You might also like
- Module 2B - Readiness For Enhanced Breastfeeding - BSN 2ADocument4 pagesModule 2B - Readiness For Enhanced Breastfeeding - BSN 2ALuis Gatchalian Lacanilao100% (2)
- Ineffective Breast FeedingDocument5 pagesIneffective Breast Feedingcamilleandaj070575% (12)
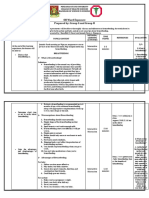
- OB Ward Exposure Prepared By: Group G and Group HDocument10 pagesOB Ward Exposure Prepared By: Group G and Group HJannah Marie A. DimaporoNo ratings yet
- Health Education On Breast FeedingDocument10 pagesHealth Education On Breast FeedingSoumya Rajeswari100% (3)
- Health Teaching PlanDocument4 pagesHealth Teaching PlanLovely Anne ArqueroNo ratings yet
- Academy of Breastfeeding Medicine's 2017 Position Statement On Informal Breast Milk Sharing For The Term Healthy InfantDocument3 pagesAcademy of Breastfeeding Medicine's 2017 Position Statement On Informal Breast Milk Sharing For The Term Healthy InfantClara Fynbu EggertNo ratings yet
- Steps To Successfully Breastfeed The Premature InfantDocument10 pagesSteps To Successfully Breastfeed The Premature InfantKholis FaisolNo ratings yet
- What Is Breastfeeding? Benefits of Breastfeeding?: Lessens The Risk of SIDSDocument2 pagesWhat Is Breastfeeding? Benefits of Breastfeeding?: Lessens The Risk of SIDSGarmaine ApostolNo ratings yet
- Teaching Plan For Proper Breast Feeding Begh ErDocument7 pagesTeaching Plan For Proper Breast Feeding Begh ErAmira Fatmah QuilapioNo ratings yet
- Mobbs Et Al-2016-Acta PaediatricaDocument6 pagesMobbs Et Al-2016-Acta Paediatricamhelanhie_09No ratings yet
- Metode Pemberian Asi 1Document4 pagesMetode Pemberian Asi 1cece likaNo ratings yet
- Breast Feeding Health TalkDocument12 pagesBreast Feeding Health TalkSanjeet DuhanNo ratings yet
- WNHS OG AbdominalExaminationDocument6 pagesWNHS OG AbdominalExaminationPanJan BalNo ratings yet
- Mothers' Breastfeeding Experiences in The NICUDocument8 pagesMothers' Breastfeeding Experiences in The NICUmourienNo ratings yet
- Breastfeeding Challenges Lau2017 Lactancia PremturDocument10 pagesBreastfeeding Challenges Lau2017 Lactancia PremturdeboraNo ratings yet
- Editorial: Breastmilk: It's Not Just For Breakfast Anymore!Document1 pageEditorial: Breastmilk: It's Not Just For Breakfast Anymore!lila bNo ratings yet
- Maria Asuncion Silvestre: Improving Neonatal CareDocument2 pagesMaria Asuncion Silvestre: Improving Neonatal CareGeorge AngelesNo ratings yet
- BrestfeedingDocument2 pagesBrestfeedingBuhkz Hermoso100% (1)
- Potential Complications Signs and SymptomsDocument2 pagesPotential Complications Signs and SymptomsJessica GomezNo ratings yet
- Scientific Article: A Longitudinal Study of The Association Between Breast-Feeding and Harmful Oral HabitsDocument5 pagesScientific Article: A Longitudinal Study of The Association Between Breast-Feeding and Harmful Oral HabitsJuan JoséNo ratings yet
- Harmful Substance To Avoid During PregnancyDocument3 pagesHarmful Substance To Avoid During PregnancyLhekha RaviendranNo ratings yet
- Nursing Care Plan Data Nursing Diagnoses Goals and Outcomes Nursing Interventions Rationale EvaluationDocument5 pagesNursing Care Plan Data Nursing Diagnoses Goals and Outcomes Nursing Interventions Rationale EvaluationClaudineNo ratings yet
- Canfamphys00151 0103Document5 pagesCanfamphys00151 0103siskaNo ratings yet
- Health Talk On BFDocument28 pagesHealth Talk On BFpriyanka75% (8)
- Veneracion NCP 1Document2 pagesVeneracion NCP 1Romm JacobNo ratings yet
- Konsep Ra Ā'ah Dalam Al-Quran (Kajian Tafsir Tematik Ayat-Ayat Tentang Menyusui Bayi Dalam Perspektif Mufassir Dan Sains)Document14 pagesKonsep Ra Ā'ah Dalam Al-Quran (Kajian Tafsir Tematik Ayat-Ayat Tentang Menyusui Bayi Dalam Perspektif Mufassir Dan Sains)Hardianty HarviyahNo ratings yet
- (Doi 10.1016/B978!1!4377-0788-5.10014-8) Lawrence, Ruth A. - Breastfeeding - Breastfeeding Infants With ProblemsDocument41 pages(Doi 10.1016/B978!1!4377-0788-5.10014-8) Lawrence, Ruth A. - Breastfeeding - Breastfeeding Infants With ProblemsBray Yvc SaNo ratings yet
- Nursing Care Plan For Interrupted Breastfeeding NCPDocument3 pagesNursing Care Plan For Interrupted Breastfeeding NCPSaira SucgangNo ratings yet
- NURSING CARE PLAN Interrupted Breastfeeding: Student Nurses' CommunityDocument3 pagesNURSING CARE PLAN Interrupted Breastfeeding: Student Nurses' CommunitySaira SucgangNo ratings yet
- Healthy Birth Practice 6 - Keep Mother and Baby Together Its Best For Mother Baby and BreastfeedingDocument7 pagesHealthy Birth Practice 6 - Keep Mother and Baby Together Its Best For Mother Baby and BreastfeedingchewychockoNo ratings yet
- Nursing Intervention - Cleft PalateDocument2 pagesNursing Intervention - Cleft PalateKyle VargasNo ratings yet
- Macronutrient Digestion and Absorption in The Preterm InfantDocument14 pagesMacronutrient Digestion and Absorption in The Preterm InfantSanjuy GzzNo ratings yet
- Breast Fedding Health TalkDocument9 pagesBreast Fedding Health TalkShahin ShekhNo ratings yet
- Presentation 1 StanyamrutamDocument1 pagePresentation 1 StanyamrutamNamrata DahakeNo ratings yet
- Dr-Nursing Care PlanDocument2 pagesDr-Nursing Care PlanKhrisha Anne Davillo100% (1)
- Maternal & Child Health NursingDocument24 pagesMaternal & Child Health NursingFranz goNo ratings yet
- Cleft Lip and PalateDocument8 pagesCleft Lip and PalateSHEILA MAE SACLOTNo ratings yet
- Exclusive Breast-Feeding Is MotivationDocument8 pagesExclusive Breast-Feeding Is MotivationsmokaNo ratings yet
- Newborn & Infant Nursing Reviews: Janeen Cross, DSW, MSW, Mba, LCSW, AcswDocument4 pagesNewborn & Infant Nursing Reviews: Janeen Cross, DSW, MSW, Mba, LCSW, AcswHatice KaraNo ratings yet
- Adiel Joy P. Calsa ASYNCHRONOUS ACTIVITY (WEEK 2 - 3)Document2 pagesAdiel Joy P. Calsa ASYNCHRONOUS ACTIVITY (WEEK 2 - 3)Adiel CalsaNo ratings yet
- Breastfeeding Challenges and The Preterm Mother-Infant Dyad A Conceptual ModelDocument10 pagesBreastfeeding Challenges and The Preterm Mother-Infant Dyad A Conceptual Modelunisa magisterNo ratings yet
- What Factors Influence The Progression of ChildbirthDocument9 pagesWhat Factors Influence The Progression of ChildbirthХристинаГулеваNo ratings yet
- Fernandez GROUP 2 NCP AND DS FORMAT LATESTDocument5 pagesFernandez GROUP 2 NCP AND DS FORMAT LATESTnaomie manaliliNo ratings yet
- Breastfeeding ManagementDocument16 pagesBreastfeeding ManagementggggangNo ratings yet
- Breastfeeding Benefits For BabyDocument4 pagesBreastfeeding Benefits For Babyedra gensonNo ratings yet
- Sumandeep Nursing College: Structured Teaching Programme ON Exclusive BreastfeedingDocument23 pagesSumandeep Nursing College: Structured Teaching Programme ON Exclusive BreastfeedingskylertNo ratings yet
- G Hid Montes Sory Pentru Bebelus IDocument42 pagesG Hid Montes Sory Pentru Bebelus Imelimatyas100% (1)
- Responsive Feeding: Supporting Close and Loving RelationshipsDocument4 pagesResponsive Feeding: Supporting Close and Loving RelationshipsAnnida HanifahNo ratings yet
- Breastfeeding "A Gift That Lasts A Lifetime"Document2 pagesBreastfeeding "A Gift That Lasts A Lifetime"Janine Mae MacaraigNo ratings yet
- Dad's: How To Know Baby Is Getting Enough Milk Things You Can DoDocument2 pagesDad's: How To Know Baby Is Getting Enough Milk Things You Can DoariniNo ratings yet
- 9B. Effectiveness of Educational Intervention On Breastfeeding Among Primi Pregnant WomanDocument6 pages9B. Effectiveness of Educational Intervention On Breastfeeding Among Primi Pregnant Womanagaua16No ratings yet
- Development of Infant Oral Feeding Skills What Do We Know1-3Document6 pagesDevelopment of Infant Oral Feeding Skills What Do We Know1-3Nur PramonoNo ratings yet
- A New Look at The Safety of Breastfeeding During Pregnancy - KellyMomDocument11 pagesA New Look at The Safety of Breastfeeding During Pregnancy - KellyMomdoggydogNo ratings yet
- Babywearing Best For BabyDocument16 pagesBabywearing Best For Babyfebria rockerNo ratings yet
- E20160772 FullDocument10 pagesE20160772 FullRaehana AlaydrusNo ratings yet
- Breast Feeding Tec.Document9 pagesBreast Feeding Tec.Chairali DodiyaNo ratings yet
- Teaching Plan For Breast FeedingDocument3 pagesTeaching Plan For Breast FeedingKramSenarevolNo ratings yet
- Jurnal Asi Craniofacial 2005Document9 pagesJurnal Asi Craniofacial 2005Masjid AlhudaNo ratings yet
- Sweet Milk Health Benefits Economic Advantages And Cultural Influences About BreastfeedingFrom EverandSweet Milk Health Benefits Economic Advantages And Cultural Influences About BreastfeedingNo ratings yet
- Umbilical Cord ProlapseDocument6 pagesUmbilical Cord ProlapseJules Cantal100% (3)
- Curriculum Vitae - DR ItaDocument2 pagesCurriculum Vitae - DR ItaZoel NikonianNo ratings yet
- The Paperless Partograph - The New User-Friendly and Simpler Tool For Monitoring LabourDocument5 pagesThe Paperless Partograph - The New User-Friendly and Simpler Tool For Monitoring LabourIOSRjournalNo ratings yet
- Syllabus Third Bams Prasuti Tantra Evum Stri Roga 120313Document26 pagesSyllabus Third Bams Prasuti Tantra Evum Stri Roga 120313Samprath SnayakNo ratings yet
- Midwifery Terminology: Mrs.V.Elizebeth Rani ReaderDocument14 pagesMidwifery Terminology: Mrs.V.Elizebeth Rani ReaderSamira MohamudNo ratings yet
- 3 ABSTRAK+ISI+DAPUS 1-11 InggrisDocument10 pages3 ABSTRAK+ISI+DAPUS 1-11 InggrisvirnaNo ratings yet
- Shoulder DystociaDocument18 pagesShoulder DystociaRadianty Haengbog Daeng FrederichaNo ratings yet
- Tocolytic Treatment in PregnancyDocument21 pagesTocolytic Treatment in PregnancyxxdrivexxNo ratings yet
- Contracted PelvisDocument48 pagesContracted Pelviskalpana shona100% (4)
- 17 JMSCRDocument5 pages17 JMSCRbela melizaNo ratings yet
- Rupture of The Uterus: Associate Professor Iolanda Blidaru, MD, PHDDocument21 pagesRupture of The Uterus: Associate Professor Iolanda Blidaru, MD, PHDOBGYN FKUI JAN-15No ratings yet
- Antecedents of CPDocument8 pagesAntecedents of CPЯковлев АлександрNo ratings yet
- Antenatal Care & ManagementDocument23 pagesAntenatal Care & ManagementPabhat Kumar100% (1)
- Preventive Obstetrics (By Mohan.s)Document52 pagesPreventive Obstetrics (By Mohan.s)mOHAN.S98% (55)
- Evaluation of The Effect of Antenatal Betamethasone On Neonatal Respiratory Morbidities in Late Preterm Deliveries (34-37 Weeks)Document9 pagesEvaluation of The Effect of Antenatal Betamethasone On Neonatal Respiratory Morbidities in Late Preterm Deliveries (34-37 Weeks)Rizka RamadaniNo ratings yet
- Obs Papers FinalizedDocument130 pagesObs Papers FinalizedRaffles HolmesNo ratings yet
- Chorioamnionitis and Prognosis For Term Infants-13Document5 pagesChorioamnionitis and Prognosis For Term Infants-13ronny29No ratings yet
- Persalinan. Yogyakarta: Yayasan Essentia MedicaDocument2 pagesPersalinan. Yogyakarta: Yayasan Essentia MedicaYemimaNo ratings yet
- Covid PregnancyDocument3 pagesCovid PregnancyDianeNo ratings yet
- IUFD For 4th Year Medical StudentsDocument19 pagesIUFD For 4th Year Medical StudentsDegefaw BikoyNo ratings yet
- Literature Review On Prevalence of Anemia in PregnancyDocument4 pagesLiterature Review On Prevalence of Anemia in Pregnancyc5pdd0qgNo ratings yet
- Planning and Intervention in Intrapartum CareDocument5 pagesPlanning and Intervention in Intrapartum CareAngela MariaNo ratings yet
- Aida Ayu Mailinda SariDocument11 pagesAida Ayu Mailinda SariMay El-MardhatillahNo ratings yet
- Maternal and Child HealthDocument62 pagesMaternal and Child HealthAsfand KhanNo ratings yet
- in Menstrual Cycle, The FSH-RF Secretes Which Hormone As A Response To Anterior Pituitary Gland Stimulation?Document41 pagesin Menstrual Cycle, The FSH-RF Secretes Which Hormone As A Response To Anterior Pituitary Gland Stimulation?charlinepingul19No ratings yet
- Smart Baby Shield Plus PLANDocument3 pagesSmart Baby Shield Plus PLANLim you enNo ratings yet
- Post Natal CareDocument15 pagesPost Natal CareDaphneyNo ratings yet
- Icds & MMRDocument42 pagesIcds & MMRsanjeev guptaNo ratings yet
- Preeclampsia and EclampsiaDocument24 pagesPreeclampsia and EclampsiaLuisa SarangayNo ratings yet
- Antenatal Care BenefitsDocument2 pagesAntenatal Care BenefitsashrafsabryNo ratings yet