You might also like
- Sporozoa (Plasmodium SPP and Babesia SPP)Document31 pagesSporozoa (Plasmodium SPP and Babesia SPP)the songwriterNo ratings yet
- MalariaDocument30 pagesMalariaderilNo ratings yet
- Malarial ParasitesDocument5 pagesMalarial ParasitesZette ArañaNo ratings yet
- Cestodes (Tapeworm) : Diphyllobotium Latum - 20 Yrs Life SpanDocument4 pagesCestodes (Tapeworm) : Diphyllobotium Latum - 20 Yrs Life SpanMicael Andrei MendozaNo ratings yet
- Malaria Plasmodium SPP WPDocument5 pagesMalaria Plasmodium SPP WPPerlie CNo ratings yet
- MalariaDocument25 pagesMalariaYelai CarveroNo ratings yet
- Lesson 5 Plasmodium SPPDocument8 pagesLesson 5 Plasmodium SPPAnya IgnacioNo ratings yet
- PLASMODIUMDocument2 pagesPLASMODIUMKylieNo ratings yet
- Phylum ApicomplexaDocument6 pagesPhylum ApicomplexaAneezaNo ratings yet
- Hemoflagellates Protozoa: Scientific Name Disease Commune NameDocument6 pagesHemoflagellates Protozoa: Scientific Name Disease Commune Nameaust austNo ratings yet
- ParasitologyDocument4 pagesParasitologyIan ZyrusNo ratings yet
- Activity 2 Blood and Tissue ProtozoansDocument42 pagesActivity 2 Blood and Tissue ProtozoansRaven TolentinoNo ratings yet
- Lesson 5 - PlasmodiumDocument9 pagesLesson 5 - PlasmodiumAnya IgnacioNo ratings yet
- PlasmodiumDocument92 pagesPlasmodiumnitesh rawat100% (1)
- PLASMODIUMDocument3 pagesPLASMODIUMsakalam shipper48No ratings yet
- Exercise 6: Malarial Parasites: Parasitology LaboratoryDocument2 pagesExercise 6: Malarial Parasites: Parasitology LaboratorySigfred Tarnate AoasNo ratings yet
- SPOROZOADocument5 pagesSPOROZOACDNo ratings yet
- Parasites by Apple TanDocument16 pagesParasites by Apple TanOlivia LimNo ratings yet
- Parasites PetalsDocument115 pagesParasites PetalsMcarl MatelNo ratings yet
- SPOROZOADocument1 pageSPOROZOAJ Pao Bayro - LacanilaoNo ratings yet
- Malaria: EtiologyDocument10 pagesMalaria: EtiologyAlayza Joy GasmenNo ratings yet
- Unit 4 Apicomplexa Malaria-1Document48 pagesUnit 4 Apicomplexa Malaria-1Denise MichelleNo ratings yet
- TrematodesDocument16 pagesTrematodesRenz Gerard AmorNo ratings yet
- Para01 - Lab Parasitology 2 (1/1) Finals: RemindersDocument2 pagesPara01 - Lab Parasitology 2 (1/1) Finals: Remindersrenato renatoNo ratings yet
- PLASMODIUMDocument5 pagesPLASMODIUMGhina RizwanNo ratings yet
- Subphylum Sporozoa - MalariaDocument6 pagesSubphylum Sporozoa - MalariaeniNo ratings yet
- Protozoa Darah (Malaria) : Dr. Dwi Handayani, Mkes Staf Bagian Parasitologi Fakultas Kedokteran UnsriDocument88 pagesProtozoa Darah (Malaria) : Dr. Dwi Handayani, Mkes Staf Bagian Parasitologi Fakultas Kedokteran UnsriGladis Aprilla RizkiNo ratings yet
- MalariaDocument7 pagesMalariaKapil ShindeNo ratings yet
- Module 5: Phylum Nematoda: Wuchereria BancroftiDocument11 pagesModule 5: Phylum Nematoda: Wuchereria BancroftiJulienne LopezNo ratings yet
- 6.2 2021para ReviewlocalwactsDocument35 pages6.2 2021para ReviewlocalwactsHeyzel joy FabianNo ratings yet
- Plasmodium. Leishmania, TripanosomaDocument48 pagesPlasmodium. Leishmania, TripanosomaStefan SaerangNo ratings yet
- Week 2 (Lec-Lab) Mls 306 Clinical Parasitology Bsmls 3A: Ascaris LumbricoidesDocument4 pagesWeek 2 (Lec-Lab) Mls 306 Clinical Parasitology Bsmls 3A: Ascaris LumbricoidesHannah Beatrice Adame TamayoNo ratings yet
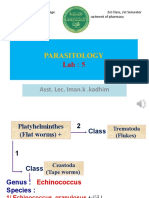
- Platyhelminthes - 6th Class PDFDocument23 pagesPlatyhelminthes - 6th Class PDFAbdulla Hil KafiNo ratings yet
- Parasitology Review On FlagellatesDocument2 pagesParasitology Review On FlagellatesKaoriMarieSembranoNo ratings yet
- 6 Plasmodium SPPDocument1 page6 Plasmodium SPPKaycee Gretz LorescaNo ratings yet
- 5 WormsDocument5 pages5 Wormsreaj.jumsaliNo ratings yet
- Dientamoeba Fragilis: Intestinal FlagellatesDocument4 pagesDientamoeba Fragilis: Intestinal FlagellatesRitz CelsoNo ratings yet
- CestodesDocument6 pagesCestodesKathryn JeuelNo ratings yet
- Para-Transes Pre-Final Exam - Unit 4Document11 pagesPara-Transes Pre-Final Exam - Unit 4Aysha AishaNo ratings yet
- Sistematika ParasitDocument30 pagesSistematika ParasitFatmawati NadhyaNo ratings yet
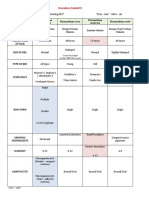
- Malaria TableDocument1 pageMalaria TableSuha AbdullahNo ratings yet
- Parasitology: Asst. Lec. Iman.k .KadhimDocument12 pagesParasitology: Asst. Lec. Iman.k .Kadhimهاني عقيل حسين جوادNo ratings yet
- Trematodes LectureDocument7 pagesTrematodes LectureCherie QuintoNo ratings yet
- Morphological Characteristics of Malaria ParasitesDocument71 pagesMorphological Characteristics of Malaria Parasitesed100% (6)
- 2023 ParaLab Trans04 2 MalariaDocument1 page2023 ParaLab Trans04 2 MalariaBrionelle DumelodNo ratings yet
- Plasmodium Table SummaryDocument2 pagesPlasmodium Table Summarychelsea xxNo ratings yet
- M6Document14 pagesM6Julianne Marie LacsentoNo ratings yet
- Significance of Commensal Amebae in StoolDocument12 pagesSignificance of Commensal Amebae in StoolNicolle PanchoNo ratings yet
- Blood and Tissue Protozoa (Con't) : DR - Mehru Nisha Mehrunisha@unikl - Edu.myDocument35 pagesBlood and Tissue Protozoa (Con't) : DR - Mehru Nisha Mehrunisha@unikl - Edu.myNida RidzuanNo ratings yet
- GR2 Plasmodium-Spp PDFDocument29 pagesGR2 Plasmodium-Spp PDFEran Mark RojasNo ratings yet
- RMTnotes PARASITOLOGYDocument68 pagesRMTnotes PARASITOLOGYArvin O-CaféNo ratings yet
- Cestodes 2020Document10 pagesCestodes 2020CDNo ratings yet
- (PARA) 1.5 - Blood and Tissue FlagellatesDocument6 pages(PARA) 1.5 - Blood and Tissue FlagellatesGuia De GuzmanNo ratings yet
- P. WestermaniDocument5 pagesP. Westermaniella diazNo ratings yet
- Adobe Scan 17-Nov-2022 PDFDocument3 pagesAdobe Scan 17-Nov-2022 PDFKOLIPAKULA POORNIMANo ratings yet
- Comparing The Malaria SpeciesDocument3 pagesComparing The Malaria SpeciesiglesiasowenNo ratings yet
- MLS 306 Week 3Document2 pagesMLS 306 Week 3Hannah Beatrice Adame TamayoNo ratings yet
- Blood SmearsDocument4 pagesBlood SmearsAmor KourdouliNo ratings yet
- Para Finals - 2Document4 pagesPara Finals - 2Jill NuñezNo ratings yet
- Atlas of Pyrenulaceae and Trypetheliaceae - Volume 1: Lichenized AscomycotaFrom EverandAtlas of Pyrenulaceae and Trypetheliaceae - Volume 1: Lichenized AscomycotaNo ratings yet
- Veterinary QuestionsDocument19 pagesVeterinary QuestionskuldipNo ratings yet
- Lecture 7 BabesiaDocument27 pagesLecture 7 BabesiaEmmanuel Thon Mading100% (1)
- Unit 11. Blood and Tissue Coccidian (Apicomplexa)Document40 pagesUnit 11. Blood and Tissue Coccidian (Apicomplexa)Michael DawitNo ratings yet
- Pro To Zoology 1954 KudoDocument988 pagesPro To Zoology 1954 KudoClaau GomezNo ratings yet
- Linhares Et Al., 2002 PDFDocument6 pagesLinhares Et Al., 2002 PDFVanessa HolsbachNo ratings yet
- Free Living Amoeba and CoccidiansDocument33 pagesFree Living Amoeba and CoccidiansGlanela ManalotoNo ratings yet
- Antibabesial Treatment Protocols Against Canine Babesiosis: W.R. Bandula Kumara B.V.SC., PH.DDocument8 pagesAntibabesial Treatment Protocols Against Canine Babesiosis: W.R. Bandula Kumara B.V.SC., PH.DJehan Somasiri JayathungaNo ratings yet
- Lesson 5 Plasmodium SPPDocument8 pagesLesson 5 Plasmodium SPPAnya IgnacioNo ratings yet
- Parasitology Babesia SPP CatDocument1 pageParasitology Babesia SPP CatIrina AtudoreiNo ratings yet
- Dairy Cattle DiseasesDocument14 pagesDairy Cattle DiseasesLaddi SandhuNo ratings yet
- Blood & Tissue ProtozoaDocument81 pagesBlood & Tissue ProtozoaMoses Tamba MomohNo ratings yet
- Canine Babesiosis Treatment RegiemsDocument5 pagesCanine Babesiosis Treatment RegiemsHitesh Shandilaya100% (1)
- Parasitic Inclusions in ErythrocytesDocument27 pagesParasitic Inclusions in ErythrocytesLian Marie ViñasNo ratings yet
- Blood SmearsDocument4 pagesBlood SmearsAmor KourdouliNo ratings yet
- Blood and Tissue ParasitesDocument62 pagesBlood and Tissue Parasitesapi-3856362No ratings yet
- Companion Animal Parasitology: A Clinical Perspective: Peter J. IrwinDocument13 pagesCompanion Animal Parasitology: A Clinical Perspective: Peter J. IrwinAngela SanchezNo ratings yet
- Handbook of ZoonosesDocument245 pagesHandbook of ZoonosesDenisa VescanNo ratings yet
- Dracunculus Medinensis and Filarial WormsDocument19 pagesDracunculus Medinensis and Filarial WormsAnastasiaNo ratings yet
- Veterinary Parasitology Arthropod 2 Ticks 2015Document81 pagesVeterinary Parasitology Arthropod 2 Ticks 2015Gheorghita Ileana100% (1)
- Module 6.4 ParasitesDocument6 pagesModule 6.4 ParasitesPNo ratings yet
- Zoonotic Potentiality of Protozoa: Assignment Subject: ParasitologyDocument7 pagesZoonotic Potentiality of Protozoa: Assignment Subject: ParasitologyArushi PatiyalNo ratings yet
- tmpAB64 TMPDocument216 pagestmpAB64 TMPFrontiersNo ratings yet
- FACULTATEA DE MEDICINĂ VETERINARĂ Lucrari StiintificeDocument148 pagesFACULTATEA DE MEDICINĂ VETERINARĂ Lucrari StiintificeCorina AlinaNo ratings yet
- Veterinary ProtozoologyDocument43 pagesVeterinary Protozoologywarda100% (1)
- Disorders of Blood and Blood Forming Organs in EquineDocument89 pagesDisorders of Blood and Blood Forming Organs in EquineasheneyNo ratings yet
- Babesia Canis and Other Tick Borne Infections in Dogs in Central Poland 2009 Veterinary ParasitolDocument8 pagesBabesia Canis and Other Tick Borne Infections in Dogs in Central Poland 2009 Veterinary ParasitolGabriela Victoria MartinescuNo ratings yet
- ICAR JRF Veterinary Question Paper - PSCDocument6 pagesICAR JRF Veterinary Question Paper - PSCSatyabrat DuttaNo ratings yet
- Equino PiroplasmoseDocument13 pagesEquino PiroplasmoseRogério Oliva CarvalhoNo ratings yet
- Babesia - PPT 2Document13 pagesBabesia - PPT 2jazelNo ratings yet
- Prevalence of Ovine and Caprine Babesiosis in Baligubadle-District PDFDocument36 pagesPrevalence of Ovine and Caprine Babesiosis in Baligubadle-District PDFRidwan MohamedNo ratings yet