You might also like
- Neurosonological Evaluation of Cerebral Venous Outflow: An Ultrasound AtlasFrom EverandNeurosonological Evaluation of Cerebral Venous Outflow: An Ultrasound AtlasNo ratings yet
- Comparison of Sequentially Measured Aloka Echo-Tracking One-Point Pulse Wave Velocity With Sphygmocor Carotid-Femoral Pulse Wave VelocityDocument7 pagesComparison of Sequentially Measured Aloka Echo-Tracking One-Point Pulse Wave Velocity With Sphygmocor Carotid-Femoral Pulse Wave VelocitySmart DocNo ratings yet
- Jhype 32 149Document5 pagesJhype 32 149Rizko Putra PradanaNo ratings yet
- Ultrasound Imaging of Congestion in Heart Failure Examinations BeyondDocument10 pagesUltrasound Imaging of Congestion in Heart Failure Examinations BeyondAncylostoma DuodenaleNo ratings yet
- 2014-08-03 09.09.53 6Document9 pages2014-08-03 09.09.53 6Nag Mallesh RaoNo ratings yet
- Ultrasound Diagnostics of Renal StenosisDocument10 pagesUltrasound Diagnostics of Renal StenosisJosè Julio Cejas SànchezNo ratings yet
- DTI Superposition PDFDocument7 pagesDTI Superposition PDFEtel SilvaNo ratings yet
- Ultrasound Non-Invasive Measurement of Intracranial Pressure in Neurointensive Care: A Prospective Observational StudyDocument16 pagesUltrasound Non-Invasive Measurement of Intracranial Pressure in Neurointensive Care: A Prospective Observational StudyRonald GoyesNo ratings yet
- An Advanced Detrending Method With Application To HRV AnalysisDocument4 pagesAn Advanced Detrending Method With Application To HRV AnalysisWenshan LuoNo ratings yet
- Diagnostic Performance of Angiography-Based FractiDocument9 pagesDiagnostic Performance of Angiography-Based FractiIrina Andra TacheNo ratings yet
- Spleen Stiffness-Spleen Size-To-platelet Ratio RiskDocument6 pagesSpleen Stiffness-Spleen Size-To-platelet Ratio RiskValentina IorgaNo ratings yet
- The Role of Color Doppler Ultrasound in Living Donor Liver Transplantation 2008 Journal of Medical UltrasoundDocument11 pagesThe Role of Color Doppler Ultrasound in Living Donor Liver Transplantation 2008 Journal of Medical UltrasoundIman Ru-ancaNo ratings yet
- Codifo Etica Medica ProfissionalDocument9 pagesCodifo Etica Medica ProfissionalBernardo Nascentes BrunoNo ratings yet
- Minimally Invasive Cardiac Output Monitors: Kate E Drummond MBBS FANZCA Edward Murphy MBBS FANZCADocument6 pagesMinimally Invasive Cardiac Output Monitors: Kate E Drummond MBBS FANZCA Edward Murphy MBBS FANZCApankaj88gmcNo ratings yet
- Dupplex Scanning of The Peripheral Arteries: Correlation of The Peak Velocity Ratio With Angiographics Diameter ReductionDocument8 pagesDupplex Scanning of The Peripheral Arteries: Correlation of The Peak Velocity Ratio With Angiographics Diameter Reductionpaquidermo85No ratings yet
- Nihms 951502Document24 pagesNihms 951502Svt Mscofficial2No ratings yet
- Analysis and Characterization of Photo-Plethysmographic SignalDocument7 pagesAnalysis and Characterization of Photo-Plethysmographic Signalpradeep4u2009No ratings yet
- Discordance Between Echocardiography and MRI in The Assessment of Mitral Regurgitation SeverityDocument11 pagesDiscordance Between Echocardiography and MRI in The Assessment of Mitral Regurgitation SeverityPanfilAlinaNo ratings yet
- โชคดี สิทธิยานุรักษ์ Comparison of Ankle- Brachial Index (ABI) Measurement between a New Oscillometric Device (MESI ABPI MD%22) and the Standard Doppler Method in the Diagnosis of Lower Extremity Arterial Disease (LDocument5 pagesโชคดี สิทธิยานุรักษ์ Comparison of Ankle- Brachial Index (ABI) Measurement between a New Oscillometric Device (MESI ABPI MD%22) and the Standard Doppler Method in the Diagnosis of Lower Extremity Arterial Disease (LChokdee SittiyanurakNo ratings yet
- Electrocardiographic Criteria For The Diagnosis of Left Ventricular HypertrophyDocument10 pagesElectrocardiographic Criteria For The Diagnosis of Left Ventricular HypertrophyHendri SaputraNo ratings yet
- 2014 Perfusion MriDocument24 pages2014 Perfusion MriR M MNo ratings yet
- Diagnosis of Carpal Tunnel SyndromeDocument11 pagesDiagnosis of Carpal Tunnel SyndromeMrAppleNo ratings yet
- Tataklaksana KacauDocument7 pagesTataklaksana KacauKrysnaNo ratings yet
- CAMPO Meas Sci Technol 2014 PDFDocument11 pagesCAMPO Meas Sci Technol 2014 PDFhoplalaNo ratings yet
- Minimally Invasive Cardiac Output by BJApdfDocument6 pagesMinimally Invasive Cardiac Output by BJApdfblessing akataNo ratings yet
- 2023 - Improved Transcranial Doppler Waveform Analysis For Intracranial Hypertension Assessment in Patients With Traumatic Brain InjuryDocument10 pages2023 - Improved Transcranial Doppler Waveform Analysis For Intracranial Hypertension Assessment in Patients With Traumatic Brain InjuryOlga Manco GuzmánNo ratings yet
- FYP in Flow 3-dDocument8 pagesFYP in Flow 3-dAwais EhsanNo ratings yet
- PIIS0007091217372124Document2 pagesPIIS0007091217372124Sangeeta TrivediNo ratings yet
- Piezoelectric Approaches For Wearable Continuous Blood Pressure Monitoring A ReviewDocument12 pagesPiezoelectric Approaches For Wearable Continuous Blood Pressure Monitoring A Reviewkeyvan babaeiNo ratings yet
- Cardiac ValveDocument21 pagesCardiac ValveSean ChenNo ratings yet
- Project Phase 1 - Odd2021-2Document14 pagesProject Phase 1 - Odd2021-2Spoorthi S VNo ratings yet
- Vena Cava DonorDocument7 pagesVena Cava Donorazizk83No ratings yet
- Reprod Domestic Animals - 2014 - Ortega Ferrusola - Use of Colour and Spectral Doppler Ultrasonography in StallionDocument9 pagesReprod Domestic Animals - 2014 - Ortega Ferrusola - Use of Colour and Spectral Doppler Ultrasonography in StallionAmanda CristinaNo ratings yet
- Bjs 11398Document9 pagesBjs 11398ratnayanti udinNo ratings yet
- Vejdani Jahromi2015Document10 pagesVejdani Jahromi2015Daniel Stefano Vásquez RojasNo ratings yet
- Accuracy of 2D and Point Shear Wave Elastography-Based Measurment For Diagnossi of Esophageal Varices A Systemic Review and Meta AnalisisDocument11 pagesAccuracy of 2D and Point Shear Wave Elastography-Based Measurment For Diagnossi of Esophageal Varices A Systemic Review and Meta AnalisisValentina IorgaNo ratings yet
- Velocity Vector Imaging: Standard Tissue-Tracking Results Acquired in Normals-The VVI-STRAIN StudyDocument10 pagesVelocity Vector Imaging: Standard Tissue-Tracking Results Acquired in Normals-The VVI-STRAIN StudyCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- GNL 13 206Document9 pagesGNL 13 206boyhutaperiNo ratings yet
- 227 Full PDFDocument3 pages227 Full PDFanon_629352389No ratings yet
- Near Infrared Spectroscopy As A Predictor For Shunt Requirement During Carotid EndarterectomyDocument9 pagesNear Infrared Spectroscopy As A Predictor For Shunt Requirement During Carotid EndarterectomyAmira DayoubNo ratings yet
- Relationship Between Ventricular Rate Variability in Nonsustained Ventricular Tachycardia and Subsequent Cardiac EventsDocument6 pagesRelationship Between Ventricular Rate Variability in Nonsustained Ventricular Tachycardia and Subsequent Cardiac EventsRobertoNo ratings yet
- Jurnal 222Document3 pagesJurnal 222rizalmantaNo ratings yet
- Original Contribution: Implementation of Spectral Width Doppler in Pulsatile Flow MeasurementsDocument7 pagesOriginal Contribution: Implementation of Spectral Width Doppler in Pulsatile Flow MeasurementsFrontiersNo ratings yet
- Interpretation of Arterial Duplex Testing of LowerextremityDocument10 pagesInterpretation of Arterial Duplex Testing of LowerextremityLuciano AlvesNo ratings yet
- Indications and Utility in The Intensive Care Unit: NeuromonitoringDocument11 pagesIndications and Utility in The Intensive Care Unit: NeuromonitoringphilipNo ratings yet
- Descrição Da Técnica - Sommerset2019Document7 pagesDescrição Da Técnica - Sommerset2019José Sergio Garcia de AlmeidaNo ratings yet
- Jawahar 1997Document4 pagesJawahar 1997Mohammed RickyNo ratings yet
- Gray-Matter Volume Estimate Score - A Novel Semi-Automatic Method Measuring Early Ischemic Change On CTDocument7 pagesGray-Matter Volume Estimate Score - A Novel Semi-Automatic Method Measuring Early Ischemic Change On CTkartini ciatawiNo ratings yet
- Biomedical Signal Processing and ControlDocument10 pagesBiomedical Signal Processing and ControlSERGIO ANDRES ROMERO TORRESNo ratings yet
- Wu 2018Document8 pagesWu 2018Karel ZertucheNo ratings yet
- Ultrasound Shear Wave Elasticity Imaging Quantifies Coronary Perfusion Pressure Effect On Cardiac ComplianceDocument9 pagesUltrasound Shear Wave Elasticity Imaging Quantifies Coronary Perfusion Pressure Effect On Cardiac CompliancejuanNo ratings yet
- Eacvi Recommendations Valvular Regurgitation Summary PDFDocument34 pagesEacvi Recommendations Valvular Regurgitation Summary PDFstoicea_katalinNo ratings yet
- Acharya Et Al. - 2006 - Heart Rate Variability A ReviewDocument22 pagesAcharya Et Al. - 2006 - Heart Rate Variability A Reviewicaro 2024No ratings yet
- Stroke Volume Variation For Prediction of Fluid Responsiveness in Patients Undergoing Gastrointestinal SurgeryDocument8 pagesStroke Volume Variation For Prediction of Fluid Responsiveness in Patients Undergoing Gastrointestinal SurgeryossinNo ratings yet
- Hypertensionaha 118 10839Document3 pagesHypertensionaha 118 10839memounuNo ratings yet
- Muscle and Nerve - 2012 - Frijlink - Increased Nerve Vascularization Detected by Color Doppler Sonography in Patients WithDocument6 pagesMuscle and Nerve - 2012 - Frijlink - Increased Nerve Vascularization Detected by Color Doppler Sonography in Patients WithChadiIbrahimNo ratings yet
- Deteksi Qrs Komplek Pada Pembacaan Heart Rate Variability (Metode TwoDocument12 pagesDeteksi Qrs Komplek Pada Pembacaan Heart Rate Variability (Metode TwoAyu NissaNo ratings yet
- Ultra 34 4 649Document6 pagesUltra 34 4 649FiqitaNo ratings yet
- Cardiologist-Level Arrhythmia Detection With Convolutional Neural Networks Stanford ML Group Pranav Rakpurkar, Awni Hannun, Codie Bourn, Andrew NGDocument9 pagesCardiologist-Level Arrhythmia Detection With Convolutional Neural Networks Stanford ML Group Pranav Rakpurkar, Awni Hannun, Codie Bourn, Andrew NGAdvaitNo ratings yet
- Completion Equipment ChecklistDocument3 pagesCompletion Equipment ChecklistYougchu LuanNo ratings yet
- Section 23 - Floco 382 and 383 MetersDocument24 pagesSection 23 - Floco 382 and 383 MetershammamiNo ratings yet
- Sepam Range High Impedance Differential ProtectionDocument12 pagesSepam Range High Impedance Differential ProtectionosmpotNo ratings yet
- Causes of Status EpilepticusDocument12 pagesCauses of Status EpilepticusSergio MouraNo ratings yet
- IS Code Based-QuestionsDocument27 pagesIS Code Based-QuestionsGURIJALA UJWAL KUMARNo ratings yet
- XMTC DatasheetDocument4 pagesXMTC DatasheetSelva RajNo ratings yet
- (U) Daily Activity Report: Marshall DistrictDocument5 pages(U) Daily Activity Report: Marshall DistrictFauquier NowNo ratings yet
- Natural Bioactive Compounds of Citrus Limon For Food and Health PDFDocument19 pagesNatural Bioactive Compounds of Citrus Limon For Food and Health PDFEsteban Davila100% (1)
- 002 Pediatric Obesity An IntroductionDocument24 pages002 Pediatric Obesity An IntroductionAnurag BhatejaNo ratings yet
- Medical Research With Music and The BrainDocument4 pagesMedical Research With Music and The BrainEngerber MarquezNo ratings yet
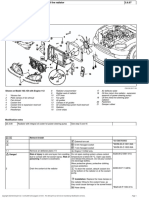
- Radiator Remove&installDocument3 pagesRadiator Remove&installHermes VacaNo ratings yet
- South 4Document24 pagesSouth 4LariNo ratings yet
- Branch Circuit Calculations Feeders Services and Overcurrent DevicesDocument61 pagesBranch Circuit Calculations Feeders Services and Overcurrent DevicesVic Rizenn Isidore BobilesNo ratings yet
- Fannie Mae Appraiser Independence Requirements 10-15-2010Document4 pagesFannie Mae Appraiser Independence Requirements 10-15-2010Frank GregoireNo ratings yet
- Project Execution PlanDocument70 pagesProject Execution PlanCedie Sietereales100% (1)
- Industrial Charcoal Production With Power Generation at Mully Children'S Family Yatta, KenyaDocument87 pagesIndustrial Charcoal Production With Power Generation at Mully Children'S Family Yatta, KenyapramitasNo ratings yet
- 2020 Guidelines WebDocument249 pages2020 Guidelines WebDaryl Barrios LamedaNo ratings yet
- Practical Project Management 101: Unit StandardsDocument109 pagesPractical Project Management 101: Unit StandardsHrh Charmagne Thando NkosiNo ratings yet
- List of Acacia Species Known To Contain Psychoactive Alkaloids - WikipediaDocument15 pagesList of Acacia Species Known To Contain Psychoactive Alkaloids - WikipediaRicardo Campuzano100% (1)
- The Anti-Violence Against Women and Their Children Act (Ra 9262)Document39 pagesThe Anti-Violence Against Women and Their Children Act (Ra 9262)Mimhy VallegaNo ratings yet
- BS-240 New Service Manual V2.0 enDocument378 pagesBS-240 New Service Manual V2.0 enAji Abdulah100% (2)
- Anthrax en PDFDocument6 pagesAnthrax en PDFWinni FebriariNo ratings yet
- Property Issue Agreement: Vinod Patel Group It DepartmentDocument3 pagesProperty Issue Agreement: Vinod Patel Group It DepartmentMaloni SavikeNo ratings yet
- 4100R Series - Thick Film Molded DIPsDocument3 pages4100R Series - Thick Film Molded DIPssiogNo ratings yet
- Bridging The Gap How Community Health Workers Promote The Health of ImmigrantsDocument257 pagesBridging The Gap How Community Health Workers Promote The Health of ImmigrantsNidaUlfahNo ratings yet
- Integrated Door Motor Controller User Manual: Shenyang Bluelight Automatic Technology Co., LTDDocument56 pagesIntegrated Door Motor Controller User Manual: Shenyang Bluelight Automatic Technology Co., LTDJulio Cesar GonzalezNo ratings yet
- Biyani's Think Tank: Cell Biology & GeneticsDocument81 pagesBiyani's Think Tank: Cell Biology & GeneticsAkshay chandrakarNo ratings yet
- Unit 7 ListeningDocument41 pagesUnit 7 ListeningHo NgocthuNo ratings yet
- Alur WBI Online CrusherDocument7 pagesAlur WBI Online Crusheremping 72No ratings yet
- The First Battle of GroznyDocument71 pagesThe First Battle of GroznyScimitar Mcmlxv100% (1)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (5)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 4.5 out of 5 stars4.5/5 (84)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeFrom EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeRating: 5 out of 5 stars5/5 (4)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (40)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (267)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 4 out of 5 stars4/5 (5)
- I Shouldn't Feel This Way: Name What’s Hard, Tame Your Guilt, and Transform Self-Sabotage into Brave ActionFrom EverandI Shouldn't Feel This Way: Name What’s Hard, Tame Your Guilt, and Transform Self-Sabotage into Brave ActionNo ratings yet
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (44)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (46)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (4)
- To Explain the World: The Discovery of Modern ScienceFrom EverandTo Explain the World: The Discovery of Modern ScienceRating: 3.5 out of 5 stars3.5/5 (51)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesFrom EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesRating: 4.5 out of 5 stars4.5/5 (1412)
- Self-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!From EverandSelf-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Rating: 5 out of 5 stars5/5 (1)