yet
- Jurnal BM 2Document6 pagesJurnal BM 2Husnul KhatimahNo ratings yet
- Ajmcr 10 1 1Document4 pagesAjmcr 10 1 1jghcl.221No ratings yet
- Challenging Diagnosis of Kimura Disease in A Child With Nephrotic Syndrome: A Case ReportDocument5 pagesChallenging Diagnosis of Kimura Disease in A Child With Nephrotic Syndrome: A Case ReportTalbiya mullaNo ratings yet
- Artigo Neuromeningeal Cryptococcosis in A Patient Not Infected With HumanDocument4 pagesArtigo Neuromeningeal Cryptococcosis in A Patient Not Infected With HumanRENATA SANTOS ASSUNCAONo ratings yet
- Autoimmune Diseases A Late Complication of Toxic Epidermal Necrolysis A Case ReportDocument4 pagesAutoimmune Diseases A Late Complication of Toxic Epidermal Necrolysis A Case ReportAthenaeum Scientific PublishersNo ratings yet
- Necrotizing Fasciitis of The Breast: A Case Series and Review of The LiteratureDocument9 pagesNecrotizing Fasciitis of The Breast: A Case Series and Review of The LiteratureElli SymeonidouNo ratings yet
- C CA AS SC CL Liin Niiq QU UE E // C CA AS SE ER RE EP PO OR RT TDocument7 pagesC CA AS SC CL Liin Niiq QU UE E // C CA AS SE ER RE EP PO OR RT TG Virucha Meivila IINo ratings yet
- A Tuzcu M Bahceci MK Celen N Kilinc S Ozmen: Correspondence AddressDocument4 pagesA Tuzcu M Bahceci MK Celen N Kilinc S Ozmen: Correspondence AddressiqbaladiNo ratings yet
- mainDocument3 pagesmainomidazadmehr1375No ratings yet
- Staphylococcus Epidermidis End PDFDocument4 pagesStaphylococcus Epidermidis End PDFNisaNo ratings yet
- Jurnal SinusitisDocument6 pagesJurnal SinusitisNurul Aisyah PaldarNo ratings yet
- Necrotizing Soft Tissue Infection: Clinical Characteristics and Outcomes at A Reconstructive Center in Jilin ProvinceDocument8 pagesNecrotizing Soft Tissue Infection: Clinical Characteristics and Outcomes at A Reconstructive Center in Jilin Provincesyak turNo ratings yet
- Ejm 17 1 40 45Document6 pagesEjm 17 1 40 45Ujean Santos SagaralNo ratings yet
- Apeced Syndrome (Family Observation)Document5 pagesApeced Syndrome (Family Observation)IJAR JOURNALNo ratings yet
- Inflammatory Choroidal NeovascularizationDocument7 pagesInflammatory Choroidal NeovascularizationMarj MendezNo ratings yet
- DiagnosisDocument4 pagesDiagnosisDiana RizkiNo ratings yet
- Cervical Necrotizing Fasciitis in Children Under Two Years of AgeDocument4 pagesCervical Necrotizing Fasciitis in Children Under Two Years of AgedenmasasinggihNo ratings yet
- American Journal of Ophthalmology Case Reports: Chad Y. Lewis, Michael E. Zegans, Nikhil N. Batra, Kelsey L. JordanDocument6 pagesAmerican Journal of Ophthalmology Case Reports: Chad Y. Lewis, Michael E. Zegans, Nikhil N. Batra, Kelsey L. JordanAishah FarihaNo ratings yet
- 2012 VideoDocument4 pages2012 VideoNur LaelaNo ratings yet
- Department of Health and Family Welfare Govt. of West BengalDocument35 pagesDepartment of Health and Family Welfare Govt. of West Bengalswagato deyNo ratings yet
- 8 Pseudocyst of Pinna and Its Treatment With Surgical Deroofing - An Experience at Tertiary Hospitals 2013Document13 pages8 Pseudocyst of Pinna and Its Treatment With Surgical Deroofing - An Experience at Tertiary Hospitals 2013solikin ikinNo ratings yet
- International Journal of Dermatology and VenereologyDocument3 pagesInternational Journal of Dermatology and VenereologyCuiting FengNo ratings yet
- Management of Unsafe Type of Chronic Suppurative Otitis Media With Extracranial Complications at A Tertiary Care CenterDocument6 pagesManagement of Unsafe Type of Chronic Suppurative Otitis Media With Extracranial Complications at A Tertiary Care CenterLarasati Gilang Fuzi AstutiNo ratings yet
- Neck Pain and Rash in an 18-Year-Old StudentDocument5 pagesNeck Pain and Rash in an 18-Year-Old StudentRahul K. JagaNo ratings yet
- A Rapidly Progressive Case of Skin and Soft Tissues Necrosis in A COVID 19 Positive PatientDocument9 pagesA Rapidly Progressive Case of Skin and Soft Tissues Necrosis in A COVID 19 Positive PatientAthenaeum Scientific PublishersNo ratings yet
- Feridas Difícil CicatrizaçãoDocument22 pagesFeridas Difícil CicatrizaçãoBia BerzotiNo ratings yet
- Medical Mycology Case Reports: SciencedirectDocument5 pagesMedical Mycology Case Reports: SciencedirectDr.Sudarsan SenNo ratings yet
- Sino-Orbital Mucormycosis in A COVID-19 Patient: A Case ReportDocument5 pagesSino-Orbital Mucormycosis in A COVID-19 Patient: A Case Reportkarol castellonNo ratings yet
- Staphylococcal Scalded Skin Syndrome in Child A CADocument6 pagesStaphylococcal Scalded Skin Syndrome in Child A CAsalshabilaNo ratings yet
- Chen 2018Document5 pagesChen 2018Teja Laksana NukanaNo ratings yet
- FLOPPYEYELID2020Document4 pagesFLOPPYEYELID2020Karina BudijantoNo ratings yet
- 10 5923 J Surgery 20130204 01 PDFDocument3 pages10 5923 J Surgery 20130204 01 PDFAndreas NatanNo ratings yet
- Necrotising FascitisDocument8 pagesNecrotising FascitisKartikey ChauhanNo ratings yet
- Observations On Time Course Changes of The CherryDocument16 pagesObservations On Time Course Changes of The CherryAndi Tiara S. AdamNo ratings yet
- Jaad O: NlineDocument2 pagesJaad O: NlinepunishNo ratings yet
- Concurrent Basal Cell and Squamous Cell Carcinomas Associated With Hydroxyurea TherapyDocument4 pagesConcurrent Basal Cell and Squamous Cell Carcinomas Associated With Hydroxyurea Therapyanisse89No ratings yet
- An Institutional Study On Covid-19 Associated Rhino-Orbital-Cerebral MucormycosisDocument8 pagesAn Institutional Study On Covid-19 Associated Rhino-Orbital-Cerebral MucormycosisIJAR JOURNALNo ratings yet
- Penetrating Keratoplasty in Active Acanthamoeba KeratitisDocument5 pagesPenetrating Keratoplasty in Active Acanthamoeba Keratitisdrvishalkulkarni2007No ratings yet
- Age-Related Macular Degeneration: Current Treatment ConceptsFrom EverandAge-Related Macular Degeneration: Current Treatment ConceptsW.E. AlbertiNo ratings yet
- Facial Soft Tissue Thickness Among ThreeSkeletal Classes in Adult Pakistani SubjectsDocument7 pagesFacial Soft Tissue Thickness Among ThreeSkeletal Classes in Adult Pakistani Subjectstoffe lopezNo ratings yet
- 2.orthodontics OrganogramDocument1 page2.orthodontics OrganogramWaqar JeelaniNo ratings yet
- Cippchecklist Mar07Document16 pagesCippchecklist Mar07Jocelyn Lopez CaihuanNo ratings yet
- C4 AnnexureDocument10 pagesC4 AnnexureWaqar JeelaniNo ratings yet
- Transfer of Motor VehicleDocument1 pageTransfer of Motor VehicleWaqar JeelaniNo ratings yet
- Car Loan Buyer Seller AgreementDocument1 pageCar Loan Buyer Seller AgreementWaqar JeelaniNo ratings yet
- RoutledgeHandbooks 9780203066201 Chapter3Document17 pagesRoutledgeHandbooks 9780203066201 Chapter3Waqar JeelaniNo ratings yet
- Twinblockshilpa 170129085958 PDFDocument130 pagesTwinblockshilpa 170129085958 PDFWaqar JeelaniNo ratings yet
- The Generics Pharmacy Philippines Case StudyDocument20 pagesThe Generics Pharmacy Philippines Case StudyYna Peregrino38% (8)
- Lesson VI: Semi-Solid Dosage Form of PreparationsDocument27 pagesLesson VI: Semi-Solid Dosage Form of PreparationsEleanorNo ratings yet
- Bahasa Inggris Swot Madam Gie Sweet Cheek BlushedDocument8 pagesBahasa Inggris Swot Madam Gie Sweet Cheek Blushedanon_681594518No ratings yet
- Developing Methodology For Evaluating The Ability of Indoor Materials To Support Microbial Growth Using Static Environmental ChambersDocument6 pagesDeveloping Methodology For Evaluating The Ability of Indoor Materials To Support Microbial Growth Using Static Environmental ChambersEugene GudimaNo ratings yet
- 28 CryptorchidismDocument23 pages28 CryptorchidismFaisal Ibn MushtaqNo ratings yet
- Fans Instructions CE (A015)Document72 pagesFans Instructions CE (A015)vasaNo ratings yet
- Ion Breeding Policy - 2006 & 2010Document42 pagesIon Breeding Policy - 2006 & 2010Ulhas GaikwadNo ratings yet
- Isu Dan Etika Pada Perawatan Paliatif PDFDocument17 pagesIsu Dan Etika Pada Perawatan Paliatif PDFNatasya ChieCaem FunforeverNo ratings yet
- Minimizing The Risk of Alzheimer S DiseaseDocument328 pagesMinimizing The Risk of Alzheimer S DiseaseLuis Raudales100% (1)
- Hematoma: HaematomaDocument3 pagesHematoma: HaematomaBeeBeeSethNo ratings yet
- Moth Balls: Safety Data SheetDocument9 pagesMoth Balls: Safety Data SheethafilrediandikaNo ratings yet
- Rhomboid Flap For Pilonidal Sinus - Our ExperienceDocument5 pagesRhomboid Flap For Pilonidal Sinus - Our ExperienceKhalidHussainNo ratings yet
- Why Is Research Important - NHS GroupDocument8 pagesWhy Is Research Important - NHS GroupRoxan PacsayNo ratings yet
- Psychological Communication Barriers PosterDocument1 pagePsychological Communication Barriers PostereliyaziyaNo ratings yet
- Periodontal Accelerated Osteogenic OrthodonticsDocument6 pagesPeriodontal Accelerated Osteogenic Orthodonticsyui cherryNo ratings yet
- Pengembangan Model Kepribadian Konselor Efektif Berbasis Budaya Siri' Na PesseDocument9 pagesPengembangan Model Kepribadian Konselor Efektif Berbasis Budaya Siri' Na PesseTjatur SurantullohNo ratings yet
- WCLC2017 Abstract Book WebDocument700 pagesWCLC2017 Abstract Book Webdavid.yb.wangNo ratings yet
- Bromine Water SafetyDocument5 pagesBromine Water SafetyWinonaNo ratings yet
- Michael Simonov CVDocument2 pagesMichael Simonov CVAnonymous QioCrCEVNo ratings yet
- Data Legacy InsuranceCos SourceRSDocument48 pagesData Legacy InsuranceCos SourceRSrishu1527No ratings yet
- House Bill 15-1043Document19 pagesHouse Bill 15-1043Michael_Lee_RobertsNo ratings yet
- Approval Romania 2008Document27 pagesApproval Romania 2008Andrés Domínguez RuizNo ratings yet
- Aliza Updated ResumeDocument2 pagesAliza Updated Resumeapi-359939852No ratings yet
- Open Versus Closed Kinetic Chain Exercises For Patellofemoral Pain Syndrome - TsaiDocument44 pagesOpen Versus Closed Kinetic Chain Exercises For Patellofemoral Pain Syndrome - TsaiBaykal Çelik100% (1)
- Vancomycin DRUGSTUDYDocument3 pagesVancomycin DRUGSTUDYEmagra AzilNo ratings yet
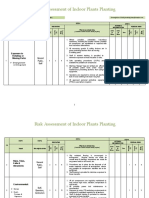
- Risk Assessment of Indoor Plants PlantingDocument5 pagesRisk Assessment of Indoor Plants Plantingطارق رضوانNo ratings yet
- Introducing Behavioural Markers of Non-Technical Skills in Oil and Gas OperationsDocument24 pagesIntroducing Behavioural Markers of Non-Technical Skills in Oil and Gas OperationsMarutpal MukherjeeNo ratings yet
- The Legal Bases of Special EducationDocument14 pagesThe Legal Bases of Special EducationMaria Dulcinea Basbas86% (7)
- Suplemento 1Document56 pagesSuplemento 1Dessirhe LaraNo ratings yet
- Norma Ashrae 62 1989Document3 pagesNorma Ashrae 62 1989Mittzi CallejasNo ratings yet