You might also like
- Commented (CW1) : This Language and Footnotes To ItDocument2 pagesCommented (CW1) : This Language and Footnotes To ItChris90% (10)
- (SINOVAC) Informed Consent Form - Eng March 5 2021Document1 page(SINOVAC) Informed Consent Form - Eng March 5 2021Mark Anthony RosasNo ratings yet
- New Corona Form Revised Version-7Document1 pageNew Corona Form Revised Version-7Rishabh JainNo ratings yet
- Name of The Life To Be Assured:: Proposal NoDocument1 pageName of The Life To Be Assured:: Proposal Noபிரேம் முருகன்No ratings yet
- Life Insurance Corporation of India Novel Coronavirus (Covid-19) Questionnaire (Revised Version - 5)Document1 pageLife Insurance Corporation of India Novel Coronavirus (Covid-19) Questionnaire (Revised Version - 5)பிரேம் முருகன்No ratings yet
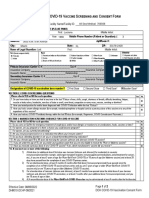
- COVID-19 Vaccine Screening and Agreement: Contact Information - Person Being VaccinatedDocument7 pagesCOVID-19 Vaccine Screening and Agreement: Contact Information - Person Being VaccinatedLuz VelezNo ratings yet
- Till 01.01.2020. If Yes ,: Annexure-I Life Insurance Corporation of IndiaDocument2 pagesTill 01.01.2020. If Yes ,: Annexure-I Life Insurance Corporation of IndiaManjunathNo ratings yet
- CDC COVID ScreeningDocument4 pagesCDC COVID ScreeningDaniel KrugNo ratings yet
- Boosters Informed Consent Form ENGDocument1 pageBoosters Informed Consent Form ENGMoi ValdozNo ratings yet
- Factsheet priorCOVID19infection ENGDocument5 pagesFactsheet priorCOVID19infection ENGVasilije MunjasNo ratings yet
- Informed Consent Form Pfizer EnglishDocument2 pagesInformed Consent Form Pfizer EnglishIway SheenaNo ratings yet
- Pfizer Consent Form - FillableDocument8 pagesPfizer Consent Form - FillableAbraham Baeza - Viajes PegüisNo ratings yet
- Undertaking Declaration PD2022 - 030Document2 pagesUndertaking Declaration PD2022 - 030MejoNo ratings yet
- COVD 19 Vaction Form 2020 Pfizerv2Document1 pageCOVD 19 Vaction Form 2020 Pfizerv2Neel YoyoNo ratings yet
- Covid-19 Test Claim FormDocument2 pagesCovid-19 Test Claim Formmuhammad anasNo ratings yet
- (Informed Consent) Covid-19 Vaccine Forms EngDocument1 page(Informed Consent) Covid-19 Vaccine Forms EngYosh PamatmatNo ratings yet
- COVID-19 (Coronavirus) Exposure Questionnaire: Please Answer The Following Questions in As Much Detail As PossibleDocument2 pagesCOVID-19 (Coronavirus) Exposure Questionnaire: Please Answer The Following Questions in As Much Detail As PossibleDharm prakashNo ratings yet
- Covid Vaccine Clover Form2948Document1 pageCovid Vaccine Clover Form2948marian2277No ratings yet
- COVID-19 Vaccine Frequently Asked Questions April 1, 2022 New/Updated Information Is Highlighted in YellowDocument14 pagesCOVID-19 Vaccine Frequently Asked Questions April 1, 2022 New/Updated Information Is Highlighted in YellowMadonna FletcherNo ratings yet
- Consent Form (Sinovac)Document1 pageConsent Form (Sinovac)Kresta BenignoNo ratings yet
- Pfizer Informed Consent Form Eng - April 15 2021Document1 pagePfizer Informed Consent Form Eng - April 15 2021Christie ConalesNo ratings yet
- PEDIA Informed Consent Form PfizerDocument2 pagesPEDIA Informed Consent Form PfizerBalba ChrislynNo ratings yet
- Get The Facts About COVID-19 Vaccines - Mayo ClinicDocument10 pagesGet The Facts About COVID-19 Vaccines - Mayo ClinicLuna BellatrixNo ratings yet
- Information On Vaccination-Differentiated Safe Management Measures (SMMS)Document9 pagesInformation On Vaccination-Differentiated Safe Management Measures (SMMS)Goh Yong DaNo ratings yet
- Pfizer (Informed Consent Form) Eng - April 15 2021Document1 pagePfizer (Informed Consent Form) Eng - April 15 2021aleiah jean libatiqueNo ratings yet
- Covid QuestionnaireDocument1 pageCovid QuestionnaireAshher UsmaniNo ratings yet
- Risk of COVID-19 Disease Transmission During IVF Treatment WaiverDocument2 pagesRisk of COVID-19 Disease Transmission During IVF Treatment WaiveraleonalonsoNo ratings yet
- COVID-19 Test Claim Form - 23122020 Woking File - ENG - FinalDocument2 pagesCOVID-19 Test Claim Form - 23122020 Woking File - ENG - FinalnorhanaaNo ratings yet
- Script For COVID Vaccination. V1.1Document6 pagesScript For COVID Vaccination. V1.1Vikram AripakaNo ratings yet
- Condado de Los Ángeles: Vacunas Contra El Covid-19-Preguntas Frecuentes (Faq)Document16 pagesCondado de Los Ángeles: Vacunas Contra El Covid-19-Preguntas Frecuentes (Faq)Shakira MonqueNo ratings yet
- Registration and Consent Form For Covid 19 Vaccination 05.03.21Document4 pagesRegistration and Consent Form For Covid 19 Vaccination 05.03.21Yash HardowarNo ratings yet
- Adobe Scan Jun 24, 2021Document2 pagesAdobe Scan Jun 24, 2021Camila Fernandez SandovalNo ratings yet
- Life Insurance Corporation of India Annexure-I Novel Coronavirus (Covid-19) QuestionnaireDocument2 pagesLife Insurance Corporation of India Annexure-I Novel Coronavirus (Covid-19) QuestionnaireshahnawazNo ratings yet
- BivalentConsent LucianaPedrosopessoa 559154Document2 pagesBivalentConsent LucianaPedrosopessoa 559154Tatah SouzaNo ratings yet
- Pfizer COVID-19 FlyerDocument2 pagesPfizer COVID-19 FlyerFrank MaradiagaNo ratings yet
- Fact Sheet For Recipients and CaregiversDocument6 pagesFact Sheet For Recipients and Caregiversapi-537351752No ratings yet
- Guideline For The Admission and Hospital Management of Pregnant Women/Individuals Who Are A Confirmed or Suspect Case of COVID-19Document8 pagesGuideline For The Admission and Hospital Management of Pregnant Women/Individuals Who Are A Confirmed or Suspect Case of COVID-19asm obginNo ratings yet
- COVID-19 Guidance For Individuals Vaccinated Outside of OntarioDocument5 pagesCOVID-19 Guidance For Individuals Vaccinated Outside of OntarioLawrence VaIenciaNo ratings yet
- Workday Philippines Job Aid Self Declaration For Your COVID 19 Vaccination StatusDocument3 pagesWorkday Philippines Job Aid Self Declaration For Your COVID 19 Vaccination StatusMay Ann Mamado OlaerNo ratings yet
- COVID 19 Consent FormDocument2 pagesCOVID 19 Consent FormfvdssfdNo ratings yet
- HC W CompensationDocument4 pagesHC W CompensationSweet SimyunnNo ratings yet
- Answering Residents Loved Ones QuestionsDocument2 pagesAnswering Residents Loved Ones Questions13WMAZNo ratings yet
- Is The COVID-19 Vaccine Safe?: Name: Joseph C. Landayan Section: STEM 5Document6 pagesIs The COVID-19 Vaccine Safe?: Name: Joseph C. Landayan Section: STEM 5Joseph LandayanNo ratings yet
- Moderna Informed Consent Form Eng June 18 2021Document1 pageModerna Informed Consent Form Eng June 18 2021Bruce GonzalesNo ratings yet
- Pfizer-BioNTech COVID-19 Vaccine EUA Fact Sheet For Recipients-withMCIR 710411 7Document6 pagesPfizer-BioNTech COVID-19 Vaccine EUA Fact Sheet For Recipients-withMCIR 710411 7Jean SaisTropNo ratings yet
- 1215 Pfizer BIONTECH COVID-19 VACCINEDocument6 pages1215 Pfizer BIONTECH COVID-19 VACCINEWLTX0% (1)
- Change Notification No 73 - COVID-19 Vaccine - WBDSGDocument4 pagesChange Notification No 73 - COVID-19 Vaccine - WBDSGJill ValdesNo ratings yet
- COVID Vaccination Packet SFODocument16 pagesCOVID Vaccination Packet SFOferNo ratings yet
- Motion: The Rise of Covid 19 Vaccination Activities in IndonesiaDocument14 pagesMotion: The Rise of Covid 19 Vaccination Activities in IndonesiaAlyvia Risvianti PutriNo ratings yet
- Pre Vaccination Screening FormDocument10 pagesPre Vaccination Screening Formbersabeh abayNo ratings yet
- COVID-19 Guidance For Individuals Vaccinated Outside of OntarioDocument13 pagesCOVID-19 Guidance For Individuals Vaccinated Outside of OntarioAda Belen AlvarezNo ratings yet
- COVID 19 Protocol For Proof Full Vaccination Events Activities enDocument19 pagesCOVID 19 Protocol For Proof Full Vaccination Events Activities enRico MaligayaNo ratings yet
- Covid-19 Self Declaration For Appearing in Phyiscial Training Conducted by The Nirc of Icai, DelhiDocument1 pageCovid-19 Self Declaration For Appearing in Phyiscial Training Conducted by The Nirc of Icai, DelhiNipun AggarwalNo ratings yet
- Frequently Asked Questions On COVID-19 Vaccine: Target Group: General Public S. No. Potential ResponseDocument8 pagesFrequently Asked Questions On COVID-19 Vaccine: Target Group: General Public S. No. Potential ResponseCNBCTV18 DigitalNo ratings yet
- Respondent Broadly and Proactivly Disseminated Inaccurate Information Regarding Covid-19 Infection PrecautionsDocument25 pagesRespondent Broadly and Proactivly Disseminated Inaccurate Information Regarding Covid-19 Infection PrecautionsAlicia PoweNo ratings yet
- Proof of Full Vaccination Guide For BusinessesDocument17 pagesProof of Full Vaccination Guide For BusinessesSteveNo ratings yet
- Informed Consent UniversalDocument1 pageInformed Consent Universalahasgahsg031No ratings yet
- EUA 27034.167 - FS For Recipients and Caregivers - Final - 5.10.2021Document7 pagesEUA 27034.167 - FS For Recipients and Caregivers - Final - 5.10.2021Diona SmithNo ratings yet