You might also like
- Birth Weight and Gestational Age Factors for Cerebral Palsy and Seizure DisordersDocument5 pagesBirth Weight and Gestational Age Factors for Cerebral Palsy and Seizure DisordersЯковлев АлександрNo ratings yet
- The Complex Aetiology of Cerebral PalsyDocument16 pagesThe Complex Aetiology of Cerebral PalsyAileen MéndezNo ratings yet
- Schizophrenia Research: Herng-Ching Lin, I-Ju Chen, Yi-Hua Chen, Hsin-Chien Lee, Fang-Jen WuDocument6 pagesSchizophrenia Research: Herng-Ching Lin, I-Ju Chen, Yi-Hua Chen, Hsin-Chien Lee, Fang-Jen WucaesabooNo ratings yet
- Neonatal Complications of Term Pregnancy: Rates by Gestational Age Increase in A Continuous, Not Threshold, FashionDocument6 pagesNeonatal Complications of Term Pregnancy: Rates by Gestational Age Increase in A Continuous, Not Threshold, FashionAndreea BorislavschiNo ratings yet
- Risk Factor Assessment For Pre-Eclampsia: A Case Control StudyDocument6 pagesRisk Factor Assessment For Pre-Eclampsia: A Case Control StudyPutra SeptiansyahNo ratings yet
- Neonatal Outcomes of Extremely Preterm Infants From The NICHD Neonatal Research NetworkDocument14 pagesNeonatal Outcomes of Extremely Preterm Infants From The NICHD Neonatal Research NetworkKattia FloresNo ratings yet
- 33873-Article Text-121761-1-10-20170831Document6 pages33873-Article Text-121761-1-10-20170831AnggaNo ratings yet
- Paternal Age and PreeclampsiaDocument8 pagesPaternal Age and PreeclampsiaCebong KampretNo ratings yet
- Unintended Pregnancy, Prenatal Care, Newborn Outcomes, and Breastfeeding in Women With EpilepsyDocument10 pagesUnintended Pregnancy, Prenatal Care, Newborn Outcomes, and Breastfeeding in Women With EpilepsyasfwegereNo ratings yet
- An-Evaluation-Of-Risk-Factors-In-Cases-Of-Perinatal-Asphyxia-9563 2021Document4 pagesAn-Evaluation-Of-Risk-Factors-In-Cases-Of-Perinatal-Asphyxia-9563 2021Chiki CacaNo ratings yet
- Pregnancy Outcomes Following in Utero Exposure To Second-Generation AntipsychoticsDocument7 pagesPregnancy Outcomes Following in Utero Exposure To Second-Generation AntipsychoticsdanielaNo ratings yet
- Jp2011191a 2Document6 pagesJp2011191a 2AnapaolaNo ratings yet
- PIIS0002937822011115Document2 pagesPIIS0002937822011115Maria Fernanda Sigcho ValenciaNo ratings yet
- Seizures in Infancy in The Offspring of Women With Epilepsy 2019Document5 pagesSeizures in Infancy in The Offspring of Women With Epilepsy 2019Josefco RiveroNo ratings yet
- Associations of Snoring Frequency and Intensity in Pregnancy With Time-To - DeliveryDocument8 pagesAssociations of Snoring Frequency and Intensity in Pregnancy With Time-To - Delivery杨钦杰No ratings yet
- Preeclampsia and The Risk of Bronchopulmonary Dysplasia in VLBW Infants A Population Based StudyDocument7 pagesPreeclampsia and The Risk of Bronchopulmonary Dysplasia in VLBW Infants A Population Based Studyatika sgrtNo ratings yet
- Endo Met RitisDocument7 pagesEndo Met RitisdanielNo ratings yet
- Can Fundal Height Predict Weight or Twins?: SommaireDocument4 pagesCan Fundal Height Predict Weight or Twins?: SommairePandawa ObgynNo ratings yet
- DownloadDocument6 pagesDownloadKai GgNo ratings yet
- CLINICAL OBSTETRICS AND GYNECOLOGY: Causative Factors in Cerebral PalsyDocument14 pagesCLINICAL OBSTETRICS AND GYNECOLOGY: Causative Factors in Cerebral PalsyFauziah Dwi AprianiNo ratings yet
- Nihms425932 2013Document11 pagesNihms425932 2013Mario OcañaNo ratings yet
- Advances in Prenatal Screening For Down Syndrome - General Principles and Second Trimester TestingDocument16 pagesAdvances in Prenatal Screening For Down Syndrome - General Principles and Second Trimester TestingMáthé AdriennNo ratings yet
- Outcome of Teenage PregnancyDocument5 pagesOutcome of Teenage PregnancyKN DumpNo ratings yet
- Bjo12636 PDFDocument9 pagesBjo12636 PDFLuphly TaluvtaNo ratings yet
- Sera Valli 2014Document6 pagesSera Valli 2014Surraya JamshaidNo ratings yet
- Height in Chronic Kidney DiseaseDocument3 pagesHeight in Chronic Kidney DiseaseRosi IndahNo ratings yet
- Smoking and CHDDocument19 pagesSmoking and CHDAnonymous NeRC5JYiSNo ratings yet
- Cardiovascular Risk in Hypertension Open Question 13Document2 pagesCardiovascular Risk in Hypertension Open Question 13Nurulhuda RashidNo ratings yet
- Hypospadias and Early Gestation Growth Restriction in InfantsDocument8 pagesHypospadias and Early Gestation Growth Restriction in InfantsNaveed HussainNo ratings yet
- Artigo 3Document7 pagesArtigo 3Cirineu NetoNo ratings yet
- Mor 2016Document9 pagesMor 2016Farin MauliaNo ratings yet
- Phenotype-Directed Management of Hypertension in Pregnancy: Contemporary ReviewDocument18 pagesPhenotype-Directed Management of Hypertension in Pregnancy: Contemporary ReviewElmer MoscosoNo ratings yet
- Congenital Hyperinsulinism: A Practical Guide to Diagnosis and ManagementFrom EverandCongenital Hyperinsulinism: A Practical Guide to Diagnosis and ManagementDiva D. De León-CrutchlowNo ratings yet
- STUDENT EXCERCISES BOOK 2023-2024 - RemovedDocument13 pagesSTUDENT EXCERCISES BOOK 2023-2024 - RemovedRiris AriskaNo ratings yet
- Maternal Hypothyroidism During Pregnancy and The Risk of Pediatric Endocrine Morbidity in The OffspringDocument6 pagesMaternal Hypothyroidism During Pregnancy and The Risk of Pediatric Endocrine Morbidity in The OffspringlananhslssNo ratings yet
- Is breech presentation a risk factor for cerebral palsyDocument6 pagesIs breech presentation a risk factor for cerebral palsyPutriNo ratings yet
- Clinical Risk Factor For Preeclamsia in Twin PregnanciesDocument8 pagesClinical Risk Factor For Preeclamsia in Twin PregnanciesLouis HadiyantoNo ratings yet
- Improving Detection of Placenta Accreta with PAI Scoring SystemDocument2 pagesImproving Detection of Placenta Accreta with PAI Scoring SystemOmpNo ratings yet
- Validation of The Placenta Accreta Index (PAI) - Improving The Antenatal Diagnosis of The Morbidly Adherent PlacentaDocument2 pagesValidation of The Placenta Accreta Index (PAI) - Improving The Antenatal Diagnosis of The Morbidly Adherent PlacentaOmpNo ratings yet
- Medical Record Validation of Maternally Reported History of PreeclampsiDocument7 pagesMedical Record Validation of Maternally Reported History of PreeclampsiezaNo ratings yet
- Risk Factors for Cerebral Palsy in Children Born at TermDocument12 pagesRisk Factors for Cerebral Palsy in Children Born at TermRaditNo ratings yet
- Autism RiskDocument14 pagesAutism RiskAlina Topor Psi-MedicalNo ratings yet
- Knowledge On PIHDocument6 pagesKnowledge On PIHMadhusmita NayakNo ratings yet
- Maternal, Labor, Delivery, and Perinatal Outcomes Associated With Placental Abruption: A Systematic ReviewDocument23 pagesMaternal, Labor, Delivery, and Perinatal Outcomes Associated With Placental Abruption: A Systematic ReviewasfwegereNo ratings yet
- Lebanon - Congenital Anomalies Prevalence and Risk FactorsDocument7 pagesLebanon - Congenital Anomalies Prevalence and Risk FactorsAbdelrhman WagdyNo ratings yet
- Early Prediction of Preeclampsia in Pregnancy With Cell-Free RNADocument24 pagesEarly Prediction of Preeclampsia in Pregnancy With Cell-Free RNAAnahí TessaNo ratings yet
- 61 Goepfert2004Document7 pages61 Goepfert2004angela_karenina_1No ratings yet
- Diabetes in Children and Adolescents: A Guide to Diagnosis and ManagementFrom EverandDiabetes in Children and Adolescents: A Guide to Diagnosis and ManagementNo ratings yet
- Risk of Autism Associated With Hyperbilirubinemia and PhototherapyDocument10 pagesRisk of Autism Associated With Hyperbilirubinemia and Phototherapynurul habibaNo ratings yet
- Original Article: National Journal of Community Medicine Volume 6 Issue 1 Jan - Mar 2015Document5 pagesOriginal Article: National Journal of Community Medicine Volume 6 Issue 1 Jan - Mar 2015Anonymous tlIQeKLriNo ratings yet
- Good Outcome of Teenage Pregnancies in High-Quality Maternity CareDocument5 pagesGood Outcome of Teenage Pregnancies in High-Quality Maternity CareNabila MomorNo ratings yet
- Relevant Obstetric Factors Associated With Fetal Heart Rate Monitoring For Cerebral Palsy in Pregnant Women With Hypertensive Disorder of PregnancyDocument8 pagesRelevant Obstetric Factors Associated With Fetal Heart Rate Monitoring For Cerebral Palsy in Pregnant Women With Hypertensive Disorder of PregnancyDwi PurwantiNo ratings yet
- Perinatalni I Prenatalni Uzroci AutizmaDocument8 pagesPerinatalni I Prenatalni Uzroci AutizmaJohn SmithNo ratings yet
- Nelson, 1978Document10 pagesNelson, 1978Arisa RosyadaNo ratings yet
- Knowledge Level and Determinants of Neonatal Jaundice A Cross-Sectional Study in The Effutu Municipality of GhanaDocument10 pagesKnowledge Level and Determinants of Neonatal Jaundice A Cross-Sectional Study in The Effutu Municipality of GhananicloverNo ratings yet
- Recurrent Hypertensive Disease Associated With Increased Long-Term Mortality RisksDocument6 pagesRecurrent Hypertensive Disease Associated With Increased Long-Term Mortality RisksNandina Rosa FloridanaNo ratings yet
- CTG UnpredictDocument6 pagesCTG UnpredictddcringNo ratings yet
- Pediatrics 2014Document14 pagesPediatrics 2014Randy PrayogoNo ratings yet
- A Meta-Analysis of Depression During Pregnancy and The Risk of Preterm Birth, Low Birth Weight, and Intrauterine Growth RestrictionDocument13 pagesA Meta-Analysis of Depression During Pregnancy and The Risk of Preterm Birth, Low Birth Weight, and Intrauterine Growth RestrictionLaurentiu CiobanuNo ratings yet
- Risk of Cerebral Palsy in Relation To Pregnancy Disorders and Preterm Birth: A National Cohort StudyDocument7 pagesRisk of Cerebral Palsy in Relation To Pregnancy Disorders and Preterm Birth: A National Cohort StudyFarin MauliaNo ratings yet
- Trends in Cerebral Palsy Among Moderately Preterm and Low Birthweight InfantsDocument7 pagesTrends in Cerebral Palsy Among Moderately Preterm and Low Birthweight InfantsЯковлев АлександрNo ratings yet
- Contribution of SES On The PrevalenceDocument9 pagesContribution of SES On The PrevalenceЯковлев АлександрNo ratings yet
- CP A Review of Epidemiological TrendsDocument12 pagesCP A Review of Epidemiological TrendsЯковлев АлександрNo ratings yet
- CP Among Children Born After in Vitro FertilizationDocument10 pagesCP Among Children Born After in Vitro FertilizationЯковлев АлександрNo ratings yet
- Cerebral Palsy Among Children Born During Dublin Randomised TrialDocument4 pagesCerebral Palsy Among Children Born During Dublin Randomised TrialЯковлев АлександрNo ratings yet
- CP A Reconceptualization of The SpectrumDocument5 pagesCP A Reconceptualization of The SpectrumЯковлев АлександрNo ratings yet
- Comparison of Children Diagnosed With Cerebral PalsyDocument8 pagesComparison of Children Diagnosed With Cerebral PalsyЯковлев АлександрNo ratings yet
- Cohort Profile CP in The Norwegian and DanishDocument5 pagesCohort Profile CP in The Norwegian and DanishЯковлев АлександрNo ratings yet
- Coping Potential and DisabilityDocument8 pagesCoping Potential and DisabilityЯковлев АлександрNo ratings yet
- Children With CP SeverityDocument9 pagesChildren With CP SeverityЯковлев АлександрNo ratings yet
- Clinical Spectrum, Comorbidities, and Risk FactorDocument4 pagesClinical Spectrum, Comorbidities, and Risk FactorЯковлев АлександрNo ratings yet
- Contribution of SES On The PrevalenceDocument9 pagesContribution of SES On The PrevalenceЯковлев АлександрNo ratings yet
- Cerebral Palsy Registries: Christine Cans, Geraldine Surman, Vicki Mcmanus, David Coghlan, Owen Hensey, and Ann JohnsonDocument6 pagesCerebral Palsy Registries: Christine Cans, Geraldine Surman, Vicki Mcmanus, David Coghlan, Owen Hensey, and Ann JohnsonЯковлев АлександрNo ratings yet
- Comparing CP Surveillance DefinitionDocument2 pagesComparing CP Surveillance DefinitionЯковлев АлександрNo ratings yet
- Children With CP Racial DisparitiesDocument10 pagesChildren With CP Racial DisparitiesЯковлев АлександрNo ratings yet
- Children With Motor Impairment Related To CPDocument5 pagesChildren With Motor Impairment Related To CPЯковлев АлександрNo ratings yet
- Comparison of Children Diagnosed With Cerebral PalsyDocument8 pagesComparison of Children Diagnosed With Cerebral PalsyЯковлев АлександрNo ratings yet
- Changing Views of Cerebral Palsy Over 35 YearsDocument8 pagesChanging Views of Cerebral Palsy Over 35 YearsЯковлев АлександрNo ratings yet
- Clinical Spectrum of CPDocument5 pagesClinical Spectrum of CPЯковлев АлександрNo ratings yet
- Clinical Spectrum of CP in North IndiaDocument5 pagesClinical Spectrum of CP in North IndiaЯковлев АлександрNo ratings yet
- Children With IntellectualDocument8 pagesChildren With IntellectualЯковлев АлександрNo ratings yet
- Clinical Presentation, Associated Disorders and Aetiological Moments in CPDocument7 pagesClinical Presentation, Associated Disorders and Aetiological Moments in CPЯковлев АлександрNo ratings yet
- Classification of Topographical PatternDocument7 pagesClassification of Topographical PatternЯковлев АлександрNo ratings yet
- Changing Panorama of CerebralDocument7 pagesChanging Panorama of CerebralЯковлев АлександрNo ratings yet
- Changing Views of Cerebral Palsy Over 35 YearsDocument8 pagesChanging Views of Cerebral Palsy Over 35 YearsЯковлев АлександрNo ratings yet
- Clinical Presentation, Associated Disorders and Aetiological Moments in CPDocument7 pagesClinical Presentation, Associated Disorders and Aetiological Moments in CPЯковлев АлександрNo ratings yet
- Children With CP SeverityDocument9 pagesChildren With CP SeverityЯковлев АлександрNo ratings yet
- Changing Pattern of CP in The Southwest Region of FinlandDocument7 pagesChanging Pattern of CP in The Southwest Region of FinlandЯковлев АлександрNo ratings yet
- Changing Pattern of CP in The Southwest Region of FinlandDocument7 pagesChanging Pattern of CP in The Southwest Region of FinlandЯковлев АлександрNo ratings yet
- Cerebral Palsy in Eastern DenmarkDocument5 pagesCerebral Palsy in Eastern DenmarkЯковлев АлександрNo ratings yet
- Blackmer Pump Parts ListDocument2 pagesBlackmer Pump Parts ListFelipe Ignacio PaillavilNo ratings yet
- ZTE UMTS KPI Optimization Analysis Guide V1 1 1Document62 pagesZTE UMTS KPI Optimization Analysis Guide V1 1 1GetitoutLetitgo100% (1)
- Entrepreneurship Macro Environment ForcesDocument26 pagesEntrepreneurship Macro Environment ForcesSivaNo ratings yet
- What Is A Supply ChainDocument20 pagesWhat Is A Supply ChainThanh Binh Tran NguyenNo ratings yet
- The Following Functional Health Pattern Assessment Is Based On A 65 Year Old Scottish Woman Who Lives Independently With Her Husband in Their Home at Happy ValleyDocument9 pagesThe Following Functional Health Pattern Assessment Is Based On A 65 Year Old Scottish Woman Who Lives Independently With Her Husband in Their Home at Happy ValleyJajangNo ratings yet
- Bronchiolitis A Practical Approach For The General RadiologistDocument42 pagesBronchiolitis A Practical Approach For The General RadiologistTara NareswariNo ratings yet
- English HL Grade 8 Language Exam Nov 2017 MEMODocument12 pagesEnglish HL Grade 8 Language Exam Nov 2017 MEMOThegn's PicklesNo ratings yet
- PTC Document Status: (Updated 11 November 2015)Document5 pagesPTC Document Status: (Updated 11 November 2015)AndersonGabriel23No ratings yet
- 05.G. Before Takeoff CheckDocument4 pages05.G. Before Takeoff CheckUDAYAPRAKASH RANGASAMYNo ratings yet
- Mechanical Design of Turine EginesDocument51 pagesMechanical Design of Turine EginessriniNo ratings yet
- Anatomy of A Plated HoleDocument5 pagesAnatomy of A Plated Holepbs0707No ratings yet
- Buckling TestDocument11 pagesBuckling Testsharusli100% (1)
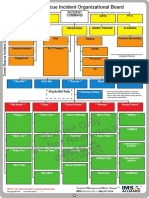
- Sample Only Do Not Reproduce: Trench Rescue Incident Organizational BoardDocument1 pageSample Only Do Not Reproduce: Trench Rescue Incident Organizational BoardLuis Diaz CerdanNo ratings yet
- Chapter 3Document58 pagesChapter 3hasanNo ratings yet
- Fitness RX For Women - December 2013Document124 pagesFitness RX For Women - December 2013renrmrm100% (2)
- Algebra 1 FINAL EXAM REVIEW 2Document2 pagesAlgebra 1 FINAL EXAM REVIEW 2Makala DarwoodNo ratings yet
- Make A Selection: Choose An Alloy and Correlating Casting ProcessDocument5 pagesMake A Selection: Choose An Alloy and Correlating Casting ProcessSarath ChandraNo ratings yet
- Material ManagementDocument106 pagesMaterial ManagementRomi AfriansyahNo ratings yet
- Biologic License ApplicationDocument16 pagesBiologic License ApplicationJean Sandra PintoNo ratings yet
- Ex 2013 1 (Recurrent)Document30 pagesEx 2013 1 (Recurrent)alh basharNo ratings yet
- Water Spray Nozzle: Fire Fighting Equipment Data SheetDocument7 pagesWater Spray Nozzle: Fire Fighting Equipment Data SheetJosef MadronaNo ratings yet
- PR900 Operator ManualDocument21 pagesPR900 Operator ManualAlan TanNo ratings yet
- Engineering Statics FundamentalsDocument28 pagesEngineering Statics FundamentalsurwaNo ratings yet
- Nursing TheoriesDocument9 pagesNursing TheoriesMichelleneChenTadleNo ratings yet
- Platelets & Blood Clotting: The Hemostasis ProcessDocument34 pagesPlatelets & Blood Clotting: The Hemostasis ProcesssamayaNo ratings yet
- Monthly Fire Extinguisher Inspection ChecklistDocument2 pagesMonthly Fire Extinguisher Inspection ChecklistisaacbombayNo ratings yet
- Assignment 12Document7 pagesAssignment 12Anonymous mqIqN5zNo ratings yet
- Definisi, Karakteristik dan Contoh Aplikasi SIGDocument28 pagesDefinisi, Karakteristik dan Contoh Aplikasi SIGtoyota taaNo ratings yet
- Estimating Hb Levels with Sahli's MethodDocument13 pagesEstimating Hb Levels with Sahli's MethodSANANo ratings yet
- Juxtaposition and Non Motion Varese BridDocument13 pagesJuxtaposition and Non Motion Varese BridIvan Eiji Yamauchi SimurraNo ratings yet