Professional Documents
Culture Documents
Adjuvant Icotinib Versus Observation in Patients W
Uploaded by
Vanilson BorgesOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Adjuvant Icotinib Versus Observation in Patients W
Uploaded by
Vanilson BorgesCopyright:
Available Formats
Articles
Adjuvant icotinib versus observation in patients with
completely resected EGFR-mutated stage IB NSCLC
(GASTO1003, CORIN): a randomised, open-label, phase 2 trial
Wei Ou,a,f Ning Li,b,f Bao-Xiao Wang,c,f Teng-Fei Zhu,a Zhi-Lin Shen,d Tao Wang,e Wu-Guang Chang,a Zeng-Hao Chang,a Xin-Xin Hu,a Yue Pu,e
Lie-Ming Ding,d and Si-Yu Wanga,∗
a
Department of Thoracic Surgery, Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in South China, Collaborative
Innovation Center for Cancer Medicine, Guangzhou, China
b
Department of Breast Oncology, Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in South China, Collaborative
Innovation Center for Cancer Medicine, Guangzhou, China
c
Department of Otolaryngology, Head and Neck Surgery, Sun Yat-sen Memorial Hospital, Sun Yat-sen University, Guangzhou, China
d
Betta Pharmaceuticals Co., Ltd., Hangzhou, China
e
Department of R&D, Hangzhou Repugene Technology Co., Ltd., Hangzhou, China
Summary eClinicalMedicine
2023;57: 101839
Background This phase 2 trial aimed to compare adjuvant icotinib with observation in patients with epidermal growth
factor receptor (EGFR) mutation-positive resected stage IB non-small cell lung cancer (NSCLC). Published Online 3
February 2023
https://doi.org/10.
Methods We performed a randomised, open-label, phase 2 trial from May 1, 2015 to December 29, 2020 at Sun 1016/j.eclinm.2023.
Yat-sen University Cancer Center in China. Patients with completely resected, EGFR-mutant, stage IB (the 7th 101839
edition of TNM staging) NSCLC without adjuvant chemotherapy were randomised (1:1) to receive adjuvant
therapy with icotinib (125 mg, three times daily) for 12 months or to undergo observation until disease
progression or intolerable toxicity occurred. The primary endpoint was 3-year disease-free survival (DFS). CORIN
(GASTO1003) was registered with Clinicaltrials.gov, with the number NCT02264210.
Findings A total of 128 patients were randomised, with 63 patients in the icotinib group and 65 patients in the
observation group. The median duration of follow-up was 39.9 months. The three-year DFS was significantly higher
in the icotinib group (96.1%, 95% confidence interval [CI], 91.3–99.9) than in the observation group (84.0%, 95% CI,
75.1–92.9; P = 0.041). The DFS was significantly longer in the icotinib group than in the observation group, with a
hazard ratio (HR) of 0.23 (95% CI, 0.07–0.81; P = 0.013). The OS data were immature, with three deaths in the
observation arm. In the icotinib group, adverse events (AEs) of any grade were reported in 49 patients (77.8%),
and grade 3 or greater AEs occurred in four patients (6.3%). No treatment-related deaths occurred.
Interpretation Our findings suggested that adjuvant icotinib improved the 3-year DFS in patients with completely
resected EGFR-mutated stage IB NSCLC with a manageable safety profile.
Funding This study was sponsored by Betta Pharmaceutical Co., Ltd.
Copyright © 2023 The Author(s). Published by Elsevier Ltd. This is an open access article under the CC BY-NC-ND
license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Keywords: Icotinib; Adjuvant therapy; Stage IB NSCLC
Introduction 80% of all lung cancer cases.2 Only 30% of patients
Lung cancer is the leading cause of cancer mortality with NSCLC are suitable for surgery, which is consid-
worldwide, with an estimated 12.8 million deaths per ered the most effective treatment option.3,4 The absolute
year, accounting for approximately 1 in 5 cancer deaths.1 survival improvement at 5 years following adjuvant
Non-small cell lung cancer (NSCLC) is the most com- cisplatin-based chemotherapy in patients with early-
mon pathological type and accounts for approximately stage NSCLC is 5.4%.5 Although platinum-based
*Corresponding author. Department of Thoracic Surgery, Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in South China,
Collaborative Innovation Center for Cancer Medicine, 651 Dongfeng Road East, Guangzhou 510060, China.
E-mail address: wangsy@sysucc.org.cn (S.-Y. Wang).
f
Contributed equally to this work.
www.thelancet.com Vol 57 March, 2023 1
Articles
Research in context
Evidence before this study staging) NSCLC who had not received adjuvant
Increasing evidence suggests that adjuvant epidermal growth chemotherapy or perioperative radiation therapy. Our
factor receptor tyrosine kinase inhibitors (EGFR-TKIs) may be study does provide important evidence that an EGFR-TKI,
effective in a selected population after resection of early-stage in the adjuvant setting, has anti-tumour efficacy and is
non-small cell lung cancer (NSCLC). However, prospective generally well tolerated in patients with completely
clinical trials of these regimens have largely excluded patients resected stage IB NSCLC.
with stage IB disease. Despite of efficacy among patients with
Implications of all the available evidence
stage IB in the ADAURA study, rare trial was designed
The results of the phase II trial suggest that adjuvant icotinib
specifically for stage IB EGFR-mutant NSCLC. We searched
is a well-tolerated regimen for patients with completely
PubMed using the terms “stage IB” and “EGFR-TKI” and
resected stage IB (the 7th edition of TNM staging) NSCLC,
“adjuvant” up to September 30, 2022, and we identified only
with longer disease-free survival (DFS) in the icotinib group
a small number of clinical trials reporting the efficacy and
than in the observation group. These findings address an
safety of adjuvant EGFR-TKI therapies for treatment of stage
important knowledge gap for the treatment of completely
IB NSCLC.
resected stage IB NSCLC and also suggest that adjuvant EGFR-
Added value of this study TKIs are a valuable therapeutic strategy. Given the limited
To the best of our knowledge, this phase II trial is the first studies on the role of adjuvant EGFR-TKIs in stage IB NSCLC,
prospective, randomised study to evaluate the efficacy and our results could directly improve clinical practise and broaden
safety of adjuvant icotinib in a patient population with treatment options for patients with completely resected stage
completely resected stage IB (the 7th edition of TNM IB NSCLC.
chemotherapy following surgery improves survival in Icotinib is a first-generation EGFR-TKI that shows
patients with stage II-IIIA NSCLC and in selected pa- similar efficacy but a good safety profile when compared
tients with IB disease, the survival outcomes are not with gefitinib in pretreated patients with advanced
satisfactory.6 The 5-year survival rate following surgery NSCLC in the ICOGEN trial.23 In the CONVINCE trial,
and adjuvant chemotherapy ranges from 67% for stage first-line icotinib significantly prolonged progression-
IB disease to 39% for stage IIIA disease, and disease free survival (PFS) and had a good tolerability profile
recurrence remains high across all disease stages.7 Lung in advanced EGFR-mutated lung adenocarcinoma
cancer screening has proven to reduce mortality by compared with chemotherapy.24 The recent EVIDENCE
20–30%, and more than a half of screening-detected trial demonstrated that icotinib improves DFS and is
lung cancers were stage I disease.8,9 The increasing associated with a more favourable safety profile in pa-
use of screening will lead to a substantial shift to early- tients with resected EGFR-mutant stage II-IIIA
stage (including stage IB) NSCLC, making adjuvant NSCLC.18 Based on the results from EVIDENCE, first-
treatment for stage IB disease a major challenge. generation icotinib was approved in China for resected
An epidermal growth factor receptor (EGFR) shows a EGFR-mutant stage II-IIIA NSCLC in the adjuvant
very high prevalence in patients from eastern Asia (40%– setting. However, no study has been designed specif-
60%) compared with patients from Western countries ically for stage IB NSCLC with EGFR mutations. This
(10%–15%).10 EGFR tyrosine kinase inhibitors (TKIs) have phase II study was designed to assess whether adjuvant
been established for advanced EGFR-mutant NSCLC.11 therapy with first-generation icotinib can improve sur-
Many efforts have been made to explore the role of vival outcomes compared with observation in patients
EGFR-TKIs as an adjuvant treatment for EGFR-mutant with resected EGFR-mutant stage IB (the 7th edition of
NSCLC.12–19 A prior meta-analysis showed that EGFR- TNM staging) NSCLC without adjuvant chemotherapy.
TKIs can significantly improve disease-free survival
(DFS) and that TKIs are associated with fewer adverse
events (AEs) in patients with resected EGFR-mutant Methods
NSCLC than chemotherapy in the adjuvant setting.20 In Study design and participants
the ADAURA trial, 3-year osimertinib in patients with CORIN (GASTO1003) was a randomised, open-label,
resected EGFR-mutated stage IB-IIIA (the 7th edition of phase 2 trial conducted at Sun Yat-sen University Can-
TNM staging) disease improved DFS compared with cer Center in China. Eligible patients were ≥18 years
placebos, with a hazard ratio (HR) of 0.20.21 Based on the old; had an Eastern Cooperative Oncology Group per-
results of the ADAURA study, the third-generation TKI formance status (ECOG PS) score of 0 or 1; had
osimertinib was approved by the FDA for NSCLC patients completely resected (R0) stage IB disease (according to
with sensitising EGFR mutations (exon 19 deletion or the 7th edition of the AJCC TNM staging system for
exon 21 L858R) in the adjuvant setting.6,22 lung cancer25); and had a confirmed EGFR mutation
2 www.thelancet.com Vol 57 March, 2023
Articles
(exon 19 deletion, exon 21 L858R, or uncommon EGFR administration of icotinib. Eligible patients received
mutations including exon 18 G719X, exon 20 S768I, and either 1 year of icotinib (125 mg thrice daily adminis-
exon 21 L861Q). Additional eligibility criteria were a life tered orally) or none. The start of treatment needed to be
expectancy of at least 1 year, adequate haematological within 4 weeks after surgical resection. The therapy
function (absolute neutrophil count ≥2.0 × 109/L, continued until disease progression or intolerable toxic
platelet count ≥100 × 109/L, and haemoglobin ≥9 g/dL), effects occurred.
adequate liver function (serum total bilirubin ≤1.5 times Follow-up assessments were scheduled at month 3
the upper limit of normal; aspartate aminotransferase and month 6 after surgery, every 6 months until 5 years,
and alanine aminotransferase ≤2.5 times the upper and every 12 months thereafter. The follow-up assess-
limit of normal), and adequate renal function (serum ments involved a physical examination and contrast-
creatinine clearance ≥60 mL/min). enhanced CT of the chest. Brain MRI was scheduled
Key exclusion criteria included a second primary every 12 months. Bone scans and other examinations
malignancy within 5 years (except for cured basal cell were performed based on symptoms. Disease recur-
carcinoma of the skin or cured in situ carcinoma of the rence was evaluated at follow-up visits and was deter-
uterine cervix); prior treatment with antitumor agents or mined according to the Response Evaluation Criteria in
radiotherapy; a history of severe drug hypersensitivity; a Solid Tumours (RECIST) version 1.1 by the in-
history of interstitial pneumonitis; a history of myocar- vestigators. At disease relapse, the dates and sites of
dial infarction or angina within the past 6 months; any recurrence were recorded. Post-recurrence therapy was
unstable systemic disease (such as unstable heart dis- permitted.
ease or uncontrolled hypertension); an active uncon- Safety and tolerability were evaluated at every visit for
trolled infection; and pregnancy or lactation. We the icotinib group. All AEs were classified according to
excluded patients who had been treated with neo- the National Cancer Institute’s Common Terminology
adjuvant chemotherapy, adjuvant chemotherapy, or Criteria for Adverse Events (NCI-CTCAE) version 4.0.
perioperative radiation therapy. The decisions for not AEs were managed according to the AE management
receiving adjuvant chemotherapy were made according protocol.
to physician and patient choices.
The study was approved by the medical ethical Outcomes
committee of the Guangdong Association of Study of The primary endpoint was 3-year DFS, which was
Thoracic Oncology (GASTO) and the Medical Ethics defined as the proportion of patients who were disease
Committee of Sun Yat-sen University Cancer Center. free at 3 years. The secondary endpoints included DFS
The trial protocol and statistical analysis plan are avail- (time from random assignment to documented disease
able in the supplementary material. This trial was con- recurrence or death, whichever occurred first), central
ducted in accordance with the Declaration of Helsinki nervous system (CNS)-related DFS (time from ran-
and Good Clinical Practise guidelines and the policy of domisation to CNS recurrence or death, whichever
the trial sponsor, Betta Pharmaceuticals. This article was occurred first), overall survival (OS, time from random
prepared in accordance with CONSORT guidelines assignment to death from any cause), safety and
(Supplementary Table S1). All patients provided written tolerability.
informed consent. CORIN (GASTO1003) was registered
with Clinicaltrials.gov, with the number NCT02264210. Statistical analysis
On the basis of the CALGB 9633 trial, we projected a 3-
Randomisation and masking year DFS of 60% for patients with stage IB NSCLC. The
Randomisation was performed by the study staff of the study was designed to determine whether adjuvant
GASTO through a computer-generated sequence with a icotinib would result in a 17% absolute improvement
minimisation method that balanced sex (male vs. fe- (from 60% to 77%) in 3-year DFS, with 80% power at a
male) and ECOG PS (0 vs. 1) for random assignment. two-sided α of 0.1. This improvement corresponded to
Eligible patients were randomly assigned in a 1:1 ratio to an hazard ratio (HR) of 0.5. Assuming an accrual time
either receive oral icotinib or undergo observation. All of 2 years, a follow-up time of 3 years, and an anticipated
investigators, study personnel, and patients were not dropout rate of 5%, a total of 128 patients would be
masked to patient distribution. required to be randomly assigned.
The point estimates of 3-year DFS were calculated by
Procedures the Kaplan–Meier method, and the difference in 3-year
Baseline assessments before study entry included a full DFS between groups was compared by the Z test. The
history and a physical examination, enhanced computed median DFS and OS were estimated by the Kaplan–
tomography (CT) scans of the chest and the upper Meier method and compared by the log-rank test. Cox
abdomen, brain magnetic resonance imaging (MRI), proportional hazards models were used to estimate HRs
and haematologic and biochemical testing. The baseline with their 95% confidence intervals (CIs). Predefined
assessments were performed within 4 weeks before the subgroup comparisons of DFS were performed for sex
www.thelancet.com Vol 57 March, 2023 3
Articles
(male vs. female) and EGFR mutation (exon 19 deletion patients in the icotinib group and 13 patients in the
vs. exon 21 L858R). Subgroup analyses of age (≥65 vs. observation group had had disease recurrence. The
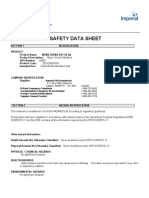
<65), smoking history (ever vs. never) and side (left vs. percentage of patients who were alive and disease-free at
right) were done in a post hoc manner. All analyses for 3 years was significantly higher in the icotinib group
efficacy were based on intention-to-treat (ITT) popula- (96.1%, 95% CI, 91.3–99.9) than in the observation
tion. Safety analysis included all patients in the icotinib group (84.0%, 95% CI, 75.1–92.9; P = 0.041; Fig. 2A).
group who received at least one dose of the study The DFS in the full analysis set was significantly longer
medication and had one or more safety follow-up visits. for those assigned icotinib than for those assigned
Patient characteristics and treatment-related AEs were observation (HR 0.23; 95% CI, 0.07–0.81; P = 0.013;
analysed descriptively. The data cutoff date was July 30, Fig. 2A). This HR equalled a 77% reduction in the risk
2022. All P values reported herein are two-sided, and P of disease recurrence or death. The HR adjusted for sex
values less than 0.05 are considered to be significant. and ECOG PS was 0.23 (95% CI, 0.06–0.79; adjusted P
value, 0.020). Although the median DFS had not been
Role of the funding source reached in either group, the Kaplan–Meier curves
The study sponsor (Betta Pharmaceuticals) was involved showed early separation between the icotinib and
in the study design, data collection, analysis, interpre- observation groups and maintained this separation
tation, and the writing of this report. All authors had full throughout the trial.
access to all the data in the study and had final re- To rule out the possible influence of different edi-
sponsibility for the decision to submit the manuscript tions of staging, we restaged all patients according to the
for publication. 8th edition of the TNM classification and performed an
exploratory analysis of DFS based on the AJCC edition
of staging. Since we only enrolled patients without
Results adjuvant chemotherapy, 123 patients remained in stage
Patients and treatment IB, and only 5 patients were reclassified as stage IIA
From May 1, 2015 through December 29, 2020, 485 (T2bN0) according to the 8th edition of the TNM staging
patients were screened, and 357 patients were excluded system. Similar results were observed in patients with
due to the following reasons: EGFR wild-type status stage IB disease by the 8th edition of TNM staging
(n = 249), adjuvant chemotherapy (n = 99), withdrawal (Fig. 2B). The 3-year DFS rates were 95.9% (95% CI,
of consent before randomisation (n = 3), unstable sys- 90.9–99.9) in the icotinib group and 83.0% (95% CI,
temic disease (n = 2), double cancer within 5 years 73.7–92.4) in the observation group, and the results
(n = 2), bone metastases before randomisation (n = 1), favoured the icotinib group (P = 0.041). The icotinib
and stage other than stage IB (n = 1). Finally, 128 group also had a significantly lengthened DFS time
eligible patients with completely resected, EGFR-mutant compared with the observation group (HR, 0.25; 95%
stage IB NSCLC without adjuvant chemotherapy were CI, 0.07–0.87; P = 0.018; Fig. 2B). This HR equalled a
enrolled and randomised to receive icotinib (n = 63) or 75% reduction in the risk of disease recurrence or death.
undergo observation (n = 65). All 128 patients were To rule out the possible influence of atypical EGFR
included in the full analysis set (Fig. 1). Baseline char- mutations, we reanalysed the DFS results by excluding 3
acteristics were balanced between the two groups patients with the exon 18 G719X mutation. As we ex-
(Table 1). Overall, 58%–59% of the patients were female. pected, the DFS was also significantly different between
Almost all surgical types were lobectomies in both arms. the two groups (P = 0.005; Supplementary Fig. S1).
Patients with exon 21 L858R accounted for 46% and Subgroup analyses of DFS with respect to baseline
52% of patients in the icotinib arm and in the obser- characteristics are shown in Fig. 3. The DFS favoured
vation arm, respectively. Of note, 3 patients with the icotinib in patients who had right-sided disease
uncommon EGFR mutation exon 18 G719X were also (P = 0.022). There were no significant differences be-
included in the full analysis set. tween icotinib and observation in other factors, although
Regarding treatment compliance, 46 patients (73.0%) the DFS had a trend toward favouring icotinib in pa-
in the icotinib group completed the planned 1-year tients who were nonsmokers (HR, 0.31; 95% CI,
treatment, and none of the patients in the icotinib 0.08–1.14; P = 0.077). These results may be due to the
group were still receiving the study medication at the small sample size and the short follow-up time.
data cutoff. A total of 17 patients discontinued icotinib CNS-related recurrence occurred in 0 of 63 patients
treatment because of patient decisions (n = 15) and AEs in the icotinib group and in 6 of 65 patients (9.2%) in
(n = 2). For patients who received icotinib, the median the observation group. The 3-year CNS-related DFS was
duration of treatment was 12.0 months (range 0.5–14.6). significantly higher in the icotinib group (100%) than in
the observation group (93.8%; Fig. 4A). The CNS-related
Efficacy DFS was significantly longer for those who received
The median follow-up in the full analysis set was 39.9 icotinib than for those who underwent observation
(IQR 25.7–59.4) months. By the data cutoff, three (P = 0.018; Fig. 4A), although the median CNS-related
4 www.thelancet.com Vol 57 March, 2023
Articles
Fig. 1: Study profile. Data cutoff on July 30, 2022. N, number; EGFR, epidermal growth factor receptor.
DFS was not reached in either group. Similar results grade were reported in 49 (77.8%) of 63 patients who
were observed in patients with stage IB disease by the had received icotinib (Table 2). The most common AEs
8th edition of TNM staging. The icotinib group also had reported were rash (25, 39.7%), diarrhoea (13, 20.6%),
a significantly lengthened CNS-related DFS compared and pain (7, 11.1%). No cases of drug-induced intersti-
with the observation group (P = 0.030; Fig. 4B). tial lung disease were recorded.
Subsequent treatments after recurrence were Grade 3 or greater AEs occurred in 4 patients (6.3%)
administered in 3 of 3 (100%) and in 12 of 13 (92.3%) in the icotinib group, including rash in 2 patients
patients in the icotinib and observation groups, respec- (3.2%), diarrhoea in 1 patient (1.6%), and pain in 1 pa-
tively. Eleven of 13 patients who had relapsed in the tient (1.6%). Dose discontinuation of icotinib owing to
observation group received EGFR-TKI treatment. All 3 AEs occurred in 2 patients (3.2%). None of the patients
patients who had had recurrence in the icotinib group had dose reductions.
received EGFR-TKI treatment.
A total of 3 death events had occurred by the data
Discussion
cutoff (icotinib, n = 0; observation, n = 3). The OS data
This phase 2, open-label, randomised CORIN
are not mature. Although the preliminary analysis
(GASTO1003) trial examined the efficacy and safety of
revealed that the Kaplan–Meier curves showed separa-
adjuvant icotinib in patients with completely resected,
tion regardless of whether the 7th or 8th edition staging
EGFR-mutant, stage IB NSCLC without adjuvant
system was used, the OS was not significantly different
chemotherapy. Although the median DFS was not
between the two groups (P = 0.098 and P = 0.095;
reached in either group at the data cutoff, the overall
Supplementary Fig. S2).
results demonstrated a positive effect of icotinib. The
primary endpoint of CORIN, 3-year DFS, was signifi-
Safety cantly improved among patients who had been assigned
All 63 patients in the icotinib group were included in the to receive icotinib (3-year DFS, 96.1% vs. 84.0%).
safety analysis set. Icotinib was well tolerated with no The CALGB 9633 trial explored the role of chemo-
unexpected AEs, and there were no deaths that were therapy in stage IB (6th edition of TNM staging)
deemed to be treatment-related. Overall, AEs of any NSCLC.26 Of note, the 6th edition of staging included
www.thelancet.com Vol 57 March, 2023 5
Articles
Icotinib (n = 63) Observation (n = 65)
Age, years 56 (35–75) 57 (32–75)
Sex
Male 26 (41.3) 27 (41.5)
Female 37 (58.7) 38 (58.5)
ECOG PS
0 63 (100.0) 64 (98.5)
1 0 1 (1.5)
Smoking status
Never 48 (76.2) 46 (70.8)
Former 1 (1.6) 3 (4.6)
Current 14 (22.2) 16 (24.6)
Histology
Adenocarcinoma 62 (98.4) 65 (100.0)
Adenosquamous carcinoma 1 (1.6) 0
Differentiation
High/Moderate 48 (76.2) 50 (76.9)
Low 14 (22.2) 13 (20.0)
Unknown 1 (1.6) 2 (3.1)
Surgery type
Lobectomy 63 (100.0) 64 (98.5)
Other 0 1 (1.5)
Side
Left 26 (41.3) 25 (38.5)
Right 37 (58.7) 40 (61.5)
EGFR mutation
Exon 19 deletion 32 (50.8) 30 (46.2)
Exon 21 L858R 29 (46.0) 34 (52.3)
Exon 18 G719X 2 (3.2) 1 (1.5)
Data are n (%) or median (range). ECOG PS, Eastern Cooperative Oncology Group performance status; EGFR, epidermal growth factor receptor.
Table 1: Demographic and clinical characteristics of patients (n = 128).
lymph node–negative and invasion-negative (other than completely resected stage II–IIIA (N1–N2) EGFR-
visceral pleura) tumours that were >3 cm in the greatest mutant NSCLC, but the DFS benefit did not translate
dimension.27 Although a significant survival advantage into a significant OS difference.16,29 The EVAN trial
was not observed in the entire population in CALGB showed that adjuvant erlotinib improved the 2-year DFS
9633, chemotherapy demonstrated superiority in regard compared with chemotherapy in resected stage IIIA
to OS in patients with tumours ≥4 cm.26 The tumour EGFR-mutant NSCLC.17 However, the IMPACT trial
size threshold was further verified in JBR-10, in which comparing gefitinib and vinorelbine plus cisplatin for
OS favoured patients with tumours ≥4 cm, whereas no patients with resected stage II-IIIA EGFR mutation-
benefit was observed in patients with tumours <4 cm. positive NSCLC failed to meet its DFS endpoint.19 Ico-
To utilise the above results in the 8th edition of the tinib showed its superiority in DFS for patients with
TNM staging system.28 adjuvant chemotherapy is rec- completely resected stage II-IIIA NSCLC with EGFR
ommended for patients with stage IIA (T2bN0) or mutations.18 There are other studies that compared
greater NSCLC. In our study, patients were enrolled EGFR-TKIs with placebos or observation after chemo-
based on the 7th edition of the TNM staging system. therapy, including the BR.19 study,12 the RADIANT
Since we only enrolled patients without adjuvant study,14 Li’s study,13 and the ADAURA study.21
chemotherapy, 123 (96.1%) patients remained in stage In the ADAURA trial, patients with completely
IB according to the 8th edition of the TNM staging resected EGFR-mutant stage IB-IIIA (7th edition of
system. TNM staging) NSCLC were randomly assigned to
There have been a few efforts to compare EGFR-TKIs receive either 3-generation osimertinib or placebos for 3
as adjuvant therapy with chemotherapy in early-stage years. The primary endpoint was DFS among patients
NSCLC. The ADJUVANT trial demonstrated that gefi- with stage II-IIIA disease. Postoperative adjuvant
tinib improved DFS compared with chemotherapy for chemotherapy before randomisation was allowed but
6 www.thelancet.com Vol 57 March, 2023
Articles
A 100 | | ||| | ||| | || | ||
| | || |||| | || | | ||| | | || ||
| || ||| || | | | || | | | | | | | | | || |
|
||
| | | || || |
Disease-free survival (%)
80 | | ||| | |
|
| || |
60
Icotinib group
Observation group
3-year DFS
40
Icotinib group 96.1%
Observation group 84.0%
20
HR, 0.23 (95% CI, 0.07-0.81); p = 0.013
0
0 12 24 36 48 60
Months since randomization
Number at risk
icotinib 63 62 49 33 19 12
observation 65 59 48 32 21 13
B 100 | ||
|| | ||| | || | ||
| | || | || | || | | ||| | | || ||
| || ||| || | | | || | | | | | | | | | ||
| ||
||
Disease-free survival (%)
| ||| || |
80 | | ||| | |
| ||
||
60 Icotinib group
Observation group
40 3-year DFS
Icotinib group 95.9%
Observation group 83.0%
20
HR, 0.25 (95% CI, 0.07-0.87); p = 0.018
0
0 12 24 36 48 60
Months since randomization
Number at risk
icotinib 61 60 47 32 18 11
observation 62 56 45 29 19 13
Fig. 2: Kaplan–Meier curves for disease-free survival in the overall population based on (A) 7th edition of TNM staging system and (B)
8th edition of TNM staging system. DMS, disease-free survival; HR, hazard ratio; CI, confidence interval.
not mandatory. In the stage IB-IIIA population, osi- NSCLC in the adjuvant setting. In exploratory analyses,
mertinib was associated with an 80% reduction in the the DFS in the stage IB population was similarly
risk of disease relapse or death, and the 1-year DFS rates improved for patients who had received osimertinib,
were 89% in the osimertinib group and 52% in the with an HR of 0.39 (95% CI, 0.18–0.76). An exploratory
placebo group.21 Based on the results from ADAURA, analysis of DFS based on the AJCC 8th edition TNM
osimertinib became the first approved targeted drug for staging system also favoured osimertinib in the stage IB
www.thelancet.com Vol 57 March, 2023 7
Articles
Variables Subgroup N (%) DFS HR (95% CI) P value
Overall 128 (100) 0.23 (0.07-0.81) 0.022
Age ≥ 65 40 (31.3) 0.02 (0.01-19.77) 0.272
<65 88 (68.8) 0.36 (0.09-1.38) 0.136
Gender Male 53 (41.4) 0.02 (0.01-11.71) 0.220
Female 75 (58.6) 0.44 (0.11-1.71) 0.237
Smoking history Yes 34 (26.6) 0.02 (0.01-70.60) 0.347
No 94 (73.4) 0.31 (0.08-1.14) 0.077
Side Left 51 (39.8) 0.99 (0.14-7.06) 0.993
Right 77 (60.2) 0.09 (0.02-0.71) 0.022
EGFR mutation Exon 19 del 62 (48.4) 0.53 (0.10-2.90) 0.465
Exon 21 L858R 63 (49.2) 0.02 (0.01-3.41) 0.131
0.01 0.1 1 10 100
Favours icotinib Favours observation
Fig. 3: Subgroup analyses of disease-free survival with respect to baseline characteristics. N, number; DFS, disease-free survival; HR, hazard
ratio; CI, confidence interval; EGFR, epidermal growth factor receptor.
population, with an HR of 0.38 (0.17–0.84).22 Of note, lead to emerging patterns of acquired resistance.32 In the
adjuvant chemotherapy was administered to approxi- EVIDENCE trial, patients in the TKI arm were planned
mately one-quarter (26%) of patients with stage IB dis- to receive first-generation icotinib for 2 years, and the
ease. Unlike the ADAURA study, CORIN is a trial median treatment duration was 22.2 months.18 In our
designed specifically for stage IB EGFR-mutant NSCLC. study, the treatment duration of icotinib was set as 1
To preclude confoundment by adjuvant chemotherapy, year. AEs were more frequent in ADAURA and EVI-
we only enrolled patients who had not received adjuvant DENCE; grade ≥3 AEs were observed in 20% of patients
chemotherapy according to physician and patient in the osimertinib arm in ADAURA, 11% of patients in
choices. In our study, icotinib was associated with a the icotinib arm in EVIDENCE, and 6.3% of patients in
75%–77% reduction in the risk of disease relapse or the icotinib arm in our study. The type and grade of AEs
death, with an HR of 0.23 (95% CI, 0.07–0.81) for the recorded in our study are consistent with the known
7th edition of TNM staging and an HR of 0.25 (95% CI, safety profiles of icotinib.23 Notably, interstitial lung
0.07–0.87) for the 8th edition of TNM staging. disease occurred in 3% of patients in ADAURA,
Compared with the results of stage IB disease from the whereas no interstitial lung disease was recorded in
ADAURA trial, a great treatment effect on DFS was EVIDENCE or our study. It seems that a shorter treat-
observed in our study. One important possible reason is ment duration is associated with fewer toxicities. The
that 96% patients were restaged as IB stage (8th edition therapy duration and the selection of appropriate EGFR-
of staging) in CORIN, whereas only about 50% were TKIs should balance the anticipated treatment benefit
restaged as IB stage in ADAURA. Direct comparisons of and harm. Circulating tumour DNA (ctDNA) has shown
different EGFR-TKIs in the adjuvant setting of NSCLC potential value in guiding early individualised cancer
are needed. The OS data of CORIN are not mature and interventions for early-stage NSCLC.33,34 Longitudinal
the OS was not significantly different between the two ctDNA positive was associated with inferior DFS for
groups now. Actually, DFS benefit also did not translate resected stage IA-IIIA EGFR-mutant NSCLC.35 The
into a significant difference in OS in ADJUVANT, optimal treatment duration and medicine choice of
ADAURA, and EVIDENCE, supporting DFS being a adjuvant EGFR-TKIs and the role of ctDNA in adjuvant
surrogate for OS in the adjuvant setting of NSCLC. The EGFR-TKIs treatment remain to be determined.
OS improvement of adjuvant EGFR-TKIs was only re- Caution should be taken when interpreting our re-
ported in the EVAN trial.30 sults in view of the fact that this is an open-label and
In ADAURA, the treatment duration of osimertinib single-centre phase 2 study focusing on stage IB NSCLC
was set to be 3 years, and the median treatment duration patients without chemotherapy. The main limitations of
was 22.5 months.21 However, some patients in this study include the relatively small sample size and
ADAURA seem to have been overtreated for years at a the immature OS data. The follow-up will continue, and
high cost to society and have suffered from AEs.31 Using the survival results might be updated. Furthermore,
third-generation osimertinib in the adjuvant setting may patients with uncommon EGFR mutations were allowed
8 www.thelancet.com Vol 57 March, 2023
Articles
A
100 | | | || | ||||
||| ||
| |||| | || || ||| || | | | | | | || |||| | || | | | | | | | || || |
||
| | | | | | ||
|| | | || || | | | | ||| | ||
CNS Disease-free survival (%)
||
80 | ||
60 Icotinib group
Observation group
40
20
p = 0.018
0
0 12 24 36 48 60
Months since randomization
Number at risk
icotinib 63 62 50 35 21 14
observation 65 64 52 35 25 14
B
100 | | | || | ||||
||| ||||||| | || || ||| || | | | | | | || | || | || | | | | | | | || || |
||
| | | | | | ||
|| | | | || | | | | ||| | || |
CNS Disease-free survival (%)
| ||
80
60 Icotinib group
Observation group
40
20
p = 0.03
0
0 12 24 36 48 60
Months since randomization
Number at risk
icotinib 61 60 48 34 20 13
observation 62 61 49 32 23 14
Fig. 4: Kaplan–Meier curves for central nervous system (CNS) disease-free survival in the overall population based on (A) 7th edition of
TNM staging system and (B) 8th edition of TNM staging system.
in this study, although an exploratory analysis of DFS in adjuvant setting, we only included Chinese patients in
patients with sensitive EGFR mutations confirmed the this study, which may not be generalisable in other
superiority of icotinib. Because icotinib was only populations. However, these limitations do not seem to
approved in China for resected EGFR-mutant stage have distorted our findings. Despite these limitations,
II-IIIA non-small cell lung cancer (NSCLC) in the our data still support important evidence on adjuvant
www.thelancet.com Vol 57 March, 2023 9
Articles
(www.researchdata.org.cn), with the approval RDD number as
AEs RDDA2022873224. The datasets used and/or analysed during the cur-
Any grade Grade 1-2 Grade ≥3 rent study are available from the corresponding author on a reasonable
request.
Totala 49 (77.8%) 45 (71.4%) 4 (6.3%)
Rash 25 (39.7%) 24 (38.1%) 2 (3.2%) Declaration of interests
Diarrhoea 13 (20.6%) 12 (19.0%) 1 (1.6%) LMD and ZLS are employees of Betta Pharmaceuticals Co., Ltd. TW and
Pain 7 (11.1%) 7 (11.1%) 1 (1.6%) YP are employees of Hangzhou Repugene Technology Co., Ltd. Other
Elevated ALT 6 (9.5%) 6 (9.5%) 0 co-authors declare no competing interests.
Decreased appetite 5 (7.9%) 5 (7.9%) 0
Acknowledgements
Insomnia 4 (6.3%) 4 (6.3%) 0
This study was sponsored by Betta Pharmaceutical Co., Ltd. We express
Fatigue 4 (6.3%) 4 (6.3%) 0 gratitude to the patients and their families. We also thank all the trial site
Nausea 3 (4.8%) 3 (4.8%) 0 coordinators. This work was supported by the Science and Technology
Leukopenia 3 (4.8%) 3 (4.8%) 0 Project of Guangzhou City (202102021063).
Oral ulcers 3 (4.8%) 3 (4.8%) 0
Appendix A. Supplementary data
AST increased 3 (4.8%) 3 (4.8%) 0
Supplementary data related to this article can be found at https://doi.
Vomiting 2 (3.2%) 2 (3.2%) 0
org/10.1016/j.eclinm.2023.101839.
Cough 2 (3.2%) 2 (3.2%) 0
Pruritus 2 (3.2%) 2 (3.2%) 0
Dizziness 2 (3.2%) 2 (3.2%) 0 References
Anaemia 1 (1.6%) 1 (1.6%) 0 1 Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020:
Constipation 1 (1.6%) 1 (1.6%) 0 GLOBOCAN estimates of incidence and mortality worldwide for 36
cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249.
Data are n (%). All AEs were assessed according to the National Cancer Institute 2 Howlader N, Forjaz G, Mooradian MJ, et al. The effect of advances
Common Terminology Criteria for Adverse Events, version 4.0). AEs, adverse in lung-cancer treatment on population mortality. N Engl J Med.
events; ALT, alanine aminotransferase; AST, aspartate transaminase. aTotal 2020;383(7):640–649.
patients who had at least one AE; some patients had more than one AE. 3 Datta D, Lahiri B. Preoperative evaluation of patients undergoing
lung resection surgery. Chest. 2003;123(6):2096–2103.
Table 2: Adverse events in the icotinib group (n = 63). 4 Le Chevalier T. Adjuvant chemotherapy for resectable non-small-cell
lung cancer: where is it going? Ann Oncol. 2010;21(Suppl 7):
vii196–v198.
5 Pignon JP, Tribodet H, Scagliotti GV, et al. Lung adjuvant cisplatin
evaluation: a pooled analysis by the LACE Collaborative Group.
EGFR-TKIs for patients with resected stage IB NSCLC J Clin Oncol. 2008;26(21):3552–3559.
with EGFR mutations. The ADAURA2 trial 6 Pisters K, Kris MG, Gaspar LE, Ismaila N. Adjuvant systemic T,
(NCT05120349) comparing 3-year osimertinib and adjuvant radiation therapy for stage ItINGEP. Adjuvant systemic
therapy and adjuvant radiation therapy for stage I-IIIA completely
observation in stage IA2-IA3 EGFR-mutant NSCLC is resected non-small-cell lung cancer: ASCO guideline rapid recom-
currently recruiting patients. The ICTAN (GASTO1002) mendation update. J Clin Oncol. 2022;40(10):1127–1129.
7 Kris MG, Gaspar LE, Chaft JE, et al. Adjuvant systemic therapy and
trial (NCT01996098) comparing chemotherapy followed adjuvant radiation therapy for stage I to IIIA completely resected
by 6-month or 12-month icotinib with chemotherapy as non-small-cell lung cancers: American society of clinical oncology/
adjuvant therapy in stage IIA-IIIA NSCLC harbouring cancer care ontario clinical practice guideline update. J Clin Oncol.
2017;35(25):2960–2974.
EGFR mutations is underway to further investigate the 8 National Lung Screening Trial Research T, Aberle DR, Adams AM,
role of icotinib in the adjuvant setting for NSCLC. et al. Reduced lung-cancer mortality with low-dose computed
In conclusion, to our knowledge, CORIN is the first tomographic screening. N Engl J Med. 2011;365(5):395–409.
9 de Koning HJ, van der Aalst CM, de Jong PA, et al. Reduced lung-
prospective study to demonstrate that adjuvant icotinib cancer mortality with volume CT screening in a randomized trial.
improves 3-year DFS compared with observation for N Engl J Med. 2020;382(6):503–513.
10 Tan DS, Mok TS, Rebbeck TR. Cancer genomics: diversity and
patients with stage IB EGFR-mutant NSCLC after disparity across ethnicity and geography. J Clin Oncol.
complete resection, with acceptable safety and tolera- 2016;34(1):91–101.
bility. Thus, icotinib provides a treatment option for 11 Tan AC, Tan DSW. Targeted therapies for lung cancer patients with
oncogenic driver molecular alterations. J Clin Oncol.
such patients. Further studies to elucidate individu- 2022;40(6):611–625.
alised strategies for adjuvant EGFR-TKI therapy in pa- 12 Goss GD, O’Callaghan C, Lorimer I, et al. Gefitinib versus placebo
tients with early-stage NSCLC are warranted. in completely resected non-small-cell lung cancer: results of the
NCIC CTG BR19 study. J Clin Oncol. 2013;31(27):3320–3326.
13 Li N, Ou W, Ye X, et al. Pemetrexed-carboplatin adjuvant chemo-
Contributors therapy with or without gefitinib in resected stage IIIA-N2 non-
SYW and LMD designed the research. WO, NL, BXW, TFZ, WGC, small cell lung cancer harbouring EGFR mutations: a randomized,
ZHC, XXH and SYW performed the research and collected data. All phase II study. Ann Surg Oncol. 2014;21(6):2091–2096.
authors analysed and interpreted the data. WO, NL and SYW have 14 Kelly K, Altorki NK, Eberhardt WE, et al. Adjuvant erlotinib versus
verified the underlying data. WO, NL, and BXW draughted the manu- placebo in patients with stage IB-IIIA non-small-cell lung cancer
script. All authors had full access to all the data in the study and had (RADIANT): a randomized, double-blind, phase III trial. J Clin
final responsibility for the decision to submit the manuscript for Oncol. 2015;33(34):4007–4014.
15 Pennell NA, Neal JW, Chaft JE, et al. SELECT: a phase II trial of
publication.
adjuvant erlotinib in patients with resected epidermal growth factor
receptor-mutant non-small-cell lung cancer. J Clin Oncol.
Data sharing statement 2019;37(2):97–104.
The authenticity of this article has been validated by uploading 16 Zhong WZ, Wang Q, Mao WM, et al. Gefitinib versus vinorelbine
the key raw data onto the Research Data Deposit public platform plus cisplatin as adjuvant treatment for stage II-IIIA (N1-N2) EGFR-
10 www.thelancet.com Vol 57 March, 2023
Articles
mutant NSCLC: final overall survival analysis of CTONG1104 26 Strauss GM, Herndon 2nd JE, Maddaus MA, et al. Adjuvant
phase III trial. J Clin Oncol. 2021;39(7):713–722. paclitaxel plus carboplatin compared with observation in stage IB
17 Yue D, Xu S, Wang Q, et al. Erlotinib versus vinorelbine plus non-small-cell lung cancer: CALGB 9633 with the cancer and leu-
cisplatin as adjuvant therapy in Chinese patients with stage IIIA kemia group B, radiation therapy Oncology group, and north cen-
EGFR mutation-positive non-small-cell lung cancer (EVAN): a tral cancer treatment group study groups. J Clin Oncol.
randomised, open-label, phase 2 trial. Lancet Respir Med. 2018;6(11): 2008;26(31):5043–5051.
863–873. 27 Mountain CF. Revisions in the international system for staging
18 He J, Su C, Liang W, et al. Icotinib versus chemotherapy as adju- lung cancer. Chest. 1997;111(6):1710–1717.
vant treatment for stage II-IIIA EGFR-mutant non-small-cell lung 28 Goldstraw P, Chansky K, Crowley J, et al. The IASLC lung
cancer (EVIDENCE): a randomised, open-label, phase 3 trial. Lancet cancer staging Project: proposals for revision of the
Respir Med. 2021;9(9):1021–1029. TNM stage groupings in the forthcoming (eighth) edition of the
19 Tada H, Mitsudomi T, Misumi T, et al. Randomized phase III TNM classification for lung cancer. J Thorac Oncol. 2016;11(1):
study of gefitinib versus cisplatin plus vinorelbine for patients with 39–51.
resected stage II-IIIA non-small-cell lung cancer with EGFR mu- 29 Zhong WZ, Wang Q, Mao WM, et al. Gefitinib versus vinorelbine
tation (IMPACT). J Clin Oncol. 2022;40(3):231–241. plus cisplatin as adjuvant treatment for stage II-IIIA (N1-N2) EGFR-
20 Cheng H, Li XJ, Wang XJ, et al. A meta-analysis of adjuvant EGFR- mutant NSCLC (ADJUVANT/CTONG1104): a randomised, open-
TKIs for patients with resected non-small cell lung cancer. Lung label, phase 3 study. Lancet Oncol. 2018;19(1):139–148.
Cancer. 2019;137:7–13. 30 Yue D, Xu S, Wang Q, et al. Updated overall survival and explor-
21 Wu YL, Tsuboi M, He J, et al. Osimertinib in resected EGFR- atory analysis from randomized, phase II EVAN study of erlotinib
mutated non-small-cell lung cancer. N Engl J Med. 2020;383(18): versus vinorelbine plus cisplatin adjuvant therapy in stage IIIA
1711–1723. epidermal growth factor Receptor+ non-small-cell lung cancer.
22 Koch AL, Vellanki PJ, Drezner N, et al. FDA approval summary: J Clin Oncol. 2022;40(34):3912–3917.
osimertinib for adjuvant treatment of surgically resected non-small 31 Gyawali B, West HJ. Lessons from ADAURA on adjuvant cancer
cell lung cancer, a collaborative Project orbis review. Clin Cancer drug trials: evidence, Ethics, and economics. J Clin Oncol.
Res. 2021;27(24):6638–6643. 2021;39(3):175–177.
23 Shi Y, Zhang L, Liu X, et al. Icotinib versus gefitinib in previously 32 Schoenfeld AJ, Yu HA. The evolving landscape of resistance to
treated advanced non-small-cell lung cancer (ICOGEN): a rando- osimertinib. J Thorac Oncol. 2020;15(1):18–21.
mised, double-blind phase 3 non-inferiority trial. Lancet Oncol. 33 Li N, Wang BX, Li J, et al. Perioperative circulating tumor DNA as a
2013;14(10):953–961. potential prognostic marker for operable stage I to IIIA non-small
24 Shi YK, Wang L, Han BH, et al. First-line icotinib versus cisplatin/ cell lung cancer. Cancer. 2022;128(4):708–718.
pemetrexed plus pemetrexed maintenance therapy for patients with 34 Zhang JT, Liu SY, Gao W, et al. Longitudinal undetectable molec-
advanced EGFR mutation-positive lung adenocarcinoma ular residual disease defines potentially cured population in local-
(CONVINCE): a phase 3, open-label, randomized study. Ann Oncol. ized non-small cell lung cancer. Cancer Discov. 2022;12(7):
2017;28(10):2443–2450. 1690–1701.
25 Goldstraw P, Crowley J, Chansky K, et al. The IASLC Lung Cancer 35 Ahn M, Jung HA, Ku BM, et al. Longitudinal monitoring of
Staging Project: proposals for the revision of the TNM stage circulating tumor DNA from plasma in patients with curative
groupings in the forthcoming (seventh) edition of the TNM Clas- resected stage IA-IIIA EGFR mutant non-small cell lung cancer.
sification of malignant tumours. J Thorac Oncol. 2007;2(8):706–714. Ann Oncol. 2022;33(suppl_7):S427–S437.
www.thelancet.com Vol 57 March, 2023 11
You might also like
- Osimertinib in Resected EGFR-Mutated Non-Small-Cell Lung CancerDocument13 pagesOsimertinib in Resected EGFR-Mutated Non-Small-Cell Lung CancerYTM LoongNo ratings yet
- Wu YL. Pubmed - ARCHER 1050Document13 pagesWu YL. Pubmed - ARCHER 1050della.ps2310No ratings yet
- Concomitant Genetic Alterations Are Associated With Worse Clinical Outcome in EGFR Mutant NSCLC Patients Treated With Tyrosine Kinase InhibitorsDocument7 pagesConcomitant Genetic Alterations Are Associated With Worse Clinical Outcome in EGFR Mutant NSCLC Patients Treated With Tyrosine Kinase InhibitorsDyahsekarayupudak wangiNo ratings yet
- Fonc 11 693386Document9 pagesFonc 11 693386Luana FerreiraNo ratings yet
- Tca 12 2161Document9 pagesTca 12 2161hafidisara05No ratings yet
- Recurrent Ta Low-Grade Non-Muscle-Invasive Bladder Cancer: What Are The Options?Document7 pagesRecurrent Ta Low-Grade Non-Muscle-Invasive Bladder Cancer: What Are The Options?Dr. Alexandre SatoNo ratings yet
- First-Line Crizotinib Versus Chemotherapy in ALK-Positive Lung CancerDocument11 pagesFirst-Line Crizotinib Versus Chemotherapy in ALK-Positive Lung CancerRitam JoarderNo ratings yet
- 2017 - CiMAvax-EGF - A New Therapeutic Vaccine Fron Adv NSCLC PatientsDocument7 pages2017 - CiMAvax-EGF - A New Therapeutic Vaccine Fron Adv NSCLC PatientsDanay Saavedra HernandezNo ratings yet
- Switch To EGFR TKI After Upfront Platinum Doublet Inductio - 2022 - Cancer TreatDocument6 pagesSwitch To EGFR TKI After Upfront Platinum Doublet Inductio - 2022 - Cancer Treatyuris hikmanNo ratings yet
- 10.1136@jitc 2020 001662Document8 pages10.1136@jitc 2020 001662DonaldNo ratings yet
- Imunoterapi SNLC 3Document7 pagesImunoterapi SNLC 3aulidaweliNo ratings yet
- He 2021 Icotinib Versus Chemotherapy As Adjuvant Treatment For Stage II-IIIA EGFR-mutant Non-Small-Cell Lung Cancer (EVIDENCE) A Randomised, Open-Label, Phase 3 TrialDocument9 pagesHe 2021 Icotinib Versus Chemotherapy As Adjuvant Treatment For Stage II-IIIA EGFR-mutant Non-Small-Cell Lung Cancer (EVIDENCE) A Randomised, Open-Label, Phase 3 TriallutfiaNo ratings yet
- Kinase Inhibitors Increase Individual Radiation Sensitivity in Normal Cells of Cancer PatientsDocument11 pagesKinase Inhibitors Increase Individual Radiation Sensitivity in Normal Cells of Cancer Patientsyuta titeNo ratings yet
- Nejme 2029532Document3 pagesNejme 2029532d_yee90No ratings yet
- Hemdan 2014Document6 pagesHemdan 2014DavorIvanićNo ratings yet
- Aspirin Sensitizes Osimertinib-Resistant NSCLC CelDocument35 pagesAspirin Sensitizes Osimertinib-Resistant NSCLC CelLeung iSamNo ratings yet
- Advancesintreatmentof Locallyadvancedor Metastaticnon-Smallcelllung CancerDocument13 pagesAdvancesintreatmentof Locallyadvancedor Metastaticnon-Smallcelllung CancerKaren GuerreroNo ratings yet
- Phase II INTERACT-ION Study: Ezabenlimab (BI 754091) and MDCF (Docetaxel, Cisplatin, and 5-Fluorouracil) Followed by Chemoradiotherapy in Patients With Stage III Squamous Cell Anal CarcinomaDocument11 pagesPhase II INTERACT-ION Study: Ezabenlimab (BI 754091) and MDCF (Docetaxel, Cisplatin, and 5-Fluorouracil) Followed by Chemoradiotherapy in Patients With Stage III Squamous Cell Anal CarcinomaStefano KimNo ratings yet
- JurnalDocument2 pagesJurnalElizabeth Puji YantiNo ratings yet
- Eddy 2007Document8 pagesEddy 2007Mimsy Quiñones TafurNo ratings yet
- Medi 95 E4797Document5 pagesMedi 95 E4797tika apriliaNo ratings yet
- Slater Case Presentation Issue 1 Article For WebsiteDocument2 pagesSlater Case Presentation Issue 1 Article For Websiteapi-400507461No ratings yet
- Neoadjuvant Chemoradiotherapy Followed by Surgery VersusDocument15 pagesNeoadjuvant Chemoradiotherapy Followed by Surgery VersusRaul Matute MartinNo ratings yet
- 10 1056@NEJMoa1900574 PDFDocument9 pages10 1056@NEJMoa1900574 PDFGhadah AlyousifNo ratings yet
- Gynecology and Minimally Invasive Therapy: Case ReportDocument5 pagesGynecology and Minimally Invasive Therapy: Case ReportMetharisaNo ratings yet
- Masood 2019Document13 pagesMasood 2019Andreea CohnNo ratings yet
- JMP 02 00022Document19 pagesJMP 02 00022Peterpan NguyenNo ratings yet
- Luo2010 PDFDocument7 pagesLuo2010 PDFAnisa D KharismaNo ratings yet
- 166440996249740030Document10 pages166440996249740030111No ratings yet
- Furmonertinib (AST2818) Versus Gefitinib As FirstDocument10 pagesFurmonertinib (AST2818) Versus Gefitinib As FirstCláudia SilvaNo ratings yet
- ESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 14Document1 pageESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 14EDWIN WIJAYANo ratings yet
- Validation of The Meet URO Score in Patients WithDocument9 pagesValidation of The Meet URO Score in Patients Withveaceslav coscodanNo ratings yet
- Heymach-2022-Design and Rationale For A Phase1Document5 pagesHeymach-2022-Design and Rationale For A Phase1Luca BertolacciniNo ratings yet
- Secpnd Line 1-S2.0-S0959804918315399-MainDocument8 pagesSecpnd Line 1-S2.0-S0959804918315399-MainmariNo ratings yet
- Colorectal Cancer Immune Infiltrates - Significance in Patient Prognosis andDocument13 pagesColorectal Cancer Immune Infiltrates - Significance in Patient Prognosis andOvamelia JulioNo ratings yet
- Article LCA ConfCycle2 1617fevrier2023Document9 pagesArticle LCA ConfCycle2 1617fevrier2023parasite myNo ratings yet
- OSIMERTINIB NNEJM - 2018 - Jan - 11 - 378 (2) - 113Document13 pagesOSIMERTINIB NNEJM - 2018 - Jan - 11 - 378 (2) - 113alberto cabelloNo ratings yet
- Fonc 12 834704Document7 pagesFonc 12 834704band pulmounandNo ratings yet
- Histopathologic Analysis of Ct-Guided Core Needle Biopsy in Radiologically Detected Suspicious Mediastinal and Lung Mass: Two Years' Study in Tertiary HospitalDocument4 pagesHistopathologic Analysis of Ct-Guided Core Needle Biopsy in Radiologically Detected Suspicious Mediastinal and Lung Mass: Two Years' Study in Tertiary HospitalDesiree MejicaNo ratings yet
- Ra - Lung AdenocarcinomaDocument7 pagesRa - Lung Adenocarcinomamuhammad irsyad khresna ajiNo ratings yet
- 18 Detection of Rare Mutations in EGFR-ARMS-PCR-Negative Lung Adenocarcinoma by Sanger SequencingDocument7 pages18 Detection of Rare Mutations in EGFR-ARMS-PCR-Negative Lung Adenocarcinoma by Sanger Sequencingdiana manuella minkoue kemgueNo ratings yet
- ESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 8Document1 pageESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 8EDWIN WIJAYANo ratings yet
- Jurnal Onklogi ParuDocument14 pagesJurnal Onklogi ParuirfanNo ratings yet
- Uganda - CervixDocument9 pagesUganda - CervixDaniel PalmeraNo ratings yet
- Cancer Science & Therapy Cancer Science & TherapyDocument6 pagesCancer Science & Therapy Cancer Science & TherapyHedo HidayatNo ratings yet
- Prognostic Value and Adverse Events of Cytoreductive Surgery With Hyperthermic Intraperitoneal Chemotherapy in Primary Advanced and PlatinumDocument14 pagesPrognostic Value and Adverse Events of Cytoreductive Surgery With Hyperthermic Intraperitoneal Chemotherapy in Primary Advanced and PlatinumChris El HadiNo ratings yet
- Safety and Efficacy of Pembrolizumab in Advanced, Programmed Death Ligand 1-Positive Cervical CancerDocument9 pagesSafety and Efficacy of Pembrolizumab in Advanced, Programmed Death Ligand 1-Positive Cervical CancerluizaNo ratings yet
- Diffuse Malignant Peritoneal Mesothelioma PDFDocument9 pagesDiffuse Malignant Peritoneal Mesothelioma PDFAndreeaPopescuNo ratings yet
- Gemcitabine Vs BCGDocument8 pagesGemcitabine Vs BCGmulkikimulNo ratings yet
- Differences in Outcome For Cervical Cancer Patients Treated With or Without BrachytherapyDocument8 pagesDifferences in Outcome For Cervical Cancer Patients Treated With or Without BrachytherapyNurul Hikmah SNo ratings yet
- Adoptive Transfer of Natural Killer Cells in Combination With Chemotherapy Improves Outcomes of Patients With Locally Advanced Colon Carcinoma.Document15 pagesAdoptive Transfer of Natural Killer Cells in Combination With Chemotherapy Improves Outcomes of Patients With Locally Advanced Colon Carcinoma.Andrew ChenNo ratings yet
- Nakachi 2018Document4 pagesNakachi 2018Nikos SerifisNo ratings yet
- Chua 2005 Long-Term Survival After Cisplatin-Based InductionDocument7 pagesChua 2005 Long-Term Survival After Cisplatin-Based InductionFitria WaffiNo ratings yet
- 31576697Document8 pages31576697Ahana MukherjeeNo ratings yet
- Sciencedirect: Original ResearchDocument8 pagesSciencedirect: Original ResearchThiamNo ratings yet
- Cisplatin-Based Chemoradiation Plus Cetuximab in Head and Neck Cancer Ann Oncol-2010-Merlano-annonc - mdq412Document6 pagesCisplatin-Based Chemoradiation Plus Cetuximab in Head and Neck Cancer Ann Oncol-2010-Merlano-annonc - mdq412ZuriNo ratings yet
- ESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 9Document1 pageESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 9EDWIN WIJAYANo ratings yet
- Pearls and Pitfalls in The Imaging of Targeted Therapy and Immunotherapy in Lung CancerDocument11 pagesPearls and Pitfalls in The Imaging of Targeted Therapy and Immunotherapy in Lung CancerNelson William UsnayoNo ratings yet
- Targeted Therapies for Lung CancerFrom EverandTargeted Therapies for Lung CancerRavi SalgiaNo ratings yet
- Annotated Answers To Gordis, Epidemiology, 4th Edition QuestionsDocument3 pagesAnnotated Answers To Gordis, Epidemiology, 4th Edition Questionssdverde100% (1)
- Radiation Protection Bushong Study GuideDocument6 pagesRadiation Protection Bushong Study GuideAsha6842100% (1)
- Final Na NiDocument60 pagesFinal Na NiJeza Bayabos83% (12)
- Clinical Methods in ENT by P. T. WakodeDocument229 pagesClinical Methods in ENT by P. T. WakodeQuranSunnat100% (1)
- Professor (DR) Rama Kant Biodata Curriculum VitaeDocument50 pagesProfessor (DR) Rama Kant Biodata Curriculum VitaebobbyramakantNo ratings yet
- Hypothalamus-Pituitary-Thyroid Axis: PRESENTERS: DR: Nyangaresi Justine DR: Mitchelle Facilitator: DRDocument31 pagesHypothalamus-Pituitary-Thyroid Axis: PRESENTERS: DR: Nyangaresi Justine DR: Mitchelle Facilitator: DRJustine NyangaresiNo ratings yet
- 5th Vital SignDocument20 pages5th Vital SignDenisse Shazz Mae MaretNo ratings yet
- Đề Thi ThửDocument242 pagesĐề Thi ThửLê Trung Kiên52% (73)
- National Guidelines For The Management of Sexually Transmitted Infections-Oa6yxme8Document84 pagesNational Guidelines For The Management of Sexually Transmitted Infections-Oa6yxme8HabtamNo ratings yet
- Pathophysiology: AppendicitisDocument3 pagesPathophysiology: AppendicitisEqah TajuddinNo ratings yet
- Cervical Polyps - Causes - Symptoms - Management - TeachMeObGynDocument2 pagesCervical Polyps - Causes - Symptoms - Management - TeachMeObGynmohanNo ratings yet
- MenopauseDocument52 pagesMenopauseGaoudam NatarajanNo ratings yet
- Pembrolizumab Treatment For Progressive Multifocal LeukoencephalopathyDocument8 pagesPembrolizumab Treatment For Progressive Multifocal LeukoencephalopathyAnonymous Kv0sHqFNo ratings yet
- Portosystemic Encephalopathy - Background, Pathophysiology, EtiologyDocument6 pagesPortosystemic Encephalopathy - Background, Pathophysiology, EtiologyAnonymous 0ed3QYB2No ratings yet
- Mobiltrans HD-30Document10 pagesMobiltrans HD-30Sebastian FuentesNo ratings yet
- PDF Wk4 - 04 Bradford Hill CriteriaDocument5 pagesPDF Wk4 - 04 Bradford Hill Criteriajackbane69No ratings yet
- Placenta PreviaDocument2 pagesPlacenta PreviaJorge De VeraNo ratings yet
- Siopel 6Document137 pagesSiopel 6Caballero X CaballeroNo ratings yet
- Fennel Foeniculum Materia Medica HerbsDocument4 pagesFennel Foeniculum Materia Medica HerbsAlejandra GuerreroNo ratings yet
- Clinical Atlas of Canine and Feline Dermatology - 2019 - Coyner - IndexDocument12 pagesClinical Atlas of Canine and Feline Dermatology - 2019 - Coyner - Indexnabal22No ratings yet
- Diseases of The Pharynx: BY DR Arif Raza Khan Assistant Professor E.N.T. K.T.HDocument29 pagesDiseases of The Pharynx: BY DR Arif Raza Khan Assistant Professor E.N.T. K.T.HSuleman MuhammadNo ratings yet
- Common Craniofacial Anomalies. Conditions of Craniofacial AtrophyHypoplasia and NeoplasiaDocument14 pagesCommon Craniofacial Anomalies. Conditions of Craniofacial AtrophyHypoplasia and NeoplasiaPaola LoloNo ratings yet
- Radiology 1Document4 pagesRadiology 1sha100% (3)
- Accident StudiesDocument63 pagesAccident Studiesmanaliamit100% (1)
- Unit III Plant Disease and SymptomsDocument23 pagesUnit III Plant Disease and SymptomsKhenan James NarismaNo ratings yet
- Pathophysiology Community Aquired Pneumonia and AnemiaDocument3 pagesPathophysiology Community Aquired Pneumonia and Anemiapa3kmedina100% (2)
- Outcomes of Recurrent cSCCADocument7 pagesOutcomes of Recurrent cSCCAPrincess B. MaristelaNo ratings yet
- Skippers United Pacific, Inc. vs. Lagne DigestDocument4 pagesSkippers United Pacific, Inc. vs. Lagne DigestEmir MendozaNo ratings yet
- Pathophysiology A Clinical Approach 2nd Edition Braun Anderson Test BankDocument36 pagesPathophysiology A Clinical Approach 2nd Edition Braun Anderson Test Bankbeswikemysteryy6rpNo ratings yet
- Bleeding in Early Late PregnancyDocument46 pagesBleeding in Early Late PregnancyAndrada Catrinoiu100% (2)