You might also like
- Airport Design GuidelinesDocument408 pagesAirport Design Guidelinesnickolololo67% (9)
- Cardiac Cycle by Bala GoyalDocument14 pagesCardiac Cycle by Bala Goyaltee su lingNo ratings yet
- Cardiac CycleDocument35 pagesCardiac CycleEnuga Applegate100% (1)
- 4,5-Cardiac Cycle Team441Document29 pages4,5-Cardiac Cycle Team441aliusman laseNo ratings yet
- PC Cardiac CycleDocument29 pagesPC Cardiac CycleSebontu HasenNo ratings yet
- Cardiac Cycle: DR Rida Ajmal KhanDocument29 pagesCardiac Cycle: DR Rida Ajmal KhanMooma fatimaNo ratings yet
- CARDIAC CYCLE - Part I PDFDocument55 pagesCARDIAC CYCLE - Part I PDFChirag Dagar100% (1)
- Lecture On Cardiac Cycle by DR RoomiDocument43 pagesLecture On Cardiac Cycle by DR RoomiMudassar Roomi100% (2)
- Cardiac Cycle by Dr. RoomiDocument71 pagesCardiac Cycle by Dr. RoomiMudassar Roomi100% (3)
- Cardiovascular SystemDocument50 pagesCardiovascular Systemkintan kamila100% (1)
- Cardiac Cycle: DR Rakesh JainDocument97 pagesCardiac Cycle: DR Rakesh JainKemoy FrancisNo ratings yet
- Cardiac CycleDocument30 pagesCardiac CycleCarrine Liew100% (2)
- Cardiac Cycle: The Events of the HeartbeatDocument37 pagesCardiac Cycle: The Events of the Heartbeatindra_jeet2009No ratings yet
- Cardiovascular Physiology: October 25, 2010Document51 pagesCardiovascular Physiology: October 25, 2010VinuPrakashJ.No ratings yet
- Lecture-5 Cardiac CycleDocument28 pagesLecture-5 Cardiac Cyclettalhalatif99No ratings yet
- Cardiac CycleDocument36 pagesCardiac Cycleanushkav443No ratings yet
- Cardiovascular PhysiologyDocument88 pagesCardiovascular Physiologykhorrami4No ratings yet
- Cardiac Cycle Phases ExplainedDocument27 pagesCardiac Cycle Phases ExplainedThird Year B PharmNo ratings yet
- Cardiac Cycle: DR - Lalitha Shanmugam, Professor of Physiology, VMCHDocument56 pagesCardiac Cycle: DR - Lalitha Shanmugam, Professor of Physiology, VMCHRamakrishnanNo ratings yet
- The Cardiac Cycle ExplainedDocument15 pagesThe Cardiac Cycle ExplainedNimisha BalakrishnanNo ratings yet
- The Cardiac Cycle ExplainedDocument15 pagesThe Cardiac Cycle ExplainedNimisha BalakrishnanNo ratings yet
- The Cardiac CycleDocument19 pagesThe Cardiac CycleRebi NesroNo ratings yet
- Cardiac Cycle: Prepared By: Mineshkumar Prajapati Roll No: 05 Biomedical Science (2021-22)Document21 pagesCardiac Cycle: Prepared By: Mineshkumar Prajapati Roll No: 05 Biomedical Science (2021-22)minesh prajapatiNo ratings yet
- The Cardiac Cycle ExplainedDocument18 pagesThe Cardiac Cycle ExplainedKundan GuptaNo ratings yet
- Circulatory SystemDocument304 pagesCirculatory Systemyapyihao2100% (1)
- DR Rahimah Zakaria Dept of PhysiologyDocument31 pagesDR Rahimah Zakaria Dept of PhysiologyChokJunHoongNo ratings yet
- Cardiac CycleDocument31 pagesCardiac CycleAdwaitha KrNo ratings yet
- Cardiac CycleDocument9 pagesCardiac Cycle502-s21-027No ratings yet
- Heart As A Pump: Departemen Fisiologi Fakultas Kedokteran Universitas Sumatera UtaraDocument33 pagesHeart As A Pump: Departemen Fisiologi Fakultas Kedokteran Universitas Sumatera UtaraXeniel AlastairNo ratings yet
- Physiology: Zhao Chun-ling (赵春玲) Email: Phone:18683073667Document62 pagesPhysiology: Zhao Chun-ling (赵春玲) Email: Phone:18683073667Akshay ChaudharyNo ratings yet
- 04-The Cardiac Cycle - Wigger's Diagram (J Swanevelder)Document6 pages04-The Cardiac Cycle - Wigger's Diagram (J Swanevelder)Patrick WilliamsNo ratings yet
- CARDIAC CYCLE-laDocument12 pagesCARDIAC CYCLE-latehillahkabwe100No ratings yet
- Cardiac Physiology PDFDocument17 pagesCardiac Physiology PDFAli Aborges Jr.No ratings yet
- Cardiac Cycle StagesDocument19 pagesCardiac Cycle StagesKhalid AbdullahNo ratings yet
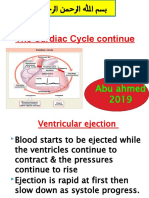
- The Cardiac Cycle Continue: Abu Ahmed 2019Document19 pagesThe Cardiac Cycle Continue: Abu Ahmed 2019Khalid AbdullahNo ratings yet
- K - 12 Heart As A Pump (Fisiologi)Document36 pagesK - 12 Heart As A Pump (Fisiologi)missirenaNo ratings yet
- Physiology of CardiovascularDocument74 pagesPhysiology of CardiovascularStevan SalosaNo ratings yet
- Cardiac Cycle - DR Rakesh JainDocument97 pagesCardiac Cycle - DR Rakesh JainEmmieNo ratings yet
- Cardiac cycle: Mechanical events and hemodynamic changesDocument20 pagesCardiac cycle: Mechanical events and hemodynamic changesKelly Yeow100% (3)
- KP 1.3.2.1 Aktivitas Mekanik Jantung (2 Jam)Document68 pagesKP 1.3.2.1 Aktivitas Mekanik Jantung (2 Jam)Try MutiaraNo ratings yet
- The Cardiac CycleDocument9 pagesThe Cardiac CycleKaylababy Hamilton BlackNo ratings yet
- Cv-4 PHDocument28 pagesCv-4 PHaya najemNo ratings yet
- DR Najeeb Cardiac CycleDocument5 pagesDR Najeeb Cardiac Cycleعلي. احمد100% (1)
- K Sembulingam Essentials of Medical Physiology 6th 105 PDFDocument11 pagesK Sembulingam Essentials of Medical Physiology 6th 105 PDFBlerta Deari100% (2)
- Prof DR Najneen AkhterDocument62 pagesProf DR Najneen Akhterislamamirul0487No ratings yet
- 5 Cardiac Cycle & Heart SoundsDocument32 pages5 Cardiac Cycle & Heart SoundsDisha SuvarnaNo ratings yet
- Cardiac CycleDocument7 pagesCardiac Cycletewogbadeomobuwajo005No ratings yet
- 4,5-Cardiac Cycle 1&2Document31 pages4,5-Cardiac Cycle 1&2Aqeel Raza HessamNo ratings yet
- Cardiac Cycle ABHINADocument11 pagesCardiac Cycle ABHINAAbhinav Thakur100% (1)
- Cardiac CycleDocument38 pagesCardiac CycleKok HoongNo ratings yet
- Cardiac Cycle Physiology-18!12!2018Document70 pagesCardiac Cycle Physiology-18!12!2018kolyagolpreetikNo ratings yet
- Oral PathologyDocument23 pagesOral PathologyRuba AbbassNo ratings yet
- Assign MNTDocument13 pagesAssign MNTADITYAROOP PATHAKNo ratings yet
- The Sequence of Events That Occur in The Heart During Cardiac CycleDocument13 pagesThe Sequence of Events That Occur in The Heart During Cardiac CycleADITYAROOP PATHAKNo ratings yet
- The Cardiac Cycle NotesDocument5 pagesThe Cardiac Cycle NotesAsad Khan Khalil100% (1)
- Cardiac Cycle: Presenter: DR Hairul Anuar Bin MahatDocument23 pagesCardiac Cycle: Presenter: DR Hairul Anuar Bin MahatHairul AnuarNo ratings yet
- Anatomy 10_01_18 posteDocument19 pagesAnatomy 10_01_18 posteOlga KucinskaNo ratings yet
- Cardiovascular Physiology ExplainedDocument33 pagesCardiovascular Physiology ExplainedHanaNo ratings yet
- Jantung Sebagai PompaDocument54 pagesJantung Sebagai PompaIndraYudhiNo ratings yet
- Uconnect User GuideDocument113 pagesUconnect User GuidetamilarasansrtNo ratings yet
- Manhole bill of materialsDocument1 pageManhole bill of materialsjalNo ratings yet
- Large Generators WEBDocument16 pagesLarge Generators WEBMaycon MaranNo ratings yet
- Pricing For International Markets 1. Discuss The Causes of and Solutions For Parallel (Grey Markets) Imports and Their Effects On PriceDocument23 pagesPricing For International Markets 1. Discuss The Causes of and Solutions For Parallel (Grey Markets) Imports and Their Effects On PricePeter Mboma100% (1)
- Lesson 2 - Procedures in Cleaning Utensils and EquipmentDocument26 pagesLesson 2 - Procedures in Cleaning Utensils and EquipmentReizel TulauanNo ratings yet
- K&J Quotation For Geotechnical - OLEODocument4 pagesK&J Quotation For Geotechnical - OLEORamakrishnaNo ratings yet
- Qualitative Research On Vocabulary and Spelling Skills of A Student Chapters I IIIDocument23 pagesQualitative Research On Vocabulary and Spelling Skills of A Student Chapters I IIIarniza blazoNo ratings yet
- Listening 2 - Log 4 - Answer. SheetDocument3 pagesListening 2 - Log 4 - Answer. SheetNguyen LeeNo ratings yet
- EEE111_Multisim_ManualDocument14 pagesEEE111_Multisim_ManualSHADOW manNo ratings yet
- Omega 1 Akanksha 9069664Document5 pagesOmega 1 Akanksha 9069664Akanksha SarangiNo ratings yet
- Recipe of Medical AirDocument13 pagesRecipe of Medical AirMd. Rokib ChowdhuryNo ratings yet
- React Rich Text EditorDocument3 pagesReact Rich Text Editordhirendrapratapsingh398No ratings yet
- List of Blade MaterialsDocument19 pagesList of Blade MaterialsAnie Ummu Alif & SyifaNo ratings yet
- Data Sheet Ads1292rDocument69 pagesData Sheet Ads1292rKaha SyawalNo ratings yet
- 3M SS Filters Data SheetDocument4 pages3M SS Filters Data SheetbinnisfquoteNo ratings yet
- MSDS Slideway Oil Iso VG 68 - 031115Document6 pagesMSDS Slideway Oil Iso VG 68 - 031115Rini SiskayantiNo ratings yet
- The Brain from Inside Out Chapter 4 SummaryDocument20 pagesThe Brain from Inside Out Chapter 4 SummaryjuannnnNo ratings yet
- TQM 2 MARKSDocument12 pagesTQM 2 MARKSMARIYAPPANNo ratings yet
- RSG 303Document196 pagesRSG 303Makinde TimiNo ratings yet
- SRV210 - 250TC Spare PartsDocument2 pagesSRV210 - 250TC Spare PartsEnzo SovittiNo ratings yet
- Mercedes Vario 1996 2003 PDF Service ManualDocument22 pagesMercedes Vario 1996 2003 PDF Service Manualveronicamurphy070288aqwNo ratings yet
- Contoh Skripsi Bahasa Inggris Case StudyDocument18 pagesContoh Skripsi Bahasa Inggris Case StudyRizki Fajrita100% (14)
- PV380 Operations ManualDocument20 pagesPV380 Operations ManualCarlosNo ratings yet
- Module 3 - Tennnis: Cit Colleges of Paniqui Foundation IncDocument14 pagesModule 3 - Tennnis: Cit Colleges of Paniqui Foundation IncLahra BalanciaNo ratings yet
- Tata Steel-MDP SessionDocument69 pagesTata Steel-MDP Sessionsasharma82No ratings yet
- Hospital NetworkDocument36 pagesHospital NetworkAbhishek MishraNo ratings yet
- AP Poetry TermsDocument8 pagesAP Poetry TermsTEACHER BARAY LLCE ANGLAISNo ratings yet
- Beowulf The Monsters and The Critics SevDocument20 pagesBeowulf The Monsters and The Critics SevNirmala GaneshNo ratings yet
- Williamstown Cannabis Cultivation PlanDocument48 pagesWilliamstown Cannabis Cultivation PlanOltion JaupajNo ratings yet