You might also like
- 1442 1 FullDocument1 page1442 1 FullmuamarrayNo ratings yet
- TOR SEMNAS KARAkTER 4 2018Document6 pagesTOR SEMNAS KARAkTER 4 2018Rosyid PrasetyoNo ratings yet
- Urticaria CronicaDocument5 pagesUrticaria CronicaalejandraNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 15: MusculoskeletalFrom EverandComplementary and Alternative Medical Lab Testing Part 15: MusculoskeletalNo ratings yet
- TH 17Document11 pagesTH 17hendarto ArifNo ratings yet
- Hydroxychloroquine Suppresses Interferon-Inducible GenesDocument5 pagesHydroxychloroquine Suppresses Interferon-Inducible GenesamilyapraditaNo ratings yet
- Cei 13095Document6 pagesCei 13095karen rinconNo ratings yet
- 7051-Article Text-20588-1-10-20160303Document6 pages7051-Article Text-20588-1-10-20160303Mark JakoNo ratings yet
- ArchRheumatol 32 21Document5 pagesArchRheumatol 32 21indriNo ratings yet
- Ar 3370Document9 pagesAr 3370Juan Manuel GonzálezNo ratings yet
- Serum Levels of TNF-and IL-18 in Patients With Active Psoriasis and Correlation With Disease SeverityDocument7 pagesSerum Levels of TNF-and IL-18 in Patients With Active Psoriasis and Correlation With Disease SeverityAgus PrimaNo ratings yet
- Para Tradudir Ejercisios y Espondilitis AnquilosanteDocument10 pagesPara Tradudir Ejercisios y Espondilitis AnquilosanteCarla Bocca MoralesNo ratings yet
- ArticleDocument11 pagesArticletgayuNo ratings yet
- Serum IGF-1 in Patients With Rheumatoid Arthritis: Correlation With Disease ActivityDocument9 pagesSerum IGF-1 in Patients With Rheumatoid Arthritis: Correlation With Disease ActivityMuhammad Rizky Anugrah PratamaNo ratings yet
- 93 - 08 Bantar 7 Hal 306-312Document7 pages93 - 08 Bantar 7 Hal 306-312amilyapraditaNo ratings yet
- Zhang Et Al-2016-Journal of Magnetic Resonance ImagingDocument8 pagesZhang Et Al-2016-Journal of Magnetic Resonance ImagingMarisol AcostaNo ratings yet
- Expression of Interleukin-22 in Myasthenia Gravis: HumanimmunologyDocument10 pagesExpression of Interleukin-22 in Myasthenia Gravis: HumanimmunologyAriefPratamaNo ratings yet
- Calin 2004 PDFDocument8 pagesCalin 2004 PDFRafaela Queiroz MascarenhasNo ratings yet
- Acupuntura para La RodillaDocument9 pagesAcupuntura para La Rodillaoscarin123456789No ratings yet
- Ferrara 2003Document8 pagesFerrara 2003Chaima DjabouNo ratings yet
- Anti-C1q Antibodies: Association With Nephritis and Disease Activity in Systemic Lupus ErythematosusDocument5 pagesAnti-C1q Antibodies: Association With Nephritis and Disease Activity in Systemic Lupus ErythematosusAlisNo ratings yet
- Antioxidant Potential of The Blood in Men With Obstructive Sleep Breathing DisordersDocument3 pagesAntioxidant Potential of The Blood in Men With Obstructive Sleep Breathing DisorderslakjdlkaNo ratings yet
- Ordi-Ros J, Et Al, 2017.Document8 pagesOrdi-Ros J, Et Al, 2017.Suhenri SiahaanNo ratings yet
- Defining The Phenotype, Pathogenesis and Treatment of Crohn'sDocument12 pagesDefining The Phenotype, Pathogenesis and Treatment of Crohn'sJEAN CERNA SOLISNo ratings yet
- AbsrectDocument10 pagesAbsrectRufaq UllahNo ratings yet
- Targeting Inflammatory Pathways in Axial SpondyloarthritisDocument30 pagesTargeting Inflammatory Pathways in Axial SpondyloarthritismsrappNo ratings yet
- SIMI - Volume Comunicazioni Orali e PosterDocument212 pagesSIMI - Volume Comunicazioni Orali e Postermaria wahyuniNo ratings yet
- Hla-B27 Allele Connotation Amongst Individuals Conjectured of Spondyloarthritis (SPA) in PakistanDocument7 pagesHla-B27 Allele Connotation Amongst Individuals Conjectured of Spondyloarthritis (SPA) in PakistancismarcivNo ratings yet
- Inflammatory Mediators Drive Neuroinflammation in Autism Spectrum Disorder and Cerebral PalsyDocument11 pagesInflammatory Mediators Drive Neuroinflammation in Autism Spectrum Disorder and Cerebral PalsyDanilo AssisNo ratings yet
- Journal of Functional Foods: Qinlu Lin, Wang Liao, Jie Bai, Wei Wu, Jianping WuDocument6 pagesJournal of Functional Foods: Qinlu Lin, Wang Liao, Jie Bai, Wei Wu, Jianping Wusuci apsari pebriantiNo ratings yet
- Khannasharma 2017Document7 pagesKhannasharma 2017Imam IskandarNo ratings yet
- JDM - Amezcua-Guerra Et Al 2017Document8 pagesJDM - Amezcua-Guerra Et Al 2017Ricardo Colín MartínezNo ratings yet
- Immunobiology: Chunfeng Ren, Jie Chen, Qincheng Che, Qian Jia, Hongqin Lu, Xiaoyan Qi, Xiaojie Zhang, Qiang ShuDocument8 pagesImmunobiology: Chunfeng Ren, Jie Chen, Qincheng Che, Qian Jia, Hongqin Lu, Xiaoyan Qi, Xiaojie Zhang, Qiang Shu马三强No ratings yet
- Osteopontin Mediated Eosinophils ActivationDocument7 pagesOsteopontin Mediated Eosinophils ActivationEDGAR FUENMAYOR PIRELANo ratings yet
- Sindrom NefrotikDocument8 pagesSindrom NefrotikDania SaraswatiNo ratings yet
- Prevalence of and Factors Associated With Sarcopenia Among Elderly Individuals With HypertensionDocument10 pagesPrevalence of and Factors Associated With Sarcopenia Among Elderly Individuals With HypertensionZaskia PutriNo ratings yet
- Marchese 2019 Controlled Study of Central Hemodynamic ChangesDocument8 pagesMarchese 2019 Controlled Study of Central Hemodynamic Changestaaaatan.04No ratings yet
- Guillain Barr Syndrome Occurring Synchronously With Systemic Lupus Erythematosus As Initial Manifestation Treated Successfully With Low DoseDocument5 pagesGuillain Barr Syndrome Occurring Synchronously With Systemic Lupus Erythematosus As Initial Manifestation Treated Successfully With Low DoseTessa CruzNo ratings yet
- ThrombomodulinDocument6 pagesThrombomodulinAlisNo ratings yet
- Fimmu 13 888644Document12 pagesFimmu 13 888644VedantNo ratings yet
- Journal Homepage: - : IntroductionDocument3 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- The Effect of Acute Psychologic Stress On Systemic and Rectal Mucosal Measures of in Ammation in Ulcerative ColitisDocument10 pagesThe Effect of Acute Psychologic Stress On Systemic and Rectal Mucosal Measures of in Ammation in Ulcerative ColitisNejc KovačNo ratings yet
- Vincent 2007Document9 pagesVincent 20071766636545No ratings yet
- Papr 12544Document11 pagesPapr 12544Michael HuntNo ratings yet
- Artigo Base SimoneDocument5 pagesArtigo Base SimoneWolfgang ThyerreNo ratings yet
- Acupuncture-Based ModalitiesDocument9 pagesAcupuncture-Based ModalitiesFelipe MaiaNo ratings yet
- Neutrophils-Lymphocytes Ratio (NLR) and Platelet-Lymphocytes Ratio (PLR) As Predictors of NSTEMI EventDocument9 pagesNeutrophils-Lymphocytes Ratio (NLR) and Platelet-Lymphocytes Ratio (PLR) As Predictors of NSTEMI EventYohanes FirmansyahNo ratings yet
- Age and Insulin Resistance Faccini 2001Document5 pagesAge and Insulin Resistance Faccini 2001MukhlidahHanunSiregarNo ratings yet
- Ijem 122553Document6 pagesIjem 122553Munawwar SaukaniNo ratings yet
- Original Article: Rizkiditia Nugraha Hadian, Renaldi Prasetia, Ahmad FariedDocument4 pagesOriginal Article: Rizkiditia Nugraha Hadian, Renaldi Prasetia, Ahmad FariedEka PutriNo ratings yet
- RJR - 2019 - 3 - Art-02 - CRISTINA GOFITA - CRPS DIAGNOSISDocument8 pagesRJR - 2019 - 3 - Art-02 - CRISTINA GOFITA - CRPS DIAGNOSISmihail.boldeanuNo ratings yet
- Rodriguez G - Serum ACE Activity in Normal Children and in Those With SarcoidosisDocument5 pagesRodriguez G - Serum ACE Activity in Normal Children and in Those With SarcoidosisPhaimNo ratings yet
- Case ReportDocument5 pagesCase ReportsyahputriNo ratings yet
- 2021 - Brazilian Recomendations For The Use of NSAID in Axial SpondyloarthritisDocument21 pages2021 - Brazilian Recomendations For The Use of NSAID in Axial SpondyloarthritisGustavo ResendeNo ratings yet
- Anti-Double-Stranded DNA Isotypes and Anti-C1q Antibody Improve The Diagnostic Specificity of SLEDocument8 pagesAnti-Double-Stranded DNA Isotypes and Anti-C1q Antibody Improve The Diagnostic Specificity of SLEPuri RahmawatiNo ratings yet
- The Molar Ratio of Total Branched-Chain Amino Acids To Tyrosine Predicts A Digit Symbol Test Abnormality in Cirrhotic PatientsDocument11 pagesThe Molar Ratio of Total Branched-Chain Amino Acids To Tyrosine Predicts A Digit Symbol Test Abnormality in Cirrhotic PatientsThinh VinhNo ratings yet
- Editorial: Complications of DiabetesDocument6 pagesEditorial: Complications of DiabetesYULISSA FLORES RONDONNo ratings yet
- The Clinical and Immunologic Effects of AcetylcystDocument2 pagesThe Clinical and Immunologic Effects of Acetylcystفرجني موغNo ratings yet
- Quality of Life in The Classic and Hyper20160418-442-Si8xbf-With-cover-page-V2Document3 pagesQuality of Life in The Classic and Hyper20160418-442-Si8xbf-With-cover-page-V2Aide SeanezNo ratings yet
- High Salivary Soluble L-Selectin and Interleukin-7 Levels in Asian Indian Patients With Primary Sjögren's SyndromeDocument5 pagesHigh Salivary Soluble L-Selectin and Interleukin-7 Levels in Asian Indian Patients With Primary Sjögren's SyndromeMaite Fernanda CuturrufoNo ratings yet
- In Ammatory Markers: Single Panel Test CartridgeDocument2 pagesIn Ammatory Markers: Single Panel Test CartridgeHussein MohamedNo ratings yet
- Rheumatoid ArthritisDocument6 pagesRheumatoid ArthritisJayson Cruz100% (2)
- Diagnosis and Prevention of Iron Deficiency and Iron-Deficiency Anemia in Infants and Young ChildrenDocument16 pagesDiagnosis and Prevention of Iron Deficiency and Iron-Deficiency Anemia in Infants and Young ChildrenAnwesa Priyadarsini PradhanNo ratings yet
- WSES Jerusalem Guidelines For Diagnosis and Treatment of Acute AppendicitisDocument25 pagesWSES Jerusalem Guidelines For Diagnosis and Treatment of Acute AppendicitisRenatoMendozaNo ratings yet
- 0007BDocument12 pages0007BnacerNo ratings yet
- Il 6Document5 pagesIl 6Suresh KumawatNo ratings yet
- Inmunonutricion COVID 2021 DestacadoDocument7 pagesInmunonutricion COVID 2021 DestacadoNoemí RojasNo ratings yet
- Clinical Manifestations and Diagnosis of Acute PancreatitisDocument31 pagesClinical Manifestations and Diagnosis of Acute PancreatitisBrian WilliamNo ratings yet
- Complete Report OAPR-77102 Praveen 29aug2019Document13 pagesComplete Report OAPR-77102 Praveen 29aug2019Praveen MNNo ratings yet
- Crohn's DiseaseDocument8 pagesCrohn's DiseaseibrahimNo ratings yet
- S53 - Syed Kashif Ghani-Fpsc Zakir Nagar: Patientreportscsuperpanel - General - Panel - Analyte - SC (Version: 6)Document11 pagesS53 - Syed Kashif Ghani-Fpsc Zakir Nagar: Patientreportscsuperpanel - General - Panel - Analyte - SC (Version: 6)Khalid Mohammad Khalid TanwiriNo ratings yet
- Malnutrition Case Study-2Document5 pagesMalnutrition Case Study-2dakota100% (1)
- Neuro Ophthalmology An Issue of Neurologic Clinics The Clinics Internal MedicineDocument284 pagesNeuro Ophthalmology An Issue of Neurologic Clinics The Clinics Internal MedicineKathleene100% (1)
- Cardiovascular Benefits and Risks of Moderate Alcohol Consumption - UpToDateDocument17 pagesCardiovascular Benefits and Risks of Moderate Alcohol Consumption - UpToDateAnca StanNo ratings yet
- Lycopene and Heart HealthDocument8 pagesLycopene and Heart HealthDr. HeleNo ratings yet
- Guideline PancreatitisDocument39 pagesGuideline Pancreatitisanda_No ratings yet
- LPL - PSC Sant Nagar (Burari) Maharaja Agrasen Complex, Main Burari Ro Ad, Sant Nagar, Burari Delhi Sharma - Har1 DelhiDocument4 pagesLPL - PSC Sant Nagar (Burari) Maharaja Agrasen Complex, Main Burari Ro Ad, Sant Nagar, Burari Delhi Sharma - Har1 DelhiarpanNo ratings yet
- INS CR EN CRP Rev.22 - 181109Document3 pagesINS CR EN CRP Rev.22 - 181109Ahmed Ben NjahNo ratings yet
- CH 063 STG Multisystem Inflammatory Syndrome in ChildrenDocument8 pagesCH 063 STG Multisystem Inflammatory Syndrome in ChildrenAarathi raoNo ratings yet
- FIA Meter Plus: Fluorescence Immunoassay Rapid Quantitative TestDocument4 pagesFIA Meter Plus: Fluorescence Immunoassay Rapid Quantitative TestWawan HardjomulionoNo ratings yet
- Fpsyt 12 804269Document10 pagesFpsyt 12 804269Sahadevan NairNo ratings yet
- 1-Aarogyam B + Covid Ab IgG - PO3827226873-180Document16 pages1-Aarogyam B + Covid Ab IgG - PO3827226873-180Rohit PandeyNo ratings yet
- BioTrust LeptiBurn BreakdownDocument7 pagesBioTrust LeptiBurn BreakdownL LNo ratings yet
- Pediatric Osteomyelitis: Annisa Nur ArifinDocument18 pagesPediatric Osteomyelitis: Annisa Nur ArifinWahyu Adhitya PrawirasatraNo ratings yet
- EVMS Critical Care COVID-19 ProtocolDocument23 pagesEVMS Critical Care COVID-19 ProtocoldarwinNo ratings yet
- Comparison of Inflammatory Markers in HTNDocument6 pagesComparison of Inflammatory Markers in HTNDan JohnstonNo ratings yet
- T. Akahoshi H. Sugimori N. Kaku K. Tokuda T. Nagata E. Noda M. Morita M. Hashizume Y. MaeharaDocument8 pagesT. Akahoshi H. Sugimori N. Kaku K. Tokuda T. Nagata E. Noda M. Morita M. Hashizume Y. Maeharadr. Ayu Nabila Kusuma PradanaNo ratings yet
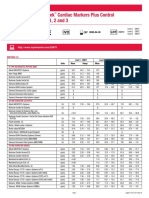
- Liquichek Cardiac Markers Plus Control Levels 1, 2 and 3: MethodDocument4 pagesLiquichek Cardiac Markers Plus Control Levels 1, 2 and 3: MethodSaifoel RahmanNo ratings yet
- Coronary Artery AtherosclerosisDocument25 pagesCoronary Artery AtherosclerosisShahrizal Che JamelNo ratings yet
- VivaChek Bio Products Catalog (En) 092421Document14 pagesVivaChek Bio Products Catalog (En) 092421Emmanuel BonillaNo ratings yet