You might also like
- 9 Steps To Heal Adrenal Fatigue NaturallyDocument3 pages9 Steps To Heal Adrenal Fatigue NaturallyAndrada Visan100% (1)
- 014 - Site Safety & Health Induction ChecklistDocument2 pages014 - Site Safety & Health Induction ChecklistRosli Bin Abdul Shukor100% (1)
- Naval Special Warfare Physical Training GuideDocument17 pagesNaval Special Warfare Physical Training GuideAnonymous k6Qd0sNo ratings yet
- VAPING 101: A Q&A Guide for Parents - A Doctor’s Advice on How to Keep Your Teens Safe from the Dangers of VapingFrom EverandVAPING 101: A Q&A Guide for Parents - A Doctor’s Advice on How to Keep Your Teens Safe from the Dangers of VapingNo ratings yet
- Appendix 7 Contractor Health and Safety PlanDocument13 pagesAppendix 7 Contractor Health and Safety PlanXozanNo ratings yet
- Hoarding Install and DismantleDocument5 pagesHoarding Install and Dismantleஅருண்ராஜ் கிருஷ்ணன்சாமி100% (1)
- Healthy Habits Presentation Week-1Document19 pagesHealthy Habits Presentation Week-1blutdurstigNo ratings yet
- Obesity AdimeDocument2 pagesObesity Adimeapi-3008826400% (1)
- Thesis On e CigarettesDocument8 pagesThesis On e Cigarettessamanthajonessavannah100% (3)
- AHA Statement-Cardiopulmonary Impact of E-Cigarettes and Vaping-2023Document26 pagesAHA Statement-Cardiopulmonary Impact of E-Cigarettes and Vaping-2023Walter ReyesNo ratings yet
- E-cigarette Effects on Teen Mental HealthDocument76 pagesE-cigarette Effects on Teen Mental HealthJustine Joy Pagulayan Ramirez100% (4)
- Impact of Electronic Cigarettes On Oral Health: A Review: Mahmoud Rouabhia, PHDDocument8 pagesImpact of Electronic Cigarettes On Oral Health: A Review: Mahmoud Rouabhia, PHDاحمد الزهرانيNo ratings yet
- Toxics 10 00074 v3Document10 pagesToxics 10 00074 v3Benítez García Leonardo Axel. 3IM9No ratings yet
- Fred Hsieh - To Vape or Not To VapeDocument2 pagesFred Hsieh - To Vape or Not To VapeKalpikNo ratings yet
- ECigarette SmokingDocument6 pagesECigarette SmokingSofia Rm.No ratings yet
- E-Cigarette Awareness, Use, and Harm Perceptions in US AdultsDocument9 pagesE-Cigarette Awareness, Use, and Harm Perceptions in US AdultsJimin ParkNo ratings yet
- TheEvolvingLandscapeofe CigarettesassDocument30 pagesTheEvolvingLandscapeofe Cigarettesasscumster123No ratings yet
- Potential Oral Health Effects of E-Cigarettes and Vaping: A Review and Case ReportsDocument5 pagesPotential Oral Health Effects of E-Cigarettes and Vaping: A Review and Case ReportsRares SuciaghiNo ratings yet
- Novel Nicotine Delivery Systems and Public Health: The Rise of The E-Cigarette''Document4 pagesNovel Nicotine Delivery Systems and Public Health: The Rise of The E-Cigarette''Frederico SoaresNo ratings yet
- Facts and Fiction On E-Cigs: What Are They?Document6 pagesFacts and Fiction On E-Cigs: What Are They?maria5basNo ratings yet
- MainDocument8 pagesMainlmarquescarvalhNo ratings yet
- HABIT OF USING VAPE CIGARETTE - docxNEWDocument21 pagesHABIT OF USING VAPE CIGARETTE - docxNEWJustinemae UbayNo ratings yet
- A Proposed Policy Agenda For Electronic Cigarettes in The US: Product, Price, Place, and PromotionDocument8 pagesA Proposed Policy Agenda For Electronic Cigarettes in The US: Product, Price, Place, and PromotionBrent StaffordNo ratings yet
- Electronic Cigarettes and Vaping: A New Challenge in Clinical Medicine and Public Health. A Literature ReviewDocument21 pagesElectronic Cigarettes and Vaping: A New Challenge in Clinical Medicine and Public Health. A Literature ReviewJohn Wilmer Dela CernaNo ratings yet
- Thesis On Electronic CigarettesDocument6 pagesThesis On Electronic Cigarettesh0dugiz0zif3100% (2)
- Dinakar2016 PDFDocument10 pagesDinakar2016 PDFGeorgeNo ratings yet
- Ajph 2021 306416Document12 pagesAjph 2021 306416Christian F. SipinNo ratings yet
- Official Statement of The Spanish Society of Pulmonology and Thoracic Surgery (SEPAR) On Electronic Cigarettes and IQOS®Document6 pagesOfficial Statement of The Spanish Society of Pulmonology and Thoracic Surgery (SEPAR) On Electronic Cigarettes and IQOS®Quang HuyNo ratings yet
- E-Cigarettes A 1-Way Street To Traditional Smoking and Nicotine Addiction For YouthDocument4 pagesE-Cigarettes A 1-Way Street To Traditional Smoking and Nicotine Addiction For YouthAsd EfgNo ratings yet
- Electronic Nicotine Delivery Systems (ENDS) and Their Relevance in Oral HealthDocument6 pagesElectronic Nicotine Delivery Systems (ENDS) and Their Relevance in Oral Healthamalia khusnaNo ratings yet
- The Oral Health Impact of Electronic Cigarette Use: A Systematic ReviewDocument32 pagesThe Oral Health Impact of Electronic Cigarette Use: A Systematic Reviewاحمد الزهرانيNo ratings yet
- Nicotine Dev BrainDocument8 pagesNicotine Dev Brainshr3d3rNo ratings yet
- CHAPTER 2 CompressedDocument9 pagesCHAPTER 2 CompressedLyren Aerey GuevarraNo ratings yet
- Association Between E-Cigarette Use and DepressionDocument11 pagesAssociation Between E-Cigarette Use and DepressionRobby RanidoNo ratings yet
- Electronic Nicotine Delivery Systems (ENDS) : What Physicians Should Know About ENDSDocument2 pagesElectronic Nicotine Delivery Systems (ENDS) : What Physicians Should Know About ENDSJanu easwarNo ratings yet
- Ijph 67 1604989Document12 pagesIjph 67 1604989Shreeya AthavaleNo ratings yet
- What Are The Respiratory Effects of E-CigarretesDocument16 pagesWhat Are The Respiratory Effects of E-CigarretesJulio Cesar Boada MartinezNo ratings yet
- E-Cigarettes Literature ReviewDocument5 pagesE-Cigarettes Literature Reviewaflskkcez100% (1)
- E-cigarette, vape and IQOS use linked to lung disease and heart risksDocument3 pagesE-cigarette, vape and IQOS use linked to lung disease and heart risksAF PortaNo ratings yet
- Ajol File Journals - 45 - Articles - 192265 - Submission - Proof - 192265 529 487470 1 10 20200116Document8 pagesAjol File Journals - 45 - Articles - 192265 - Submission - Proof - 192265 529 487470 1 10 20200116diegoud2003No ratings yet
- Are Electronic Nicotine Delivery Systems Helping Cigarette Smokers Quit? Evidence From A Prospective Cohort Study of U.S. Adult Smokers, 2015-2016Document25 pagesAre Electronic Nicotine Delivery Systems Helping Cigarette Smokers Quit? Evidence From A Prospective Cohort Study of U.S. Adult Smokers, 2015-2016drm1238475No ratings yet
- Study Conducted To Evaluate The Adverse Effect of Smoking Among The Adult in The NigeriaDocument6 pagesStudy Conducted To Evaluate The Adverse Effect of Smoking Among The Adult in The NigeriaHasrul Al MuttaqinNo ratings yet
- E-Cigarette Use Among Youth and Young Adults: A Report of the Surgeon GeneralDocument24 pagesE-Cigarette Use Among Youth and Young Adults: A Report of the Surgeon GeneralScherylle Jeanne Martinez AbarcarNo ratings yet
- Datamex - College of Saint Adeline: Senior High School PageDocument4 pagesDatamex - College of Saint Adeline: Senior High School PageRenalyn MaacwileNo ratings yet
- Research Paper About Secondhand SmokeDocument4 pagesResearch Paper About Secondhand Smokeafeaxdhwl100% (1)
- E Cigarette DissertationDocument6 pagesE Cigarette DissertationDoMyCollegePaperSingapore100% (1)
- E-Cigarettes: Glycol) Mists Should Be Avoided,"Document2 pagesE-Cigarettes: Glycol) Mists Should Be Avoided,"Mick PolNo ratings yet
- Ijerph 17 01971Document22 pagesIjerph 17 01971Ancuta PatiNo ratings yet
- Vaping: The New Wave of Nicotine Addiction: ReviewDocument10 pagesVaping: The New Wave of Nicotine Addiction: ReviewjohanNo ratings yet
- E-cigarette Health Effects Reviewed in 44 StudiesDocument6 pagesE-cigarette Health Effects Reviewed in 44 StudiesHesketh FengxianNo ratings yet
- Thesis About Cigarette AddictionDocument8 pagesThesis About Cigarette Addictionjenniferreitherspringfield100% (1)
- Research Paper About Second Hand SmokeDocument4 pagesResearch Paper About Second Hand Smokefvjebmpk100% (1)
- Electronic Cigarettes: A Primer For CliniciansDocument10 pagesElectronic Cigarettes: A Primer For Cliniciansgirish_s777No ratings yet
- Focus: Vaper, Beware: The Unique Toxicological Profile of Electronic CigarettesDocument10 pagesFocus: Vaper, Beware: The Unique Toxicological Profile of Electronic CigarettesDiana EsperanzaNo ratings yet
- Biomarkers of Tobacco Exposure Decrease After Smokers Switch To An E-Cigarette or Nicotine GumDocument9 pagesBiomarkers of Tobacco Exposure Decrease After Smokers Switch To An E-Cigarette or Nicotine GumBrent StaffordNo ratings yet
- Literature Review FinalDocument7 pagesLiterature Review Finalapi-625941419No ratings yet
- Vaping 2022 State of The Art BMJDocument15 pagesVaping 2022 State of The Art BMJgabrielnunesNo ratings yet
- Research Paper Second Hand SmokeDocument8 pagesResearch Paper Second Hand Smokeafnkeuooulejtl100% (1)
- TobaccoEcigarettes PositionPaperDocument2 pagesTobaccoEcigarettes PositionPaperPaolo RicoNo ratings yet
- Annotated Source ListDocument11 pagesAnnotated Source Listapi-512140321No ratings yet
- 2016 Article 111Document8 pages2016 Article 111Taro RahmatiaNo ratings yet
- CDC 114247 DS1Document27 pagesCDC 114247 DS1Ana Maria Guerron CabreraNo ratings yet
- Electronic Cigarettes Toxicity From Periodontal DDocument19 pagesElectronic Cigarettes Toxicity From Periodontal DRares GhimpuNo ratings yet
- The Effect of e Cigarette Aerosol Emissions On Respiratory Health A Narrative ReviewDocument18 pagesThe Effect of e Cigarette Aerosol Emissions On Respiratory Health A Narrative ReviewBrent StaffordNo ratings yet
- Electronic Cigarettes: Human Health Effects: Priscilla Callahan-LyonDocument5 pagesElectronic Cigarettes: Human Health Effects: Priscilla Callahan-Lyonbramantya andyatmaNo ratings yet
- Dangers of Vaping 03.15.2019Document23 pagesDangers of Vaping 03.15.2019Emily EresumaNo ratings yet
- Tigari ElectroniceDocument14 pagesTigari ElectroniceAdina GeorgianaNo ratings yet
- Mil Quiz Lesson 7 Q2Document7 pagesMil Quiz Lesson 7 Q2Clark DomingoNo ratings yet
- Pa 1 Persuasive EssayDocument4 pagesPa 1 Persuasive Essayapi-458023500No ratings yet
- Food Insecurity Duration: 6 HoursDocument13 pagesFood Insecurity Duration: 6 HoursLeila Mae L. InfanteNo ratings yet
- Past Examination Papers IGC2 September 2009 IGC2Document0 pagesPast Examination Papers IGC2 September 2009 IGC2bharathost100% (2)
- Fitness Tabata Interval TrainingDocument3 pagesFitness Tabata Interval TrainingKartik ChaudharyNo ratings yet
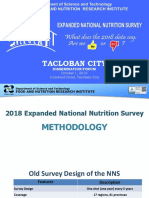
- 2018 ENNS Dissemination Tacloban CityDocument164 pages2018 ENNS Dissemination Tacloban CityJessa mae macasojotNo ratings yet
- 7 FatBurning Foods For All Day Energy 1116Document40 pages7 FatBurning Foods For All Day Energy 1116Angelo MarottaNo ratings yet
- Kliping Analitycal ExpositionDocument6 pagesKliping Analitycal ExpositionAlya SalmaNo ratings yet
- Contractor Safety Passport System CourseDocument2 pagesContractor Safety Passport System CourseTeh ArfahNo ratings yet
- Group 4: Global Recommendation On Physical ActivityDocument50 pagesGroup 4: Global Recommendation On Physical ActivityMYLE MANAYONNo ratings yet
- 1 Briefing MemoDocument2 pages1 Briefing Memoapi-240690004No ratings yet
- Combined - Training - LipidemiaDocument9 pagesCombined - Training - LipidemiaIara CruzNo ratings yet
- Personal Fitness Presentation 2-1Document38 pagesPersonal Fitness Presentation 2-1Ray Archer100% (1)
- FA3 - Contemporary WorldDocument15 pagesFA3 - Contemporary WorldGill GregorioNo ratings yet
- Policy On Tobacco Use: Latest RevisionDocument5 pagesPolicy On Tobacco Use: Latest Revisionnona aryanNo ratings yet
- Community Nutrition Intervention PDFDocument2 pagesCommunity Nutrition Intervention PDFBarbara100% (1)
- FDARDocument1 pageFDARJohn Lloyd MontecilloNo ratings yet
- Essay On Physical Fitness:Wellness:Health Related TopicDocument1 pageEssay On Physical Fitness:Wellness:Health Related TopicPaul Johann VersulaNo ratings yet
- Classroom Hazards Risk AssessmentDocument5 pagesClassroom Hazards Risk AssessmentMehrab AliNo ratings yet
- Chapter 1 Physical FitnessDocument17 pagesChapter 1 Physical FitnessYvette Marie ParenoNo ratings yet
- Slay Manage Your Stress AwayDocument3 pagesSlay Manage Your Stress AwayDix TyNo ratings yet
- Unit8 Fitt Principles TemplateDocument7 pagesUnit8 Fitt Principles Templateapi-399099520No ratings yet
- Nutrición Hospitalaria: Trabajo OriginalDocument6 pagesNutrición Hospitalaria: Trabajo OriginalJefersonNo ratings yet