You might also like
- GI Procedures and Nursing ResponsibilitiesDocument2 pagesGI Procedures and Nursing ResponsibilitiesShaina DiyaNo ratings yet
- Heart FailureDocument29 pagesHeart Failuremerin sunilNo ratings yet
- Ten Questions ICU Specialists Should Address When Managing Cardiogenic Acute Pulmonary OedemaDocument4 pagesTen Questions ICU Specialists Should Address When Managing Cardiogenic Acute Pulmonary OedemaFarmacia Del Bosque100% (1)
- Advanced Knowledge Assessment in Adult Critical CareDocument570 pagesAdvanced Knowledge Assessment in Adult Critical CareMajor EmadNo ratings yet
- Genitourinary SystemDocument8 pagesGenitourinary Systemsarguss14100% (1)
- Acute Respiratory Distress in ChildrenDocument25 pagesAcute Respiratory Distress in Childrensai ram100% (1)
- Impaired Urinary EliminationDocument2 pagesImpaired Urinary EliminationSiafei RabeNo ratings yet
- Case Scenario: Prostate CancerDocument5 pagesCase Scenario: Prostate Cancer24 PAULINO ALDRIN MUJARNo ratings yet
- Nursing Practice IDocument39 pagesNursing Practice IStephanie Abler Abellanosa100% (2)
- P1 Compilation PDFDocument56 pagesP1 Compilation PDFJames Eugene CaasiNo ratings yet
- NCP GbsDocument2 pagesNCP GbsJaylord VerazonNo ratings yet
- Surgical Atlas Transureteroureterostomy: John M. BarryDocument7 pagesSurgical Atlas Transureteroureterostomy: John M. BarrycristiangelsNo ratings yet
- Nursing Care Plan For Pulmonary Edema PDFDocument2 pagesNursing Care Plan For Pulmonary Edema PDFAsmaa100% (1)
- NCM 112 Eval ExamDocument11 pagesNCM 112 Eval ExamMartin T Manuel100% (1)
- 3 MerilDocument1 page3 MerilGuntur Aji PrasetyoNo ratings yet
- Nursing Care Plan: RationaleDocument5 pagesNursing Care Plan: Rationalerona-chanNo ratings yet
- UrinaryDocument19 pagesUrinaryfiel borataNo ratings yet
- Nursing Care Planning FINALDocument4 pagesNursing Care Planning FINALLizli LoredoNo ratings yet
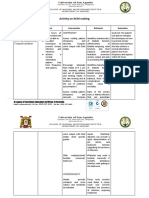
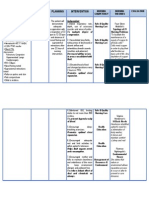
- Activity On NCM MakingDocument4 pagesActivity On NCM MakingJollan Marie BuenvenidaNo ratings yet
- Impaired Urinary EliminationDocument2 pagesImpaired Urinary EliminationMatty-b AskalaniNo ratings yet
- Urinary Tract PDFDocument2 pagesUrinary Tract PDFVette Angelikka Dela CruzNo ratings yet
- Benign Prostatic HyperplasiaDocument3 pagesBenign Prostatic HyperplasiaBebeness MoNo ratings yet
- CARE PLAN Urinary ObstructionDocument2 pagesCARE PLAN Urinary Obstructionjinsi georgeNo ratings yet
- Assignment in NCM 106 LectureDocument6 pagesAssignment in NCM 106 LectureJeanessa Delantar QuilisadioNo ratings yet
- Investigation JF The Urinary TractDocument139 pagesInvestigation JF The Urinary TractВладимир КурпаянидиNo ratings yet
- Urinary Incontinence - MKLDocument42 pagesUrinary Incontinence - MKLFreeburn SimunchembuNo ratings yet
- Intravenous Pyelography: Week 5Document2 pagesIntravenous Pyelography: Week 5Shaina Angelique SaliNo ratings yet
- (2nd Half) Mind Mapping TAHDocument4 pages(2nd Half) Mind Mapping TAHjnetNo ratings yet
- Fibroscan® and Transient Elastography: What Are The Indications For This Test?Document4 pagesFibroscan® and Transient Elastography: What Are The Indications For This Test?Clarisa AnindyaNo ratings yet
- NCP Pedia RotDocument5 pagesNCP Pedia RotGian kyle AradillosNo ratings yet
- Vuj ObstructionDocument2 pagesVuj ObstructionMuhammad FarhanNo ratings yet
- Urethral Stricture Disease: Evaluation of The Male UrethraDocument5 pagesUrethral Stricture Disease: Evaluation of The Male UrethraCentanarianNo ratings yet
- Aquino NCP UtiDocument3 pagesAquino NCP UtiGianne ObaldoNo ratings yet
- CARE PLANs Renal StoneDocument5 pagesCARE PLANs Renal Stonejinsi georgeNo ratings yet
- Committee Opinion: Evaluation of Uncomplicated Stress Urinary Incontinence in Women Before Surgical TreatmentDocument5 pagesCommittee Opinion: Evaluation of Uncomplicated Stress Urinary Incontinence in Women Before Surgical Treatmentw yNo ratings yet
- Diagnostic Studies - GI BleedingDocument21 pagesDiagnostic Studies - GI BleedingnoemilauNo ratings yet
- Institute of Nursing and Allied Health Education: Cabanatuan City, Nueva Ecija, Philippines 3100Document14 pagesInstitute of Nursing and Allied Health Education: Cabanatuan City, Nueva Ecija, Philippines 3100Potato BananaNo ratings yet
- Repro System NotesDocument13 pagesRepro System NotesAraw GabiNo ratings yet
- Prioritization of Problems Rank Problem Identified: San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesDocument5 pagesPrioritization of Problems Rank Problem Identified: San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesTom CuencaNo ratings yet
- Hydraulic UrethralDocument2 pagesHydraulic UrethralMalgorzata LisowskaNo ratings yet
- NCPDocument2 pagesNCPbulok netflakesNo ratings yet
- Artigotutoria PDFDocument12 pagesArtigotutoria PDFZARA BATISTANo ratings yet
- Silvaqueenie Rose Multiple SclerosisDocument5 pagesSilvaqueenie Rose Multiple SclerosisQueenie SilvaNo ratings yet
- Nursing of Urinary System: Hema Malini, S.KP, MN, PHDDocument4 pagesNursing of Urinary System: Hema Malini, S.KP, MN, PHDmutia ilhamNo ratings yet
- Alteration of The Starling Forces Which Control Transfer of Fluid From The Vascular Compartment To Surrounding Tissue SpacesDocument3 pagesAlteration of The Starling Forces Which Control Transfer of Fluid From The Vascular Compartment To Surrounding Tissue SpacesNicole cuencosNo ratings yet
- Risk For Decreased Cardiac Tissue PerfusionDocument3 pagesRisk For Decreased Cardiac Tissue PerfusionKarina MadriagaNo ratings yet
- Chest Drainage ChecklistDocument4 pagesChest Drainage Checklistjon elleNo ratings yet
- NCP Metro San JoseDocument8 pagesNCP Metro San JosePrincess NavarroNo ratings yet
- Total Abdominal Hysterectomy Bilateral Salpingo Oophorectomy (Tahbso) Nursing Responsibilities Rationale Pre-OperativeDocument4 pagesTotal Abdominal Hysterectomy Bilateral Salpingo Oophorectomy (Tahbso) Nursing Responsibilities Rationale Pre-OperativeMiar QuestNo ratings yet
- 22-Bladder CatheterizationDocument16 pages22-Bladder CatheterizationmeewhayNo ratings yet
- Creog Urogyn ReviewDocument97 pagesCreog Urogyn ReviewAlexandriah AlasNo ratings yet
- Urinary TractDocument3 pagesUrinary TractRifki MuhamadNo ratings yet
- Clinical Review: Managing Urinary Incontinence in Older PeopleDocument15 pagesClinical Review: Managing Urinary Incontinence in Older PeopleMatthias WollfNo ratings yet
- Urinary Diversions: A Primer of The Surgical Techniques and Imaging FindingsDocument12 pagesUrinary Diversions: A Primer of The Surgical Techniques and Imaging FindingsMCFNo ratings yet
- Surgery of Reproductive, Urinary, and OrthopedicsDocument3 pagesSurgery of Reproductive, Urinary, and Orthopedicsancheta.alleahjean.oNo ratings yet
- Ob NCP 2Document2 pagesOb NCP 2Kimberly Mondala (SHS)No ratings yet
- CARE PLANs BPHDocument5 pagesCARE PLANs BPHjinsi georgeNo ratings yet
- Litho Trips yDocument1 pageLitho Trips yRed StohlNo ratings yet
- Imaging of The Genitourinary Tract: Mashuri, DR.,SP - Rad.,M.KesDocument90 pagesImaging of The Genitourinary Tract: Mashuri, DR.,SP - Rad.,M.KesmirzasullivanNo ratings yet
- NCP - Mod9Document3 pagesNCP - Mod9designericlelynsoronioNo ratings yet
- Prostatic CancerDocument3 pagesProstatic CancerShakour El seifyNo ratings yet
- Nursing Implications For Diagnostic Tests: Bone Scan and Gallium ScanDocument1 pageNursing Implications For Diagnostic Tests: Bone Scan and Gallium ScanAnisa JamitoNo ratings yet
- Adult MegaureterDocument25 pagesAdult MegaureterSonntagsschule St. Antonius Kloster in KröffelbachNo ratings yet
- Fluoroscopy & AngiographyDocument2 pagesFluoroscopy & AngiographyPilar FernandezNo ratings yet
- Ureteroscpy 1Document2 pagesUreteroscpy 1Fareed ShahwaniNo ratings yet
- NURSING CARE PLAN - Impaired Urinary EliminationDocument2 pagesNURSING CARE PLAN - Impaired Urinary EliminationDaniel Andre S. SomorayNo ratings yet
- Investigations of The Urinary System: Group 4Document53 pagesInvestigations of The Urinary System: Group 4YvonneNo ratings yet
- Interpretation of Urodynamic Studies: A Case Study-Based GuideFrom EverandInterpretation of Urodynamic Studies: A Case Study-Based GuideNo ratings yet
- Shock SIRS & MODS - Lewis Flashcards - QuizletDocument17 pagesShock SIRS & MODS - Lewis Flashcards - QuizletNursyNurseNo ratings yet
- Como Optimizar La EntubaciónDocument4 pagesComo Optimizar La EntubaciónKaren Aline Gómez CruzNo ratings yet
- BLUE & FALLS Protocol LichensteinDocument12 pagesBLUE & FALLS Protocol LichensteinCarlos MoncayoNo ratings yet
- Acute Respiratory FailureDocument28 pagesAcute Respiratory FailureMohamed Na3eemNo ratings yet
- Managing Covid 19 Patients Nurses Role and ConsiderationsDocument7 pagesManaging Covid 19 Patients Nurses Role and ConsiderationsSimona Marcela ȚibuleacNo ratings yet
- 5.respiratory Distress Dental LectureDocument40 pages5.respiratory Distress Dental LecturehaneeneeNo ratings yet
- IMS MCQ Bank 2023 VXDocument28 pagesIMS MCQ Bank 2023 VXAbdulrahman AlharbiNo ratings yet
- HFA Position Papers 2019Document264 pagesHFA Position Papers 2019Irina Cabac-PogoreviciNo ratings yet
- Philosophy of Critical Care NursingDocument5 pagesPhilosophy of Critical Care NursingAICEL A. ABILNo ratings yet
- Congestive Heart FailureDocument43 pagesCongestive Heart Failure568563100% (1)
- Case NCPDocument25 pagesCase NCPJoher Bolante Mendez100% (1)
- Blood Volume Prior To and Following Treatment of Acute Cardiogenic Pulmonary EdemaDocument8 pagesBlood Volume Prior To and Following Treatment of Acute Cardiogenic Pulmonary EdemaBagus MahendraNo ratings yet
- Respiratory Plab 1 Notes 2014: SamsonDocument19 pagesRespiratory Plab 1 Notes 2014: Samsonزكريا عمرNo ratings yet
- Egans Chapter 27 Workbook Answer KeyDocument11 pagesEgans Chapter 27 Workbook Answer KeyStevenPaulDaclesNo ratings yet
- Postural DrainageDocument7 pagesPostural DrainagemohtishimNo ratings yet
- Nur 111 Session 2 Sas 1Document10 pagesNur 111 Session 2 Sas 1Zzimply Tri Sha UmaliNo ratings yet
- Albumin Solution - Drug Information - UpToDateDocument15 pagesAlbumin Solution - Drug Information - UpToDateSuci WijayaNo ratings yet
- Tips On How To Answer An Essay Question by Doaa Kamal 2001Document9 pagesTips On How To Answer An Essay Question by Doaa Kamal 2001Amr El TaherNo ratings yet
- By: Darryl Jamison Macon County EMS Training CoordinatorDocument53 pagesBy: Darryl Jamison Macon County EMS Training Coordinatorsharin143No ratings yet
- Trauma Respuesta Ishikawa2013Document7 pagesTrauma Respuesta Ishikawa2013María José BencomoNo ratings yet
- Ca 2 Cardiovascular-Oxygenation Assignment Part 1Document8 pagesCa 2 Cardiovascular-Oxygenation Assignment Part 1Joseph AbangNo ratings yet
- Management of Cardiogenic Shock After Acute - 2023Document10 pagesManagement of Cardiogenic Shock After Acute - 2023Angy KarakostaNo ratings yet