You might also like
- Healing Across Cultures: Pathways to Indigenius Health EquityFrom EverandHealing Across Cultures: Pathways to Indigenius Health EquityNo ratings yet
- SEWB Fact SheetDocument4 pagesSEWB Fact Sheetalbatross558No ratings yet
- Social and Emotional Well Being Framework 2004-2009Document79 pagesSocial and Emotional Well Being Framework 2004-2009MikeJacksonNo ratings yet
- Psychological Healing: Historical and Philosophical Foundations of Professional PsychologyFrom EverandPsychological Healing: Historical and Philosophical Foundations of Professional PsychologyNo ratings yet
- Mason Durie ReadingDocument8 pagesMason Durie ReadingTim Dennis100% (1)
- Backup of s2 Ole1615 - Ole1616Document3 pagesBackup of s2 Ole1615 - Ole1616Vivien LiuNo ratings yet
- Measuring Social and Emotional Wellbeing in Aboriginal Youth Using Strong Souls: A Rasch Measurement ApproachDocument18 pagesMeasuring Social and Emotional Wellbeing in Aboriginal Youth Using Strong Souls: A Rasch Measurement ApproachMares InliwanNo ratings yet
- OLET1616 - The Science of Health and WellbeingDocument6 pagesOLET1616 - The Science of Health and Wellbeinghillbilly675No ratings yet
- RetrieveDocument10 pagesRetrieveAlexa Ramírez ContrerasNo ratings yet
- Decolonising AustraliaDocument22 pagesDecolonising AustraliaJamal Mughal100% (2)
- Journal Pone 0280213Document10 pagesJournal Pone 0280213Kasep PisanNo ratings yet
- Pacific Cultural Competencies FrameworkDocument22 pagesPacific Cultural Competencies FrameworkSándor TóthNo ratings yet
- MHC Lived Experience PW Framework Oct2022 DigitalDocument44 pagesMHC Lived Experience PW Framework Oct2022 DigitalChrisNo ratings yet
- E Haku Inoa: To Weave A Name Discussion GuideDocument13 pagesE Haku Inoa: To Weave A Name Discussion GuideChristenHepuakoaMarquezNo ratings yet
- 0408PP TrujilloDocument15 pages0408PP TrujillojaverianaNo ratings yet
- National Aboriginal and Torres Strait Islander Health Plan 2021 2031Document107 pagesNational Aboriginal and Torres Strait Islander Health Plan 2021 2031MeNo ratings yet
- Health_psychology[1]Document8 pagesHealth_psychology[1]Ritika SenNo ratings yet
- What Is Health EssayDocument1 pageWhat Is Health Essayathialiu12No ratings yet
- Cultural Competency in Health PDFDocument6 pagesCultural Competency in Health PDFMikaela HomukNo ratings yet
- Understanding Culture's Importance in Nursing CareDocument9 pagesUnderstanding Culture's Importance in Nursing CareRahul SharmaNo ratings yet
- Hea TH HistoryDocument3 pagesHea TH HistoryFasra ChiongNo ratings yet
- أساسيات طب المجتمع 1Document318 pagesأساسيات طب المجتمع 1Visalini VimalaNo ratings yet
- Halbert DunnDocument7 pagesHalbert DunnNaresh K SinghNo ratings yet
- BC Health Quality Matrix March 2020Document14 pagesBC Health Quality Matrix March 2020ather lodhiNo ratings yet
- ResearchDocument8 pagesResearchArchie Dumalag GarciaNo ratings yet
- CALD in AustraliaDocument7 pagesCALD in AustraliaJosphat MwangiNo ratings yet
- Personal Philosophy On Therapeutic RecreationDocument19 pagesPersonal Philosophy On Therapeutic Recreationapi-282894761100% (1)
- Cultural Competence in Correctional Mental HealthDocument8 pagesCultural Competence in Correctional Mental HealthArielNo ratings yet
- Ticman, Analyn M.: Review On Related LiteratureDocument9 pagesTicman, Analyn M.: Review On Related LiteratureRodger AreolaNo ratings yet
- Ethical Guideline ATSIDocument8 pagesEthical Guideline ATSINectanabisNo ratings yet
- Physical Examination and Health Assessment 6th Edition Jarvis Solutions Manual PDFDocument36 pagesPhysical Examination and Health Assessment 6th Edition Jarvis Solutions Manual PDFverandalocallyrcp821100% (27)
- Cultural Factors in Elder CareDocument8 pagesCultural Factors in Elder CareDannah Jean GranNo ratings yet
- Ancient GreeceDocument4 pagesAncient GreeceDalida Stephanie miriam STEM 11ANo ratings yet
- Dwnload Full Physical Examination and Health Assessment 6th Edition Jarvis Solutions Manual PDFDocument36 pagesDwnload Full Physical Examination and Health Assessment 6th Edition Jarvis Solutions Manual PDFsithprisus100% (7)
- CHN 1 Lec Module1Document17 pagesCHN 1 Lec Module1Jimlord GarciaNo ratings yet
- Preliminary Psychometric Properties of The Multidimensional Well-Being InventoryDocument1 pagePreliminary Psychometric Properties of The Multidimensional Well-Being InventoryShelly P. Harrell, Ph.D.No ratings yet
- World Happiness Report, 2world Happiness Report, 2013013Document172 pagesWorld Happiness Report, 2world Happiness Report, 2013013VictorAradanNo ratings yet
- Filipino PsychologyDocument8 pagesFilipino PsychologyDayanara TolentinoNo ratings yet
- Mark & Lyons, 2010Document9 pagesMark & Lyons, 2010Isaac James BisharaNo ratings yet
- WYECPaperDocument4 pagesWYECPaperPatricia LacanlaleNo ratings yet
- Trans CulturalDocument74 pagesTrans CulturalAirah Ramos PacquingNo ratings yet
- Copy 2Document7 pagesCopy 2Abdullah SakhiNo ratings yet
- Contemplative Practices: A Strategy To Improve Health and Reduce DisparitiesDocument9 pagesContemplative Practices: A Strategy To Improve Health and Reduce DisparitieschrtestaNo ratings yet
- Article Review Name - ID - Course Name - Date of SubmissionDocument6 pagesArticle Review Name - ID - Course Name - Date of SubmissionPrachi SharmaNo ratings yet
- Health and The CommunityDocument20 pagesHealth and The CommunityJane BautistaNo ratings yet
- Cultural, Ethical Context of Health LiteracyDocument4 pagesCultural, Ethical Context of Health Literacykimani JosephNo ratings yet
- WPA Position Statement Spirituality Psy-15!02!23Document3 pagesWPA Position Statement Spirituality Psy-15!02!23ursoaycaNo ratings yet
- Foundations of Multicultural Psychology Intro SampleDocument16 pagesFoundations of Multicultural Psychology Intro SampleGlory Mae ProllesNo ratings yet
- Purnell L. The Purnell Model For Cultural Competence. Journal of Transcultural NursingDocument10 pagesPurnell L. The Purnell Model For Cultural Competence. Journal of Transcultural NursingCengizhan ErNo ratings yet
- Public Health Assignment Explains Key Health ConceptsDocument12 pagesPublic Health Assignment Explains Key Health ConceptsPragya PandeyNo ratings yet
- Bahan Bacaan - 1 - Culture The Missing Link in Health ReseaDocument10 pagesBahan Bacaan - 1 - Culture The Missing Link in Health ReseaannisyahmerianaazanNo ratings yet
- Nursing Theory Essay 1 WeeblyDocument7 pagesNursing Theory Essay 1 Weeblyapi-305752422No ratings yet
- Recovery and Person-Centred Care in Dementia: Common Purpose, Common Practice?Document11 pagesRecovery and Person-Centred Care in Dementia: Common Purpose, Common Practice?thebonsaitreeNo ratings yet
- SARVIMAKI 2006 - Well-Being As Being Well - A Heideggerian Look at Well-BeingDocument7 pagesSARVIMAKI 2006 - Well-Being As Being Well - A Heideggerian Look at Well-BeingApeiron30No ratings yet
- World Happiness Report 2013Document156 pagesWorld Happiness Report 2013sofiabloemNo ratings yet
- 3 3a CHN FamilyDocument7 pages3 3a CHN FamilyJanelle Ann AntonioNo ratings yet
- The Purnell Model For Cultural CompetenceDocument11 pagesThe Purnell Model For Cultural CompetenceJoebert BangsoyNo ratings yet
- Drost 2019 - Indigenous Healing PracticesDocument9 pagesDrost 2019 - Indigenous Healing PracticesMoo HooNo ratings yet
- Health and Wellness AssignmentDocument17 pagesHealth and Wellness AssignmentAnjena KeshaNo ratings yet
- Prescription of Renin Angiotensin System Blockers and Risk of AKIDocument9 pagesPrescription of Renin Angiotensin System Blockers and Risk of AKINatasha AlbaShakiraNo ratings yet
- Gender Differences in AKI To CKD TransitionDocument13 pagesGender Differences in AKI To CKD TransitionNatasha AlbaShakiraNo ratings yet
- Sex Specific Differences in Haemodialysis Prevalences and Practices and Male To Female Mortality RateDocument17 pagesSex Specific Differences in Haemodialysis Prevalences and Practices and Male To Female Mortality RateNatasha AlbaShakiraNo ratings yet
- Metzenbaum Scissors: Lighter Scissors Used For Cutting Delicate Tissue (E.g., Heart) and For Blunt Dissection. Also Called "Metz" in PracticeDocument2 pagesMetzenbaum Scissors: Lighter Scissors Used For Cutting Delicate Tissue (E.g., Heart) and For Blunt Dissection. Also Called "Metz" in PracticeNatasha AlbaShakiraNo ratings yet
- Cellular and Molecular Mechanisms of Sex Differences in Renal Ischaemia Reperfusion InjuryDocument10 pagesCellular and Molecular Mechanisms of Sex Differences in Renal Ischaemia Reperfusion InjuryNatasha AlbaShakiraNo ratings yet
- 2014 - 09 - Accord Policy Brief Unworkability of Greens - Animal Test Bill September 2014Document4 pages2014 - 09 - Accord Policy Brief Unworkability of Greens - Animal Test Bill September 2014Natasha AlbaShakiraNo ratings yet
- Supported Accommodation For People With Severe Mental Illness: An UpdateDocument11 pagesSupported Accommodation For People With Severe Mental Illness: An UpdateNatasha AlbaShakiraNo ratings yet
- Vol 1Document202 pagesVol 1Natasha AlbaShakiraNo ratings yet
- Women and Chronic Kidney Disease - Exploring Gender Differences in Prevalence and Outcomes - University of AberdeenDocument3 pagesWomen and Chronic Kidney Disease - Exploring Gender Differences in Prevalence and Outcomes - University of AberdeenNatasha AlbaShakiraNo ratings yet
- Global Mental Health 5: SeriesDocument10 pagesGlobal Mental Health 5: SeriesNatasha AlbaShakiraNo ratings yet
- PIR - Integration of Mental Health ServicesDocument98 pagesPIR - Integration of Mental Health ServicesNatasha AlbaShakiraNo ratings yet
- Converting Your GPADocument1 pageConverting Your GPAOlegVaskevichNo ratings yet
- A Heavy Burden On Young Minds The Global Burden of Mental and Substance Use Disorders in Children and YouthDocument13 pagesA Heavy Burden On Young Minds The Global Burden of Mental and Substance Use Disorders in Children and YouthNatasha AlbaShakiraNo ratings yet
- Doing Mental Health Care Integration: A Qualitative Study of A New Work RoleDocument14 pagesDoing Mental Health Care Integration: A Qualitative Study of A New Work RoleNatasha AlbaShakiraNo ratings yet
- Vikram Patel - Mental Health For All by Involving All - TED TalkDocument8 pagesVikram Patel - Mental Health For All by Involving All - TED TalkNatasha AlbaShakiraNo ratings yet
- Priorities, 3rd Edition: ReviewDocument14 pagesPriorities, 3rd Edition: ReviewNatasha AlbaShakiraNo ratings yet
- Better Access To Mental Health Care and The Failure of The Medicare Principle of UniversalityDocument6 pagesBetter Access To Mental Health Care and The Failure of The Medicare Principle of UniversalityNatasha AlbaShakiraNo ratings yet
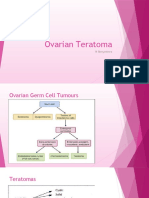
- TeratomaDocument9 pagesTeratomaNatasha AlbaShakiraNo ratings yet
- Mental Health and Aging in The 21st CenturyDocument17 pagesMental Health and Aging in The 21st CenturyNatasha AlbaShakiraNo ratings yet
- Stigma and Discrimination Related To Mental Illness in Low and Middle Income CountriesDocument13 pagesStigma and Discrimination Related To Mental Illness in Low and Middle Income CountriesNatasha AlbaShakiraNo ratings yet
- Grand Challenges: Integrating Mental Health Services Into Priority Health Care PlatformsDocument6 pagesGrand Challenges: Integrating Mental Health Services Into Priority Health Care PlatformsNatasha AlbaShakiraNo ratings yet
- Hyperbaric Oxygen TherapyDocument3 pagesHyperbaric Oxygen TherapyNatasha AlbaShakiraNo ratings yet
- Working Together Aboriginal and Wellbeing 2014Document618 pagesWorking Together Aboriginal and Wellbeing 2014Natasha AlbaShakira100% (1)
- Bone TuteDocument3 pagesBone TuteNatasha AlbaShakiraNo ratings yet
- CBL TopicsDocument1 pageCBL TopicsNatasha AlbaShakiraNo ratings yet
- Management of Pain On The WardsDocument4 pagesManagement of Pain On The WardsNatasha AlbaShakiraNo ratings yet
- Psych OscesDocument1 pagePsych OscesNatasha AlbaShakiraNo ratings yet
- Paediatric SummaryDocument20 pagesPaediatric SummaryNatasha AlbaShakiraNo ratings yet
- CNS InfectionsDocument2 pagesCNS InfectionsNatasha AlbaShakiraNo ratings yet
- Module 2Document23 pagesModule 2Irine Grace PisayNo ratings yet
- Capstone TemplateDocument24 pagesCapstone TemplateHanzTzy GamingNo ratings yet
- PR2 ReviewerDocument3 pagesPR2 ReviewerGabby GargantosNo ratings yet
- Emotions Language Signs BehaviorsDocument2 pagesEmotions Language Signs BehaviorsAthenaNo ratings yet
- National Service Training ProgramDocument7 pagesNational Service Training ProgramBerlyn TagamaNo ratings yet
- Professional Discussion QuestionsDocument2 pagesProfessional Discussion QuestionsViorel OpreaNo ratings yet
- Theory of Architecture Theory of ArchitectureDocument59 pagesTheory of Architecture Theory of ArchitectureChrisella Joy TorresNo ratings yet
- RRL Teachers StressorsDocument13 pagesRRL Teachers StressorsJerven BregañoNo ratings yet
- Adolescent Assess 2 Powerpoint SlidesDocument6 pagesAdolescent Assess 2 Powerpoint Slidesapi-532260281No ratings yet
- Educational PsychologyDocument10 pagesEducational PsychologyabdulNo ratings yet
- Public Health Nutrition From PrinciplesDocument1 pagePublic Health Nutrition From PrinciplesFiza IshtiaqNo ratings yet
- A Seminar Report On Soft Skills: Submitted To Visvesvaraya Technological University, BelgaumDocument18 pagesA Seminar Report On Soft Skills: Submitted To Visvesvaraya Technological University, Belgaumvishal vallapure100% (1)
- Sahnaz Nabila Manuskrip SkripsiDocument13 pagesSahnaz Nabila Manuskrip SkripsiShahnaz NabilaNo ratings yet
- CHIRP Perception Decision Making and Fatigue at Sea 2018 01Document16 pagesCHIRP Perception Decision Making and Fatigue at Sea 2018 01Mithran DirNo ratings yet
- Patients' satisfaction in Saudi hospitals analyzed using SERVQUALDocument11 pagesPatients' satisfaction in Saudi hospitals analyzed using SERVQUALHarari MkiNo ratings yet
- Appsy 2018Document67 pagesAppsy 2018Asad KhanNo ratings yet
- A Study On Effectiveness of Training and DevelopmentDocument3 pagesA Study On Effectiveness of Training and Developmentbabuvijay2No ratings yet
- IB CAS Handbook: A Guide to Creativity, Activity, and ServiceDocument15 pagesIB CAS Handbook: A Guide to Creativity, Activity, and Servicemike simsonNo ratings yet
- Portfolio - Action Research-Jennifer MackayDocument8 pagesPortfolio - Action Research-Jennifer Mackayapi-502451543No ratings yet
- Artigos e Livros de RogersDocument13 pagesArtigos e Livros de RogersSomeflower FlowerNo ratings yet
- Form 1.3 Summary of Current CompetenciesDocument3 pagesForm 1.3 Summary of Current CompetenciesJinky AydallaNo ratings yet
- Nursing Interventions for Self-Care Deficit and DepressionDocument3 pagesNursing Interventions for Self-Care Deficit and DepressionDanica Kate GalleonNo ratings yet
- How It Is Done?: Prepared By: Prof. MARIA LUISA ELMA-BARRETTODocument21 pagesHow It Is Done?: Prepared By: Prof. MARIA LUISA ELMA-BARRETTOPaul Gabriel CasquejoNo ratings yet
- Objective: Address: PHONE: 9019624640, 9113906785. Email IdDocument2 pagesObjective: Address: PHONE: 9019624640, 9113906785. Email Idvivek anandaNo ratings yet
- Big Data & Predictive Analytics: How To SubmitDocument4 pagesBig Data & Predictive Analytics: How To SubmitKrishna MarwahNo ratings yet
- The Biopsychosocial Model ... 2017Document10 pagesThe Biopsychosocial Model ... 2017Camila AlmeidaNo ratings yet
- The Relationship Between Work-Family Con Ict, Correctional Officer Job Stress, and Job SatisfactionDocument18 pagesThe Relationship Between Work-Family Con Ict, Correctional Officer Job Stress, and Job SatisfactionSilvester SimanjuntakNo ratings yet
- Yielding To Temptation Self-Control FailDocument8 pagesYielding To Temptation Self-Control FailwilsonNo ratings yet
- Evaluation For CommunityDocument20 pagesEvaluation For CommunityBebaskita GintingNo ratings yet
- Ebsco Ebooks Career 2015Document12 pagesEbsco Ebooks Career 2015Teodora Maria BulauNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (15)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Troubled: A Memoir of Foster Care, Family, and Social ClassFrom EverandTroubled: A Memoir of Foster Care, Family, and Social ClassRating: 4.5 out of 5 stars4.5/5 (24)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeFrom EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeNo ratings yet
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Summary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (61)
















![Health_psychology[1]](https://imgv2-2-f.scribdassets.com/img/document/724992900/149x198/02a12ea0e1/1713635144?v=1)