You might also like
- Healing Across Cultures: Pathways to Indigenius Health EquityFrom EverandHealing Across Cultures: Pathways to Indigenius Health EquityNo ratings yet
- Indigenous Cultural Training For Health Workers in AustraliaDocument11 pagesIndigenous Cultural Training For Health Workers in AustraliaLe HuyNo ratings yet
- Measuring Social and Emotional Wellbeing in Aboriginal Youth Using Strong Souls: A Rasch Measurement ApproachDocument18 pagesMeasuring Social and Emotional Wellbeing in Aboriginal Youth Using Strong Souls: A Rasch Measurement ApproachMares InliwanNo ratings yet
- 1-s2.0-S1326020023000547-main (1)Document10 pages1-s2.0-S1326020023000547-main (1)Neal TorwaneNo ratings yet
- Assessment 3Document9 pagesAssessment 3Teliah ThyssenNo ratings yet
- Articulo Nuevo TEAFDocument14 pagesArticulo Nuevo TEAFyury urregoNo ratings yet
- Western Notions of Informed Consent and Indigenous Cultures: Australian Findings at The InterfaceDocument11 pagesWestern Notions of Informed Consent and Indigenous Cultures: Australian Findings at The InterfaceJanet YauNo ratings yet
- Promote AboDocument20 pagesPromote AboDavid WilsonNo ratings yet
- Chapter Objectives: Health Care and Indigenous AustraliansDocument1 pageChapter Objectives: Health Care and Indigenous AustraliansAhmedFarooqNo ratings yet
- Goris PDFDocument24 pagesGoris PDFAndrew WongNo ratings yet
- Cultural Safety No Turning BackDocument2 pagesCultural Safety No Turning BackCale HollowayNo ratings yet
- RetrieveDocument10 pagesRetrieveAlexa Ramírez ContrerasNo ratings yet
- Term 2 Reflection 4Document3 pagesTerm 2 Reflection 4api-477982644No ratings yet
- ReviewDocument11 pagesReviewyhenti widjayantiNo ratings yet
- Aboriginal Health and Aboriginal Health Statistics: COSPAR Information Bulletin May 1982Document42 pagesAboriginal Health and Aboriginal Health Statistics: COSPAR Information Bulletin May 1982fahad zakirNo ratings yet
- 1 s2.0 S2211335521003673 MainDocument13 pages1 s2.0 S2211335521003673 MainMarichelle LeclairNo ratings yet
- Evidence Based PracticeDocument11 pagesEvidence Based PracticesulhaaskaNo ratings yet
- Mental Health Research and EvaDocument26 pagesMental Health Research and EvaRima MuhsenNo ratings yet
- Culture and Healthy Lifestyles: A Qualitative Exploration of The Role of Food and Physical Activity in Three Urban Australian Indigenous CommunitiesDocument6 pagesCulture and Healthy Lifestyles: A Qualitative Exploration of The Role of Food and Physical Activity in Three Urban Australian Indigenous CommunitiesnettyNo ratings yet
- East Kimberley concepts of health and illnessDocument13 pagesEast Kimberley concepts of health and illnessgeralddsackNo ratings yet
- Decolonising AustraliaDocument22 pagesDecolonising AustraliaJamal Mughal100% (2)
- Copy 2Document7 pagesCopy 2Abdullah SakhiNo ratings yet
- Understanding Culture's Importance in Nursing CareDocument9 pagesUnderstanding Culture's Importance in Nursing CareRahul SharmaNo ratings yet
- 2008 Munro2008Document17 pages2008 Munro2008Lucila S. RolfoNo ratings yet
- IKC101 Assessment 3Document9 pagesIKC101 Assessment 3ovov711No ratings yet
- CALD in AustraliaDocument7 pagesCALD in AustraliaJosphat MwangiNo ratings yet
- Intersecting Cultures in Deaf Mental Health: An Ethnographic Study of NHS Professionals Diagnosing Autism in D/deaf ChildrenDocument22 pagesIntersecting Cultures in Deaf Mental Health: An Ethnographic Study of NHS Professionals Diagnosing Autism in D/deaf ChildrenCarol Albuquerque0% (1)
- Article Review Name - ID - Course Name - Date of SubmissionDocument6 pagesArticle Review Name - ID - Course Name - Date of SubmissionPrachi SharmaNo ratings yet
- Article Print 4155Document12 pagesArticle Print 4155bejanNo ratings yet
- Barriers_Accessing_Mental_HealDocument6 pagesBarriers_Accessing_Mental_HealRima MuhsenNo ratings yet
- WT Part 1 Chapt 4 FinalDocument14 pagesWT Part 1 Chapt 4 FinalNatasha AlbaShakiraNo ratings yet
- SEWB Fact SheetDocument4 pagesSEWB Fact Sheetalbatross558No ratings yet
- Deeble Institue Issues Brief No 19 1Document15 pagesDeeble Institue Issues Brief No 19 1dyan ayu puspariniNo ratings yet
- African Traditional Medicine's Contributions to Nigeria's HealthcareDocument12 pagesAfrican Traditional Medicine's Contributions to Nigeria's HealthcareAliNo ratings yet
- Cultural Competency in Health PDFDocument6 pagesCultural Competency in Health PDFMikaela HomukNo ratings yet
- Cultural Competence in Correctional Mental HealthDocument8 pagesCultural Competence in Correctional Mental HealthArielNo ratings yet
- 2 GreenblattDocument10 pages2 Greenblattisabel galloNo ratings yet
- Research participation by people with intellectual disability and mental health issues: An examination of the processes of consentDocument12 pagesResearch participation by people with intellectual disability and mental health issues: An examination of the processes of consentyalenaj09No ratings yet
- Negotiated Assignment ProposalDocument2 pagesNegotiated Assignment ProposalJerome PrattNo ratings yet
- Providing Culturally Appropriate Care: A Literature ReviewDocument9 pagesProviding Culturally Appropriate Care: A Literature ReviewLynette Pearce100% (1)
- Ethical Guideline ATSIDocument8 pagesEthical Guideline ATSINectanabisNo ratings yet
- 1 PB PDFDocument19 pages1 PB PDFKharen Domacena DomilNo ratings yet
- Bellamyetal 2015 Accesstomedication RefugeesDocument7 pagesBellamyetal 2015 Accesstomedication Refugeesdilmav111No ratings yet
- Mental Health Issues Among Refugee Children and Adolescents: Joh Henley and Julie RobinsonDocument12 pagesMental Health Issues Among Refugee Children and Adolescents: Joh Henley and Julie RobinsonMohamed Ridzwan AJNo ratings yet
- Traditional Healing: A Review of LiteratureDocument32 pagesTraditional Healing: A Review of LiteratureMax MarcusNo ratings yet
- Reflection pcp2-1 KsDocument4 pagesReflection pcp2-1 Ksapi-468597987No ratings yet
- Concepts DoajDocument21 pagesConcepts DoajNur AiniNo ratings yet
- 2017 UofT-IndigenousMedEd-HandbookDocument14 pages2017 UofT-IndigenousMedEd-HandbookRésaNo ratings yet
- Ijerph 19 11282 With CoverDocument13 pagesIjerph 19 11282 With Coverandriaeypreel1224No ratings yet
- Religion & SpiritualityDocument31 pagesReligion & SpiritualityMega Lita StevaniNo ratings yet
- Journal 2Document13 pagesJournal 2NurfaizuraNo ratings yet
- Indigenous Health Information and Knowledge SystemsDocument20 pagesIndigenous Health Information and Knowledge SystemsDexter Abrenica AlfonsoNo ratings yet
- MHC Lived Experience PW Framework Oct2022 DigitalDocument44 pagesMHC Lived Experience PW Framework Oct2022 DigitalChrisNo ratings yet
- Exploring The Relationship Between Housing and Health For Refugees and Asylum Seekers in South Australia 2017Document20 pagesExploring The Relationship Between Housing and Health For Refugees and Asylum Seekers in South Australia 2017GuiheneufNo ratings yet
- 1 s2.0 S2157171615311242 MainDocument4 pages1 s2.0 S2157171615311242 MainGustavo Geronimo HernandezNo ratings yet
- Impact of colonisation on Aboriginal healthDocument6 pagesImpact of colonisation on Aboriginal healthマイ ケ ルNo ratings yet
- Health Information Services and Public Healthcare Awareness A Behavioral Study of Rural Inhabitants of The Balasore District of OdishaDocument7 pagesHealth Information Services and Public Healthcare Awareness A Behavioral Study of Rural Inhabitants of The Balasore District of OdishaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- End-Of-life Issues For Aboriginal Patients A Literature ReviewDocument7 pagesEnd-Of-life Issues For Aboriginal Patients A Literature ReviewafmabreouxqmrcNo ratings yet
- Dwnload Full Physical Examination and Health Assessment 6th Edition Jarvis Solutions Manual PDFDocument36 pagesDwnload Full Physical Examination and Health Assessment 6th Edition Jarvis Solutions Manual PDFsithprisus100% (7)
- Assessment 2 - Written.Document5 pagesAssessment 2 - Written.jonkers85No ratings yet
- Human Resources Manager in San Jose CA Resume Priscilla CramerDocument2 pagesHuman Resources Manager in San Jose CA Resume Priscilla CramerPriscillaCramerNo ratings yet
- Colorectal Cancer: Symptoms, Staging and ScreeningDocument65 pagesColorectal Cancer: Symptoms, Staging and ScreeningMuhammed Muzzammil Sangani50% (2)
- SIP Physical SCiDocument8 pagesSIP Physical SCiShane Catherine BesaresNo ratings yet
- IELTS Essay SamplesDocument5 pagesIELTS Essay SamplesRebaz Jamal AhmedNo ratings yet
- Round Hill Community Garden FAQ - Round Hill, VirginiaDocument3 pagesRound Hill Community Garden FAQ - Round Hill, VirginiaZafiriou MavrogianniNo ratings yet
- Neonatal Care Pocket Guide For Hospital Physicians PDFDocument319 pagesNeonatal Care Pocket Guide For Hospital Physicians PDFelmaadawy2002100% (7)
- Obamacare Ushers in New Era For The Healthcare IndustryDocument20 pagesObamacare Ushers in New Era For The Healthcare Industryvedran1980No ratings yet
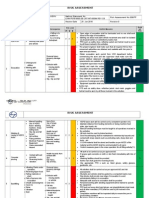
- Hse Risk Assessment - 006 Ra - Hdpe Duct LayingDocument7 pagesHse Risk Assessment - 006 Ra - Hdpe Duct Layingbinunalukandam83% (12)
- The Works of Alan OpenshawDocument38 pagesThe Works of Alan OpenshawAlan OpenshawNo ratings yet
- Water Treatment PDFDocument87 pagesWater Treatment PDFJubin KumarNo ratings yet
- T2anklearthrodesis Optech b1000044d0710Document36 pagesT2anklearthrodesis Optech b1000044d0710Alsed GjoniNo ratings yet
- Penile Injection TherapyDocument4 pagesPenile Injection Therapydr NayanBharadwajNo ratings yet
- Organon of Medicine All Years 2marks Question Viva Questions AnswersDocument12 pagesOrganon of Medicine All Years 2marks Question Viva Questions Answersabcxyz15021999No ratings yet
- Clinical Immunology and AllergyDocument156 pagesClinical Immunology and AllergySoleil DaddouNo ratings yet
- TWC Final Settlement DocsDocument374 pagesTWC Final Settlement DocsTHROnlineNo ratings yet
- Booklet - e 1 - 2013Document101 pagesBooklet - e 1 - 2013Dani AedoNo ratings yet
- Media Kesehatan Masyarakat: Gracewati Rambu Ladu Day, Muntasir Basri, Rina Waty SiraitDocument15 pagesMedia Kesehatan Masyarakat: Gracewati Rambu Ladu Day, Muntasir Basri, Rina Waty Siraitnimas ayu kusumaningrumNo ratings yet
- NCP LymphomaDocument3 pagesNCP Lymphomamahmoud fuqahaNo ratings yet
- Pothole Claim Form in PhiladelphiaDocument3 pagesPothole Claim Form in Philadelphiaphilly victorNo ratings yet
- Psychopathic Personality: Bridging The Gap Between Scientific Evidence and Public PolicyDocument69 pagesPsychopathic Personality: Bridging The Gap Between Scientific Evidence and Public PolicyGokushimakNo ratings yet
- DMLC Part I & II Cyprus (Hyundai Busan)Document17 pagesDMLC Part I & II Cyprus (Hyundai Busan)Shankar Singh0% (1)
- Thomas Foot ReflexologyDocument112 pagesThomas Foot ReflexologySa MiNo ratings yet
- 1.2 POWERPOINT History of ForensicsDocument23 pages1.2 POWERPOINT History of ForensicsSilay Parole & ProbationNo ratings yet
- Detecting Malingering On The MMPI-2 - An Examination of The Utilit PDFDocument56 pagesDetecting Malingering On The MMPI-2 - An Examination of The Utilit PDFernie moreNo ratings yet
- Top 10 Graphic Design Interview Questions and AnswersDocument16 pagesTop 10 Graphic Design Interview Questions and Answersbetsjonh100% (1)
- Ecg 01Document103 pagesEcg 01Bandar al ghamdi100% (1)
- 3075 SWMS RendererDocument13 pages3075 SWMS Renderernik KooNo ratings yet
- Introduction of Online Basic First Aid Course - For Circulation April 2021Document39 pagesIntroduction of Online Basic First Aid Course - For Circulation April 2021Yuwaraj NaiduNo ratings yet
- Leopold Maneuvers Nursing ProcedureDocument3 pagesLeopold Maneuvers Nursing ProcedureDiane grace SorianoNo ratings yet
- Measurement and Correlates of Family Caregiver Self-Efficacy For Managing DementiaDocument9 pagesMeasurement and Correlates of Family Caregiver Self-Efficacy For Managing DementiariskhawatiNo ratings yet