You might also like
- MetabolicRenewal FemaleFlatBellyDocument13 pagesMetabolicRenewal FemaleFlatBellyDiana Parracho100% (12)
- Apemilast: Apremilast INNDocument1 pageApemilast: Apremilast INNerfan alamNo ratings yet
- Drug StudyyDocument5 pagesDrug StudyyKiana Garlitos CasasNo ratings yet
- Pediatric Pharmacotherapy3Document1 pagePediatric Pharmacotherapy3DrNoor MD MohsenNo ratings yet
- Practice 1Document25 pagesPractice 1Bro BroNo ratings yet
- Indever PDFDocument4 pagesIndever PDFbiddut95No ratings yet
- Treatment of MalariaDocument49 pagesTreatment of MalariaShanza AmaanNo ratings yet
- Motilium PIDocument12 pagesMotilium PIKok Foo YipNo ratings yet
- Pyramax Product Information - enDocument53 pagesPyramax Product Information - enonen patoNo ratings yet
- Migraine in Emergency Update DR Tanjim OveeDocument2 pagesMigraine in Emergency Update DR Tanjim OveeAHMED TANJIMUL ISLAMNo ratings yet
- Chapter 2Document34 pagesChapter 2zaidhusam100% (2)
- Migraine - Acute ManagementDocument48 pagesMigraine - Acute ManagementMohan PrasadNo ratings yet
- Management of Migraine (With or Without Aura) Management of Migraine (With or Without Aura)Document12 pagesManagement of Migraine (With or Without Aura) Management of Migraine (With or Without Aura)mehakNo ratings yet
- Apremilast PI Europe Aug 2019Document14 pagesApremilast PI Europe Aug 2019Wei Sheng ChongNo ratings yet
- MethergineDocument3 pagesMethergineJohn AlanoNo ratings yet
- Psych DrugsDocument6 pagesPsych DrugsdianneingusanNo ratings yet
- Toxicity: Onitoring OF HerapyDocument1 pageToxicity: Onitoring OF HerapyDrNoor MD MohsenNo ratings yet
- Treatment of Migraine Attacks and Prevention of MiDocument40 pagesTreatment of Migraine Attacks and Prevention of MiHemi Amalia AmirullahNo ratings yet
- Decidex Compuesto: Clorfenamina / Pseudoefedrina / ParacetamolDocument2 pagesDecidex Compuesto: Clorfenamina / Pseudoefedrina / ParacetamolEmanuel mOmoNo ratings yet
- Product Guide 2015Document269 pagesProduct Guide 2015Joy loboNo ratings yet
- Rishum 3 03821017Document22 pagesRishum 3 03821017moiseancuta87No ratings yet
- Antispastics Emtyaz FDocument57 pagesAntispastics Emtyaz FMuhammed MuhsinNo ratings yet
- 970 PDFDocument4 pages970 PDFFibiaka AlgebriNo ratings yet
- Myasthenia Gravis: Association of British Neurologists' Management GuidelinesDocument14 pagesMyasthenia Gravis: Association of British Neurologists' Management Guidelinesafm26No ratings yet
- LPD - Myrin P Forte (Pakistan)Document17 pagesLPD - Myrin P Forte (Pakistan)Azeem Abbas0% (1)
- Manual Farma 2Document10 pagesManual Farma 2Fernanda Roldán CastañedaNo ratings yet
- 1) Selective Serotonin Reuptic Inhepetor (SSRI) - Xetine: Fluoxetine, Paroxetine, Sertraline, DoluexitineDocument13 pages1) Selective Serotonin Reuptic Inhepetor (SSRI) - Xetine: Fluoxetine, Paroxetine, Sertraline, DoluexitineSEIYADU IBRAHIM KNo ratings yet
- Aprepitant - 125mg CapsuleDocument9 pagesAprepitant - 125mg CapsuleMd. Abdur RahmanNo ratings yet
- 4.7.4 Antimigraine DrugsDocument2 pages4.7.4 Antimigraine DrugsaldriansilverNo ratings yet
- Pizotifen MalateDocument2 pagesPizotifen MalatesadafNo ratings yet
- Lim Drug StudyDocument7 pagesLim Drug StudyKhovianna LimNo ratings yet
- Cardiology ReviewDocument24 pagesCardiology ReviewAmna KhanNo ratings yet
- Primaquine: Phosphate Tablets, UspDocument6 pagesPrimaquine: Phosphate Tablets, UspEphenk PunkNo ratings yet
- Reference: Chapter 47. Basic and Clinical Pharmacology - 13th Edition. Katzung and Trevor. Lec GuideDocument8 pagesReference: Chapter 47. Basic and Clinical Pharmacology - 13th Edition. Katzung and Trevor. Lec GuideselflessdoctorNo ratings yet
- Migraine: By: B K PandaDocument19 pagesMigraine: By: B K PandapandabijoyNo ratings yet
- Paracetamol - Fresenius 10mg - MLDocument3 pagesParacetamol - Fresenius 10mg - MLainia taufiqaNo ratings yet
- Allersin Syrup/ F Tablet: Amended Package InsertDocument1 pageAllersin Syrup/ F Tablet: Amended Package Insertraul sinatoNo ratings yet
- Perjeta Epar Product Information - enDocument43 pagesPerjeta Epar Product Information - enGeo GeoNo ratings yet
- Susten MedicineDocument1 pageSusten MedicineAdnan TowfiqueNo ratings yet
- Topiramate (Topamax) For Migraine Prevention - NPS MedicineWiseDocument7 pagesTopiramate (Topamax) For Migraine Prevention - NPS MedicineWiserobouNo ratings yet
- Anadol 1Document3 pagesAnadol 1jmohideenkadharNo ratings yet
- Tramadol Hydrochloride + Paracetamol: 37.5 MG / 325 MG Film-Coated TABLET Analgesic ™algesiaDocument7 pagesTramadol Hydrochloride + Paracetamol: 37.5 MG / 325 MG Film-Coated TABLET Analgesic ™algesiaNikkae AngobNo ratings yet
- Clomipramine PDFDocument18 pagesClomipramine PDFddandan_2No ratings yet
- Acute Treatment of Migraine in Adults - UpToDateDocument42 pagesAcute Treatment of Migraine in Adults - UpToDateSebas MontoyaNo ratings yet
- Drug Review-Tramadol.: Journal of The Institute of Medicine December 2006Document6 pagesDrug Review-Tramadol.: Journal of The Institute of Medicine December 2006NINDYA PRASTIWINo ratings yet
- Ketamine Guidelines Feb 05Document3 pagesKetamine Guidelines Feb 05AdiAri RosiuNo ratings yet
- Dextroamphetamine: Brand Name: DexedrineDocument23 pagesDextroamphetamine: Brand Name: DexedrineSharry Fe OasayNo ratings yet
- Dextroamphetamine: Brand Name: DexedrineDocument23 pagesDextroamphetamine: Brand Name: DexedrineSharry Fe OasayNo ratings yet
- Otezla 10 MG Film-Coated Tablets: 1. Name of The Medicinal ProductDocument22 pagesOtezla 10 MG Film-Coated Tablets: 1. Name of The Medicinal ProductSunil SewakNo ratings yet
- Otezla 10 MG Film-Coated Tablets: 1. Name of The Medicinal ProductDocument22 pagesOtezla 10 MG Film-Coated Tablets: 1. Name of The Medicinal ProductSunil SewakNo ratings yet
- Core Safety ProfileDocument6 pagesCore Safety ProfilexepayahNo ratings yet
- Drug StudyDocument4 pagesDrug Studyhernandezquennee0701No ratings yet
- 01-Tramadol Guidelines PDFDocument1 page01-Tramadol Guidelines PDFDina Aulia FakhrinaNo ratings yet
- NAVELBINE 20 MG, 30mg CapsulesDocument2 pagesNAVELBINE 20 MG, 30mg Capsulesddandan_2No ratings yet
- Pdoc - Susten DSDocument1 pagePdoc - Susten DSRaisha EasinNo ratings yet
- Ondansetron - Cahulogan, JPDocument9 pagesOndansetron - Cahulogan, JPpearl japsonNo ratings yet
- APRANAXDocument2 pagesAPRANAXAmy PainterNo ratings yet
- Paracetamol Package InsertDocument1 pageParacetamol Package InsertEryll Paolo Alea100% (1)
- Medicine Guideline - ParacetamolDocument9 pagesMedicine Guideline - ParacetamolAbu Mejza'atNo ratings yet
- Oseltamivir (Tamiflu)Document17 pagesOseltamivir (Tamiflu)asdwasdNo ratings yet
- Aqualisa Brochure January 2019Document57 pagesAqualisa Brochure January 2019stewartNo ratings yet
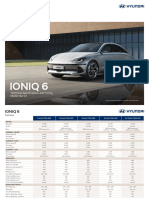
- Brochure Ioniq6 Price and SpecDocument10 pagesBrochure Ioniq6 Price and SpecstewartNo ratings yet
- Bar MenuDocument1 pageBar MenustewartNo ratings yet
- Christmas Day Lunch 2022 MenuDocument1 pageChristmas Day Lunch 2022 MenustewartNo ratings yet
- CANH Full GuidanceDocument100 pagesCANH Full GuidancestewartNo ratings yet
- Group No 5Document6 pagesGroup No 5Isaac Samson Ayeng'oNo ratings yet
- iADH Develops An Undergraduate Curriculum in Special Care Dentistry - JCDADocument3 pagesiADH Develops An Undergraduate Curriculum in Special Care Dentistry - JCDAMOHD ISYRAFUDDIN ISMAILNo ratings yet
- Rule of Ayurvedic Formation in Management of Ashmari A Case StudyDocument6 pagesRule of Ayurvedic Formation in Management of Ashmari A Case StudyEditor IJTSRDNo ratings yet
- As Dda Mile DFD StonesDocument2 pagesAs Dda Mile DFD StonesffffffffNo ratings yet
- HSE Report On Electrical Incidents Rr842Document146 pagesHSE Report On Electrical Incidents Rr842Chris ParkinsonNo ratings yet
- Ideas For IELTS WritingDocument154 pagesIdeas For IELTS WritingTRAN AN KHANHNo ratings yet
- Neurotic (Psychoneurotic) BehaviorsDocument2 pagesNeurotic (Psychoneurotic) BehaviorsNoelyn Natarte LuadNo ratings yet
- SG4 - Group Project OM - ENTREE 19Document10 pagesSG4 - Group Project OM - ENTREE 19Raymond Yonathan HutapeaNo ratings yet
- ADEA EssaysDocument6 pagesADEA EssaysprasantiNo ratings yet
- Edited TITLE TO FIRST PAGE of RATIONALE Second TimeDocument12 pagesEdited TITLE TO FIRST PAGE of RATIONALE Second TimeSimplicio Gadugdug VNo ratings yet
- Unit 1 - Nature of PsychologyDocument6 pagesUnit 1 - Nature of PsychologyJomyl Amador PetracortaNo ratings yet
- Research CriminologyDocument27 pagesResearch CriminologyChloie Marie RosalejosNo ratings yet
- Program Planning and Proposal WritingDocument5 pagesProgram Planning and Proposal Writingcarolsmith1957No ratings yet
- Action Plan 2018 - 2020 Without ExpensesDocument10 pagesAction Plan 2018 - 2020 Without Expensesapi-238795410No ratings yet
- Nowadays Food Has Become Easier To PrepareDocument11 pagesNowadays Food Has Become Easier To PrepareDirshan Kumar Gurnani100% (1)
- Components of Food Class 6thDocument2 pagesComponents of Food Class 6thSantoshPathakNo ratings yet
- HOSPITAL MANAGEMENT SYSTEMS AND Patients Records ManagementDocument35 pagesHOSPITAL MANAGEMENT SYSTEMS AND Patients Records Managementokello100% (1)
- Beamotil Tablet Information LeafletDocument3 pagesBeamotil Tablet Information Leafletadam malikNo ratings yet
- 1st Lecture - Cestodes - Clinical ParasitologyDocument29 pages1st Lecture - Cestodes - Clinical ParasitologyAhmed MoghazyNo ratings yet
- She PlusDocument2 pagesShe PlusHarjinder SinghNo ratings yet
- Pendidikan, Pekerjaan Dan Pendapatan Terhadap Kejadian Lelaki Seks LelakiDocument7 pagesPendidikan, Pekerjaan Dan Pendapatan Terhadap Kejadian Lelaki Seks LelakiFeny WartisaNo ratings yet
- Literature Review On Stress Among College StudentsDocument5 pagesLiterature Review On Stress Among College StudentsaflssjrdaNo ratings yet
- Abdominal Trauma: Maria MayasariDocument35 pagesAbdominal Trauma: Maria MayasariDanus RamadanusNo ratings yet
- Social Determinants of HealthDocument13 pagesSocial Determinants of HealthEllen TNo ratings yet
- Materials. Atlanta, Georgia: U.S. Department of Health and Human ServicesDocument1 pageMaterials. Atlanta, Georgia: U.S. Department of Health and Human ServicesAnonymous l6Q1ROq2No ratings yet
- Obstetrical Emergency & ManagementDocument38 pagesObstetrical Emergency & ManagementDrPreeti Thakur ChouhanNo ratings yet
- Boots ROI Healthcare Assistant Programme Module 2 WorkbookDocument69 pagesBoots ROI Healthcare Assistant Programme Module 2 WorkbookevacawleyNo ratings yet
- NMC Hospital Abu Dhabi - 2011!06!08Document16 pagesNMC Hospital Abu Dhabi - 2011!06!08Manjul TakleNo ratings yet
- Research MethodologyDocument4 pagesResearch MethodologyPayal PurohitNo ratings yet