You might also like
- Chapter 14: Introduction To Health Promotion and Health Protection Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionDocument2 pagesChapter 14: Introduction To Health Promotion and Health Protection Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionHelen UgochukwuNo ratings yet
- Nursing Informatics in The Philippines - Past, Present, and FutureDocument5 pagesNursing Informatics in The Philippines - Past, Present, and FutureRea Rabi100% (1)
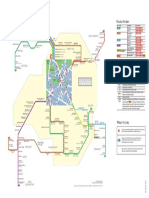
- TFL Spider Map For New ElthamDocument1 pageTFL Spider Map For New Elthamhrpwmv83No ratings yet
- Week 11Document1 pageWeek 11nikhilsolanki1127No ratings yet
- PVM Technical Design: - Stakeholders - Bpe - Product Owner - Support Team - Satellite SystemsDocument12 pagesPVM Technical Design: - Stakeholders - Bpe - Product Owner - Support Team - Satellite SystemsJayabharath SNo ratings yet
- Municipality of Cuyapo: 2nd QUARTER 2018Document2 pagesMunicipality of Cuyapo: 2nd QUARTER 2018badboiNo ratings yet
- ZTE 2G Handover Algorithm: Why Do We Need Handover ?Document37 pagesZTE 2G Handover Algorithm: Why Do We Need Handover ?syrish2622No ratings yet
- Information To CandidatesDocument7 pagesInformation To CandidatesLokesh ModemzNo ratings yet
- Choosing The Right Scholarship Type For Your Otago Master'S DegreeDocument1 pageChoosing The Right Scholarship Type For Your Otago Master'S DegreeSubkhan11No ratings yet
- Week 10Document1 pageWeek 10nikhilsolanki1127No ratings yet
- TNPSC Vao Basics of Village Administration Notes in Tamil PDF 2016 - Part 1 PDFDocument6 pagesTNPSC Vao Basics of Village Administration Notes in Tamil PDF 2016 - Part 1 PDFRajesh GovindNo ratings yet
- TNPSC Vao Basics of Village Administration Notes in Tamil PDF 2016 - Part 1Document6 pagesTNPSC Vao Basics of Village Administration Notes in Tamil PDF 2016 - Part 1Srk Siva IyerNo ratings yet
- Week 14Document1 pageWeek 14nikhilsolanki1127No ratings yet
- TTS-29 04 2024-05 05 2024Document2 pagesTTS-29 04 2024-05 05 2024devpradhan258No ratings yet
- EJMCM Volume 7 Issue 10 Pages 1400-1409Document10 pagesEJMCM Volume 7 Issue 10 Pages 1400-1409ismahfrNo ratings yet
- Quality Assurance in Radiation DosimetryDocument9 pagesQuality Assurance in Radiation DosimetrydinkarvermaNo ratings yet
- TTS-06 05 2024-12 05 2024Document2 pagesTTS-06 05 2024-12 05 2024E Fact WorldNo ratings yet
- SBSV - Rnav Gnss 167 - Iac - 20201212Document1 pageSBSV - Rnav Gnss 167 - Iac - 20201212Leonardo BrasilNo ratings yet
- Dragomirov: Manual de SolfejoDocument22 pagesDragomirov: Manual de SolfejoMiguel RojasNo ratings yet
- TTS-13 05 2024-19 05 2024Document2 pagesTTS-13 05 2024-19 05 2024IX D-49 SIDHARTH HOTANo ratings yet
- LSCs As On 16 - 07 - 19Document4 pagesLSCs As On 16 - 07 - 19shiva karnatiNo ratings yet
- 1512738340648-Courses 18Document6 pages1512738340648-Courses 18Durgesh JaiswalNo ratings yet
- Diagrama Maxx Force 13Document7 pagesDiagrama Maxx Force 13WalterNo ratings yet
- Materials Today: Proceedings: M.A. Munjer, Venkatesh Boddapati, M.R.I. Sheikh, M.A. AlimDocument6 pagesMaterials Today: Proceedings: M.A. Munjer, Venkatesh Boddapati, M.R.I. Sheikh, M.A. Alimbipul ahmedNo ratings yet
- NIR For Blending Time-2Document11 pagesNIR For Blending Time-2Itzel Melitce Martinez RomeroNo ratings yet
- MarineDocument1 pageMarineMystique Sri LankaNo ratings yet
- TTS-05 09 2022-11 09 2022Document1 pageTTS-05 09 2022-11 09 2022Hello BroNo ratings yet
- A Robust Encoderless Predictive Current Control Using Novel MRAS Observer For Surface-Mounted Permanent-Magnet Synchronous GeneratorsDocument21 pagesA Robust Encoderless Predictive Current Control Using Novel MRAS Observer For Surface-Mounted Permanent-Magnet Synchronous GeneratorsYahya AsiriNo ratings yet
- Week 13Document1 pageWeek 13nikhilsolanki1127No ratings yet
- B-XRD1001 Quantitative Analysis of A 4-Component Sample by WPPF Method ApplicationNote Q0723en PDFDocument1 pageB-XRD1001 Quantitative Analysis of A 4-Component Sample by WPPF Method ApplicationNote Q0723en PDFYiinjian LowNo ratings yet
- TTS-15.04.2024-21.04.2024 (1) - 1Document2 pagesTTS-15.04.2024-21.04.2024 (1) - 1E Fact WorldNo ratings yet
- Irisetcc20 PDFDocument6 pagesIrisetcc20 PDFamitgapsNo ratings yet
- MAIN Time Table 18-23 MAY 2021 SENIOR WINGDocument21 pagesMAIN Time Table 18-23 MAY 2021 SENIOR WINGMeenu KhannaNo ratings yet
- Netmanias.2013.02.15 LTE Protocol Stack UE Side (E)Document1 pageNetmanias.2013.02.15 LTE Protocol Stack UE Side (E)Mahendra Nath ReddyNo ratings yet
- Engine Controls XC90 2006Document4 pagesEngine Controls XC90 2006Rogelio ArenasNo ratings yet
- XII-NEET: 2021-22: Solutions Chemical EquilibriumDocument5 pagesXII-NEET: 2021-22: Solutions Chemical EquilibriumLalit KNo ratings yet
- Week 9Document1 pageWeek 9nikhilsolanki1127No ratings yet
- Week 7Document1 pageWeek 7nikhilsolanki1127No ratings yet
- Week 6Document1 pageWeek 6nikhilsolanki1127No ratings yet
- TTS-02 01 2023-08 01 2023Document1 pageTTS-02 01 2023-08 01 2023Monster GamerNo ratings yet
- SEACG2020 Parallel SessionDocument1 pageSEACG2020 Parallel SessionRamadhani Yasyfi CyselaNo ratings yet
- Using Nuclear Microsatellite Data To Trace The Gene Flow and Population Structure in Czech HorsesDocument5 pagesUsing Nuclear Microsatellite Data To Trace The Gene Flow and Population Structure in Czech HorsesFarisNo ratings yet
- Field Evaluation Smart Citizen Kit v2.1Document27 pagesField Evaluation Smart Citizen Kit v2.1Gisselle GranadaNo ratings yet
- AnalogyDocument19 pagesAnalogyAkshaya institute HyderabadNo ratings yet
- Cellular Technologies Evolution From 3G To 4G and BeyondDocument52 pagesCellular Technologies Evolution From 3G To 4G and BeyondstNo ratings yet
- 1512730534726-Iriset Signal NG Course Calendar 2018 PDFDocument3 pages1512730534726-Iriset Signal NG Course Calendar 2018 PDFRohit KumarNo ratings yet
- XII-NEET: 2021-22: Solutions Chemical EquilibriumDocument4 pagesXII-NEET: 2021-22: Solutions Chemical EquilibriumLalit KNo ratings yet
- NASA 140640main ESAS 09Document22 pagesNASA 140640main ESAS 09NASAdocumentsNo ratings yet
- DKP E-Learning 18 Januari 2023, BST, Ism Code, Erm, BRMDocument5 pagesDKP E-Learning 18 Januari 2023, BST, Ism Code, Erm, BRMReyexer ReckyNo ratings yet
- Summary Staff and Worker Data BaseDocument7 pagesSummary Staff and Worker Data BaseBHRBPP SHE TeamNo ratings yet
- Mumbai OneDocument1 pageMumbai OnehelloymousNo ratings yet
- CFD Modeling and Optimization of Magneto-Rheological Abrasive Flow Finishing (MRAFF) ProcessDocument50 pagesCFD Modeling and Optimization of Magneto-Rheological Abrasive Flow Finishing (MRAFF) Processsoumyajit dasNo ratings yet
- TTS-05 12 2022-11 12 2022-1Document1 pageTTS-05 12 2022-11 12 2022-1Sanket RoutNo ratings yet
- Supervisors' Training Centre, Secunderabad Feed Back Form: AppropriateDocument4 pagesSupervisors' Training Centre, Secunderabad Feed Back Form: AppropriateSsk0% (1)
- Assignment 03 - Matrix Inverses and DeterminantsDocument2 pagesAssignment 03 - Matrix Inverses and DeterminantscoosssyNo ratings yet
- Doublecurvepricingslidesv11 12653096880345 Phpapp01Document21 pagesDoublecurvepricingslidesv11 12653096880345 Phpapp01sbearNo ratings yet
- Esquemas de Serviços Periodicidade FT Ciclo I PV Espécie Ciclo RMM TolerânciaDocument9 pagesEsquemas de Serviços Periodicidade FT Ciclo I PV Espécie Ciclo RMM TolerânciaJames EstanislauNo ratings yet
- Paper#141 Acise2019 AchmadWidodoDocument20 pagesPaper#141 Acise2019 AchmadWidodoachmad widodoNo ratings yet
- Hints & Solution: NEET/JEE: 2020-21Document2 pagesHints & Solution: NEET/JEE: 2020-21shantinath123gmailcoNo ratings yet
- TIME TABLE W40 (26th September - 02nd October 2022)Document2 pagesTIME TABLE W40 (26th September - 02nd October 2022)skylardexNo ratings yet
- Kia Engine 3 of 3 PDFDocument1 pageKia Engine 3 of 3 PDFKevine KhaledNo ratings yet
- Kia Engine 3 of 3 PDFDocument1 pageKia Engine 3 of 3 PDFKevine KhaledNo ratings yet
- Patient's Assessment and ReassesmentDocument8 pagesPatient's Assessment and ReassesmenttopNo ratings yet
- Medical Record Review ToolsDocument10 pagesMedical Record Review ToolstopNo ratings yet
- C41 Bed Management Policy Nov21Document46 pagesC41 Bed Management Policy Nov21topNo ratings yet
- ACCP Cardiology PRN JC June 2022Document16 pagesACCP Cardiology PRN JC June 2022topNo ratings yet
- 1045amET HOST EXAM Acc 2021Document22 pages1045amET HOST EXAM Acc 2021topNo ratings yet
- Rajiv Gandhi University of Health Sciences Exam Result: PrintDocument1 pageRajiv Gandhi University of Health Sciences Exam Result: PrintTauheed ahmedNo ratings yet
- Emergencies in General PracticeDocument17 pagesEmergencies in General PracticeIoana NavaliciNo ratings yet
- Microeconomics: Assignment 1: Moving Less, Retiring LaterDocument6 pagesMicroeconomics: Assignment 1: Moving Less, Retiring LaterRuhi UppalNo ratings yet
- GDP Audit Checklist For Storage & Transport of PharmaDocument11 pagesGDP Audit Checklist For Storage & Transport of Pharmaمحيد محيمدانNo ratings yet
- (Intercity Bus Schedule Via Geoga Bridge) : Busan Gohyeon Gohyeon BusanDocument3 pages(Intercity Bus Schedule Via Geoga Bridge) : Busan Gohyeon Gohyeon BusanNur Khairah Bahirah SafianNo ratings yet
- Group 9 - Roles of Community Health Nurse in EhealthDocument11 pagesGroup 9 - Roles of Community Health Nurse in EhealthCharlene RepolloNo ratings yet
- Draft Final Oral Health Strategic Plan 2020-2025 v3Document42 pagesDraft Final Oral Health Strategic Plan 2020-2025 v3Romualdo Das Neves XimenesNo ratings yet
- Behavioral Pattern - FinalDocument6 pagesBehavioral Pattern - FinalSaileneGuemoDellosaNo ratings yet
- CV 2022042413502179Document2 pagesCV 2022042413502179Shennah AlertaNo ratings yet
- CPG Philippine Clinical Practice Guideline On Palliative and End of Life Care For Adults With CancerDocument225 pagesCPG Philippine Clinical Practice Guideline On Palliative and End of Life Care For Adults With CancermjartezaNo ratings yet
- Dr. Fe Del Mundo A Pioneer in Pediatric MedicineDocument11 pagesDr. Fe Del Mundo A Pioneer in Pediatric Medicinekyla arboledaNo ratings yet
- Patients Bill of Rights - Nursing JurisprudenceDocument2 pagesPatients Bill of Rights - Nursing JurisprudenceVia Songcal100% (1)
- Clinical Nursing Judgement PaperDocument5 pagesClinical Nursing Judgement Paperapi-663237692No ratings yet
- 7 Chapter 3 Goals of Prevention Methods of PreventionDocument4 pages7 Chapter 3 Goals of Prevention Methods of Preventionaryam aliNo ratings yet
- Philatelic Gossip 180 APR 18 1925Document28 pagesPhilatelic Gossip 180 APR 18 1925Gele TraafNo ratings yet
- Ejercicios de KpiDocument89 pagesEjercicios de KpiVlone DorianNo ratings yet
- MejigoDocument2 pagesMejigoGaurav YadavNo ratings yet
- Medical Claim Sheet RajuDocument2 pagesMedical Claim Sheet RajurajusgowdarNo ratings yet
- Transport GuideDocument31 pagesTransport GuideGrimmo1979No ratings yet
- Learning Guide - 43: Apply Quality ControlDocument6 pagesLearning Guide - 43: Apply Quality ControlKena SamuelNo ratings yet
- Reducing Patient Falls On The Telemetry Unit: Korri Tanner, Sydney Carskadon, Claire Caviolo, Chance SasserDocument15 pagesReducing Patient Falls On The Telemetry Unit: Korri Tanner, Sydney Carskadon, Claire Caviolo, Chance Sasserapi-707685857No ratings yet
- Vermont DecertificationsDocument1 pageVermont DecertificationsMaleeha SyedNo ratings yet
- DTH Pharmacy PresentationDocument46 pagesDTH Pharmacy PresentationdrkefyalewtayeNo ratings yet
- A1 Passers Training, Research, Review & Development CompanyDocument6 pagesA1 Passers Training, Research, Review & Development CompanyPaul EspinosaNo ratings yet
- Mapehhealth Q4 Summative-TestDocument1 pageMapehhealth Q4 Summative-TestMary Grace BanugNo ratings yet
- Provision 7 9Document15 pagesProvision 7 9IsbelNo ratings yet
- OHW NarrativeDocument5 pagesOHW NarrativeJESSICA ARNADONo ratings yet