You might also like
- The Ammonicarb Operation Book Format 4 PDF FreeDocument149 pagesThe Ammonicarb Operation Book Format 4 PDF FreePantelis Krintz100% (1)
- Clandestine InfoDocument115 pagesClandestine Infoxathrid369100% (5)
- Naproxen Patch TransdermalDocument9 pagesNaproxen Patch Transdermalnurhayati novitaNo ratings yet
- Interpol Review of Controlled Substances Review 20Document62 pagesInterpol Review of Controlled Substances Review 20ORLANDO CASTILLO100% (2)
- Guidelines Remediation Clandestine Meth Lab SitesDocument173 pagesGuidelines Remediation Clandestine Meth Lab SitesJonathan MerrittNo ratings yet
- MPJE NSU Dr. Seamon 2022Document134 pagesMPJE NSU Dr. Seamon 2022Tammy100% (1)
- Ma Huang Ephedrae Herba Setting The Record StraightDocument13 pagesMa Huang Ephedrae Herba Setting The Record StraighttiaraNo ratings yet
- 1 s2.0 S2589871X22000882 MainDocument44 pages1 s2.0 S2589871X22000882 MainGregory AssonitisNo ratings yet
- Dai 2020Document7 pagesDai 2020yalocim666No ratings yet
- My EPQDocument20 pagesMy EPQAnthony Sa'id0% (1)
- 1947-489X 210755Document9 pages1947-489X 210755게임 뉴비에 게임 모험No ratings yet
- Earwax As An Alternative Specimen For Forensic AnalysisDocument11 pagesEarwax As An Alternative Specimen For Forensic AnalysisNAYARA MOREIRA DAMASCENONo ratings yet
- Molecules: Recent Trends in Pharmaceutical Analytical ChemistryDocument4 pagesMolecules: Recent Trends in Pharmaceutical Analytical ChemistryLhorruama DiasNo ratings yet
- Epilepsia - 2009 - La Marca - A New Rapid Micromethod For The Assay of Phenobarbital From Dried Blood Spots by LC TandemDocument5 pagesEpilepsia - 2009 - La Marca - A New Rapid Micromethod For The Assay of Phenobarbital From Dried Blood Spots by LC TandemWaode RahmahNo ratings yet
- Study On The Sampling of Methadone From ExhaledDocument8 pagesStudy On The Sampling of Methadone From Exhaledkassim AliNo ratings yet
- Journal Pone 0074584Document13 pagesJournal Pone 0074584Devy dwianaiNo ratings yet
- Articlealdehydes Hyg Med 2006 Van DrongelenDocument5 pagesArticlealdehydes Hyg Med 2006 Van DrongelenOMAR EL HAMDAOUINo ratings yet
- Ritscher 2019Document10 pagesRitscher 2019maxsmaxNo ratings yet
- Screening For Drugs of Abuse. II Cannabinoids, Lysergic Acid Diethylamide, Buprenorphine, Methadone, Barbiturates, Benzodiazepines and Other DrugsDocument51 pagesScreening For Drugs of Abuse. II Cannabinoids, Lysergic Acid Diethylamide, Buprenorphine, Methadone, Barbiturates, Benzodiazepines and Other DrugsRafal RogalewiczNo ratings yet
- Cromatografía 2Document13 pagesCromatografía 2Lau CondeNo ratings yet
- Determinación de Antimonio QumicaNovaDocument10 pagesDeterminación de Antimonio QumicaNovajose fernando ovalles duranNo ratings yet
- 2018 Wastewater-Based Tracing of Doping Use by The General Population and Amateur AthletesDocument11 pages2018 Wastewater-Based Tracing of Doping Use by The General Population and Amateur Athleteskryylmz.tNo ratings yet
- The Stability of Heroin Metabolites and Adulterants in Blood To Evaluate Role of The Stability On Postmortem RedistributionDocument7 pagesThe Stability of Heroin Metabolites and Adulterants in Blood To Evaluate Role of The Stability On Postmortem RedistributionIJAR JOURNALNo ratings yet
- Impact of Estrogen Type On Cardiovascular Safety of Combined OralDocument12 pagesImpact of Estrogen Type On Cardiovascular Safety of Combined OralMary SuescaNo ratings yet
- WRC ReportDocument613 pagesWRC ReportAnup SharmaNo ratings yet
- Journal Pre-Proof: European Journal of PharmacologyDocument34 pagesJournal Pre-Proof: European Journal of Pharmacologymanisha thakurNo ratings yet
- Wang 2020Document17 pagesWang 2020Maria VieiraNo ratings yet
- Determination of Synthetic Hallucinogens in Oral Fluids by Microextraction by Packed Sorbent and Liquid Chromatography-Tandem Mass SpectrometryDocument11 pagesDetermination of Synthetic Hallucinogens in Oral Fluids by Microextraction by Packed Sorbent and Liquid Chromatography-Tandem Mass Spectrometryyulis9777No ratings yet
- Eric Chen, Canyon Crest Academy, San Diego, CADocument1 pageEric Chen, Canyon Crest Academy, San Diego, CAAdrian GreenNo ratings yet
- Abendazol 2Document6 pagesAbendazol 2Agung WijayantoNo ratings yet
- Nanotechnology in Forensic Toxicology: How The Little Guys Are Giving Us The Big PictureDocument14 pagesNanotechnology in Forensic Toxicology: How The Little Guys Are Giving Us The Big PictureVickie KapNo ratings yet
- The Relationship Between Oxidant-Antioxidant Status and Bronchial Obstructive Parameters in Patients With COPDDocument4 pagesThe Relationship Between Oxidant-Antioxidant Status and Bronchial Obstructive Parameters in Patients With COPDOyunbiligt BaatarNo ratings yet
- Comparison of The Use of A Dry Chemistry Analyser in Primary Care in Norway and The United KingdomDocument6 pagesComparison of The Use of A Dry Chemistry Analyser in Primary Care in Norway and The United KingdomWaleed KhalidNo ratings yet
- Degel 1996Document12 pagesDegel 1996Alexsandro Nicolay PontoanNo ratings yet
- Bioequivalence Study of Two Formulations of Bisoprolol Fumarate Tablets in Healthy SubjectsDocument7 pagesBioequivalence Study of Two Formulations of Bisoprolol Fumarate Tablets in Healthy SubjectsSan-Clin-Eq LaboratoryNo ratings yet
- Validated Spectrophotometric Method For The Estimation of Vincristine and VinblastineDocument10 pagesValidated Spectrophotometric Method For The Estimation of Vincristine and VinblastineEL HASSAN AARIFNo ratings yet
- Limulus Amoebocyte Lysate (Lal) Test - An Alternative Method For Detection of Bacterial EndotoxinsDocument6 pagesLimulus Amoebocyte Lysate (Lal) Test - An Alternative Method For Detection of Bacterial EndotoxinsOula HatahetNo ratings yet
- Ijms 22 03573 v2Document20 pagesIjms 22 03573 v2Mohammed Shuaib KhanNo ratings yet
- Journal of Chromatographic Science 54 (7) 1153-1158Document7 pagesJournal of Chromatographic Science 54 (7) 1153-1158Xime Martinez PobleteNo ratings yet
- Ref 5 Single Bead Investigation Ahnfelt 2018Document13 pagesRef 5 Single Bead Investigation Ahnfelt 2018ณพดนัย จักรภีร์ศิริสุขNo ratings yet
- 1 Reverse HPLC Method BudesonideDocument11 pages1 Reverse HPLC Method Budesonidenonick18No ratings yet
- L. CanabinoidDocument10 pagesL. CanabinoidRoxana StanNo ratings yet
- Gcms ProposalDocument8 pagesGcms Proposalapi-281150432No ratings yet
- TMP CDA4Document5 pagesTMP CDA4FrontiersNo ratings yet
- Simultaneous Determination Ofloxacin + Ornidazole - SpectrophotometricDocument6 pagesSimultaneous Determination Ofloxacin + Ornidazole - SpectrophotometricNájla KassabNo ratings yet
- 1 s2.0 S1386142522002141 MainDocument9 pages1 s2.0 S1386142522002141 MainArijit DuttaNo ratings yet
- Characterization of The Designer Benzodiazepine Pyrazolam and Its Detectability in Human Serum and UrineDocument9 pagesCharacterization of The Designer Benzodiazepine Pyrazolam and Its Detectability in Human Serum and UrineAnonymous 4KaJRMNo ratings yet
- Development and Validation of A Simple HPLC Method For Simultaneous in Vitro Determination of Amoxicillin and Metronidazole at Single WavelengthDocument5 pagesDevelopment and Validation of A Simple HPLC Method For Simultaneous in Vitro Determination of Amoxicillin and Metronidazole at Single WavelengthAnkit VishnoiNo ratings yet
- 7458-Article Text-13623-1-10-20181026Document9 pages7458-Article Text-13623-1-10-20181026Yahia MasriNo ratings yet
- Spirometry in Chronic Obstructive Pulmonary Disease in Norwegian General PracticeDocument6 pagesSpirometry in Chronic Obstructive Pulmonary Disease in Norwegian General PracticeNimas ChanNo ratings yet
- Solubility of Budesonide, Hydrocortisone, and Prednisolone in Ethanol + Water Mixtures at 298.2 KDocument90 pagesSolubility of Budesonide, Hydrocortisone, and Prednisolone in Ethanol + Water Mixtures at 298.2 KsekahaNo ratings yet
- Fluorescence PaperDocument15 pagesFluorescence Papernisar khanNo ratings yet
- Rapid, Simple and Selective Determination of 2,4-Dinitrophenol byDocument3 pagesRapid, Simple and Selective Determination of 2,4-Dinitrophenol byAnna Carolina MachadoNo ratings yet
- Shahsavari Et Al, 2017Document7 pagesShahsavari Et Al, 2017Ramu RacikNo ratings yet
- Southern Chinese Children Chromatography Sampling: Breath Hydrogen Novel Automatic SystemDocument10 pagesSouthern Chinese Children Chromatography Sampling: Breath Hydrogen Novel Automatic Systemraisya farah monicaNo ratings yet
- What Can Radio Isotopes Do For Man?: Medicine and BiologyDocument10 pagesWhat Can Radio Isotopes Do For Man?: Medicine and Biologyvasukimp572No ratings yet
- 3 ArsDocument12 pages3 Arsfoaad foaadNo ratings yet
- Lal Test An Alternative Method For Detection of Bacterial EndotoxinsDocument6 pagesLal Test An Alternative Method For Detection of Bacterial EndotoxinsStanislaw YohanNo ratings yet
- Doping Control Analysis of 46 Polar Drugs in Horse Plasma and UrineDocument9 pagesDoping Control Analysis of 46 Polar Drugs in Horse Plasma and Urinekassim AliNo ratings yet
- Detection of Etizolam, Flualprazolam, and Flubromazolam by Benzodiazepine-Specific Lateral Flow Immunoassay Test StripsDocument13 pagesDetection of Etizolam, Flualprazolam, and Flubromazolam by Benzodiazepine-Specific Lateral Flow Immunoassay Test Stripsthor888888No ratings yet
- Spectrofluorometric Analysis of New-Generation Antidepressant Drugs in Pharmaceutical Formulations, Human Urine, and Plasma SamplesDocument14 pagesSpectrofluorometric Analysis of New-Generation Antidepressant Drugs in Pharmaceutical Formulations, Human Urine, and Plasma Samplesisma_jrNo ratings yet
- Zhang 2018Document6 pagesZhang 2018ILEANA CASTILLONo ratings yet
- Environmental Immunochemical Analysis Detection of Pesticides and Other Chemicals: A User's GuideFrom EverandEnvironmental Immunochemical Analysis Detection of Pesticides and Other Chemicals: A User's GuideNo ratings yet
- Analytical Methods Used For The Detection andDocument11 pagesAnalytical Methods Used For The Detection andkassim AliNo ratings yet
- Esports - Historical Review Current State and Future ChallengesDocument25 pagesEsports - Historical Review Current State and Future Challengeskassim AliNo ratings yet
- Multidimention Why Need More ResearchDocument14 pagesMultidimention Why Need More Researchkassim AliNo ratings yet
- The Crucifixion of JesusDocument6 pagesThe Crucifixion of Jesuskassim AliNo ratings yet
- The Virtues of Fasting - Fasting Is A Protection From Lusts and Atonement of Sins - Topics On Fasting - Islamic ShariahDocument8 pagesThe Virtues of Fasting - Fasting Is A Protection From Lusts and Atonement of Sins - Topics On Fasting - Islamic Shariahkassim AliNo ratings yet
- Comparison of LC-MS-MS and GC-MS Analysis of Benzodiazepine Compounds Included in The Drug Demand Reduction Analysis ProgramDocument7 pagesComparison of LC-MS-MS and GC-MS Analysis of Benzodiazepine Compounds Included in The Drug Demand Reduction Analysis Programkassim AliNo ratings yet
- Propaganda TechniquesDocument12 pagesPropaganda Techniqueskassim AliNo ratings yet
- PrvaslbchklstDocument4 pagesPrvaslbchklstkassim AliNo ratings yet
- 51 - Absorption of ToxicantsDocument89 pages51 - Absorption of Toxicantskassim AliNo ratings yet
- Safety Services Brochure Single PageDocument12 pagesSafety Services Brochure Single Pagekassim AliNo ratings yet
- Chemical Waste Handling Procedures For Secondary School Science LaboratoriesDocument15 pagesChemical Waste Handling Procedures For Secondary School Science Laboratorieskassim AliNo ratings yet
- Barbosa 2020Document9 pagesBarbosa 2020kassim AliNo ratings yet
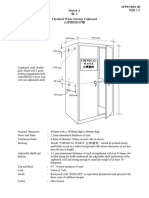
- Chemical Waste Storage CupboardDocument5 pagesChemical Waste Storage Cupboardkassim AliNo ratings yet
- Charges For Technology: A ProposalDocument7 pagesCharges For Technology: A Proposalkassim AliNo ratings yet
- Proposal Form: 2013 Student Technology Fee (STF)Document10 pagesProposal Form: 2013 Student Technology Fee (STF)kassim AliNo ratings yet
- Implementation of QA: 520 Days?Document5 pagesImplementation of QA: 520 Days?kassim AliNo ratings yet
- Content Sheet 4-1: Purchasing and Inventory Overview: Role in Quality Management SystemsDocument11 pagesContent Sheet 4-1: Purchasing and Inventory Overview: Role in Quality Management Systemskassim AliNo ratings yet
- ChromatographyDocument35 pagesChromatographykassim AliNo ratings yet
- CrystalMeth and Index PDFDocument53 pagesCrystalMeth and Index PDFAnthonyHansenNo ratings yet
- Forensic Chem and Toxicology ReviewerDocument40 pagesForensic Chem and Toxicology ReviewerJohn Carl DomingoNo ratings yet
- 03.09.16 News Star WEBDocument16 pages03.09.16 News Star WEBPeter DowellNo ratings yet
- States That Require A Prescription For Dispensing Ephedrine To An Ultimate User, December 2012Document21 pagesStates That Require A Prescription For Dispensing Ephedrine To An Ultimate User, December 2012Joshua HNo ratings yet
- OrganicDocument35 pagesOrganicKristina CoeNo ratings yet
- Anti Allergic DrugsDocument8 pagesAnti Allergic DrugsYojna PatilNo ratings yet
- 00516-CLIA-Newsletter Jan 06Document4 pages00516-CLIA-Newsletter Jan 06losangelesNo ratings yet
- 2ARandomizedControlledVol24No2 3june Sep2006P97Document7 pages2ARandomizedControlledVol24No2 3june Sep2006P97I Made AryanaNo ratings yet
- Kimia AnalisisDocument75 pagesKimia AnalisisQonita NitaNo ratings yet
- Loratadine 5mg + Pseudoephedrine 120mg (Clarinase Repetabs)Document9 pagesLoratadine 5mg + Pseudoephedrine 120mg (Clarinase Repetabs)ddandan_2No ratings yet
- Diary Retail (AutoRecovered)Document56 pagesDiary Retail (AutoRecovered)Maizurah ZulkafliNo ratings yet
- ChloroephedrineDocument9 pagesChloroephedrineTyanNo ratings yet
- Acetaminophen Dextromethorphan Hydrobromide Doxylamine Succinate and Pseudoephedrine Hydrochloride Oral SolutionDocument2 pagesAcetaminophen Dextromethorphan Hydrobromide Doxylamine Succinate and Pseudoephedrine Hydrochloride Oral SolutionMaximiliano OjedaNo ratings yet
- United States v. Goodhue, 486 F.3d 52, 1st Cir. (2007)Document11 pagesUnited States v. Goodhue, 486 F.3d 52, 1st Cir. (2007)Scribd Government DocsNo ratings yet
- Clandestine Laboratory Training Revision 4Document67 pagesClandestine Laboratory Training Revision 4Abbas NjjarkhatirNo ratings yet
- Pseudoephedrine HydrochlorideDocument6 pagesPseudoephedrine HydrochlorideAbdelrhman AboodaNo ratings yet
- History of MethamphetamineDocument3 pagesHistory of Methamphetaminegloria4966No ratings yet
- Daftar Obat PrekusorDocument4 pagesDaftar Obat PrekusormegauningNo ratings yet
- Notice: Registration Revocations, Restrictions, Denials, Reinstatements: Dariah, Gerald E., M.D.Document2 pagesNotice: Registration Revocations, Restrictions, Denials, Reinstatements: Dariah, Gerald E., M.D.Justia.comNo ratings yet
- A Comprehensive Guide To Cooking Meth On Breaking Bad VICE United Kingdom PDFDocument13 pagesA Comprehensive Guide To Cooking Meth On Breaking Bad VICE United Kingdom PDFNguyễn Dũng67% (3)
- A Ferin Plus Pediatric Syrup Chlorpheniramine Maleate Paracetamol Pseudoephedrine Hydrochloride Bilim Ilac Sanayi Ve Ticaret AsDocument9 pagesA Ferin Plus Pediatric Syrup Chlorpheniramine Maleate Paracetamol Pseudoephedrine Hydrochloride Bilim Ilac Sanayi Ve Ticaret Asaschetefera6No ratings yet
- Alexandra Doddridge, Michael Collins and Helen SalourosDocument26 pagesAlexandra Doddridge, Michael Collins and Helen SalourosDoc MartenzNo ratings yet
- Prekursor 16 Mei 23 (Perubahan Kandungan Neozep Forte)Document2 pagesPrekursor 16 Mei 23 (Perubahan Kandungan Neozep Forte)binarobinNo ratings yet
- Backgrounder FDADocument89 pagesBackgrounder FDAWilliams PerdomoNo ratings yet
- CH 7 - Doping in SportsDocument80 pagesCH 7 - Doping in SportsMuhammadAbdulJabarAdnanNo ratings yet