You might also like
- SupplementStack PDFDocument19 pagesSupplementStack PDFbungureanu_6100% (1)
- Contractor Safety ManualDocument145 pagesContractor Safety Manualdaladar2008No ratings yet
- Abnormal Psychology Beidel 3rd Edition Test BankDocument4 pagesAbnormal Psychology Beidel 3rd Edition Test BankChuck Simmons100% (25)
- Medical Malpractice and Compensation in The UKDocument33 pagesMedical Malpractice and Compensation in The UKgun rayNo ratings yet
- The Family Doctor - Prof. Henry S Taylor, M.D., 1860Document324 pagesThe Family Doctor - Prof. Henry S Taylor, M.D., 1860IreneRainsNo ratings yet
- Health Care Regulation in Low-And Middle-Income Countries: A Literature ReviewDocument20 pagesHealth Care Regulation in Low-And Middle-Income Countries: A Literature ReviewNossal Institute for Global HealthNo ratings yet
- Summary of Key Points from 2010 NHS White PaperDocument5 pagesSummary of Key Points from 2010 NHS White Paperdub2746No ratings yet
- Make Decisions: NPA Discussion - NHS White Paper. 28 Jul 2010Document4 pagesMake Decisions: NPA Discussion - NHS White Paper. 28 Jul 2010Idrees MohammedNo ratings yet
- UK AND US HEALTHCARE COMPARISON - EditedDocument19 pagesUK AND US HEALTHCARE COMPARISON - EditedAbiola Abraham100% (1)
- The Future of Positive Psychology: A Declaration of IndependenceDocument17 pagesThe Future of Positive Psychology: A Declaration of IndependenceEbonnie DiazNo ratings yet
- The Henry Fords of Healthcar: Lessons the West Can Learn from the EastFrom EverandThe Henry Fords of Healthcar: Lessons the West Can Learn from the EastNo ratings yet
- A Critical Insight, Analysis and Comparative of Health Care Provision in The United Kingdom and United States of America.Document19 pagesA Critical Insight, Analysis and Comparative of Health Care Provision in The United Kingdom and United States of America.Abiola AbrahamNo ratings yet
- Reforming The Swedish Health Services - The International Context.Document13 pagesReforming The Swedish Health Services - The International Context.Junca VictorNo ratings yet
- Sector Career Research and Opportunity AwarenessDocument12 pagesSector Career Research and Opportunity AwarenessjacintaNo ratings yet
- Mmw@liverpool Ac UkDocument12 pagesMmw@liverpool Ac Ukapi-48772628No ratings yet
- Please Circulate This Document As A Whole or As Individual Questions To Everyone You Can in This Country, and Ask The Recipients To Do The SameDocument7 pagesPlease Circulate This Document As A Whole or As Individual Questions To Everyone You Can in This Country, and Ask The Recipients To Do The Sameapi-120831962No ratings yet
- Medicina Basada en La EvidenciaDocument6 pagesMedicina Basada en La EvidenciaJulivaiNo ratings yet
- Unite Guide To: Privatisation of The NHS EnglandDocument24 pagesUnite Guide To: Privatisation of The NHS EnglandKarishma MartiniNo ratings yet
- NHS Change Management(1)Document20 pagesNHS Change Management(1)Mary NjeriNo ratings yet
- Economies of HealthDocument17 pagesEconomies of HealthHina Mecarther GillNo ratings yet
- NHS Act Overview: Clinicians Lead CommissioningDocument2 pagesNHS Act Overview: Clinicians Lead CommissioningMohammad Tayyab KhanNo ratings yet
- National Health ServiceDocument24 pagesNational Health Servicevictor oliverNo ratings yet
- MOMD EssayDocument4 pagesMOMD EssayKachy Kayman AkamnonuNo ratings yet
- C. Mjaset - Value-Based Health Care in Four Different Health Care SystemsDocument23 pagesC. Mjaset - Value-Based Health Care in Four Different Health Care SystemsRodney RosaliaNo ratings yet
- Managing Change - The NHS Scotland Case Stdy by ..... 2Document7 pagesManaging Change - The NHS Scotland Case Stdy by ..... 2njimbongstelian4No ratings yet
- Implementing Operations Strategy Through Lean Processes Within Health CareDocument35 pagesImplementing Operations Strategy Through Lean Processes Within Health CareNatala WillzNo ratings yet
- Public Private HealthDocument41 pagesPublic Private HealthSreetama007No ratings yet
- Discussion Paper 1: Enshrining The Ability To Work in The New NHS, Steve BoormanDocument9 pagesDiscussion Paper 1: Enshrining The Ability To Work in The New NHS, Steve BoormanFitForWorkUKNo ratings yet
- Role of Govenrment in Healthcare MarketsDocument9 pagesRole of Govenrment in Healthcare Marketsshandil7No ratings yet
- Do doctors respond to financial incentivesDocument24 pagesDo doctors respond to financial incentivesvarian90No ratings yet
- MOH Vision and StrategyDocument8 pagesMOH Vision and StrategyJohn MutukuNo ratings yet
- MOH Vision and StrategyDocument8 pagesMOH Vision and StrategyJohn MutukuNo ratings yet
- CHE Research Paper 64: Do Hospitals Respond To Greater Autonomy? Evidence From The English NHSDocument32 pagesCHE Research Paper 64: Do Hospitals Respond To Greater Autonomy? Evidence From The English NHSSonam WangdusNo ratings yet
- Paula Anglia Ruskin-ARU-HEDocument19 pagesPaula Anglia Ruskin-ARU-HERoki Hassan0% (1)
- Afforable Care Act FinalDocument64 pagesAfforable Care Act FinalArafat MazharNo ratings yet
- The National Health Service (Primary Care) Bill (HL) : Research Paper 97/16 5 February 1997Document45 pagesThe National Health Service (Primary Care) Bill (HL) : Research Paper 97/16 5 February 1997qqztagNo ratings yet
- Lippincott Williams & WilkinsDocument13 pagesLippincott Williams & WilkinscaptainfreakoutNo ratings yet
- The Market in Primary CareDocument4 pagesThe Market in Primary CareAnonymous 3PrQCoMNo ratings yet
- Uk Public Service Gates FoundatgonDocument40 pagesUk Public Service Gates Foundatgoneastwind_gNo ratings yet
- Health InsuranceDocument32 pagesHealth InsuranceAshwini DongreNo ratings yet
- AHA BundledPayment ReportDocument20 pagesAHA BundledPayment Reportbikram2128100% (1)
- Economics in SocietyDocument4 pagesEconomics in Societyscorpio786No ratings yet
- The 2011 Proposal For Universal Health Insurance in IrelandDocument7 pagesThe 2011 Proposal For Universal Health Insurance in IrelandIbrahim DoruNo ratings yet
- BMA Briefing on Lords Committee Stage of Health and Social Care BillDocument6 pagesBMA Briefing on Lords Committee Stage of Health and Social Care Billjoke1874No ratings yet
- 2017 Austeridade Portugal Servicos SaudeDocument12 pages2017 Austeridade Portugal Servicos SaudeluistbfNo ratings yet
- Ramos, Sioco Chapter 25 and 26Document59 pagesRamos, Sioco Chapter 25 and 26DOROTHY ANN SOMBILUNANo ratings yet
- AccidentalLean ReflectionsonOperationsStrategyDocument29 pagesAccidentalLean ReflectionsonOperationsStrategyRasika ATHUKORALANo ratings yet
- Curing Australia's Health Care System: Reform by Joshua Gans and Stephen KingDocument27 pagesCuring Australia's Health Care System: Reform by Joshua Gans and Stephen KingCore ResearchNo ratings yet
- 05 20 Jane LewisDocument34 pages05 20 Jane LewisPrince G.No ratings yet
- Australia and New Zealand Health PolicyDocument9 pagesAustralia and New Zealand Health PolicyElena JilavuNo ratings yet
- Answer 1Document8 pagesAnswer 1Hezekiah AtindaNo ratings yet
- Witness Testimony Benedic Ippolito HE Hearing 03.28.23Document17 pagesWitness Testimony Benedic Ippolito HE Hearing 03.28.23petersu11No ratings yet
- UK Country Profile 2008Document3 pagesUK Country Profile 2008albajcNo ratings yet
- The Marketing Challenges of Healthcare Enterpreeurship An Emperical Invesigation in NigeriaDocument17 pagesThe Marketing Challenges of Healthcare Enterpreeurship An Emperical Invesigation in NigeriaHumming BirdNo ratings yet
- Chalkley Governmet Purchase HealthDocument44 pagesChalkley Governmet Purchase Healthnecroteck1No ratings yet
- Integrated Health and Social Care in England - ProgressDocument4 pagesIntegrated Health and Social Care in England - ProgressAntonelle BeharryNo ratings yet
- Conflicting Institutional Logics: A National Programme For IT in The Organisational Field of HealthcareDocument21 pagesConflicting Institutional Logics: A National Programme For IT in The Organisational Field of HealthcareSharon Rose CalabrosoNo ratings yet
- Financ Acc Manag - 2017 - Gebreiter - Accounting and The Emergence of Care Pathways in The National Health ServiceDocument12 pagesFinanc Acc Manag - 2017 - Gebreiter - Accounting and The Emergence of Care Pathways in The National Health ServiceKimSeokJin StanNo ratings yet
- The Use of Evidence in English Local Public Health Decision-Making: A Systematic Scoping ReviewDocument12 pagesThe Use of Evidence in English Local Public Health Decision-Making: A Systematic Scoping ReviewatouyaNo ratings yet
- A Sustainable Health System IIDocument73 pagesA Sustainable Health System IICírculo de EmpresariosNo ratings yet
- The Impact of Clinical Services Provided by Community Pharmacies On The Australian Healthcare System A Review of The Literature Journal of PharmaceutDocument42 pagesThe Impact of Clinical Services Provided by Community Pharmacies On The Australian Healthcare System A Review of The Literature Journal of PharmaceutBIANCA KARLA LICATANNo ratings yet
- Adoption and Spread of Innovation in The NHS: This Content Relates To The Following TopicsDocument4 pagesAdoption and Spread of Innovation in The NHS: This Content Relates To The Following Topicszeze_13No ratings yet
- Economic CommentaryDocument83 pagesEconomic Commentarystingo21No ratings yet
- SSRN Id3795336Document33 pagesSSRN Id3795336Med MedNo ratings yet
- Partnership and Accountability in The Era of Integrated Care: A Tale From EnglandDocument3 pagesPartnership and Accountability in The Era of Integrated Care: A Tale From EnglandAjideniNo ratings yet
- JAJ TestimoniesDocument2 pagesJAJ TestimoniesErdem Ğ. ÇalışkanNo ratings yet
- Ectopic PregnancyDocument54 pagesEctopic Pregnancypatriciaatan1497No ratings yet
- Birth asphyxia causes and neonatal resuscitationDocument20 pagesBirth asphyxia causes and neonatal resuscitationinne_fNo ratings yet
- They Are All MadDocument100 pagesThey Are All Madcraig1014No ratings yet
- Qol SonDocument3 pagesQol Sonpermana0adityaNo ratings yet
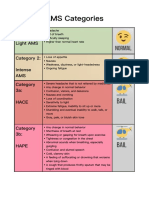
- AMS Symptoms and CategoriesDocument1 pageAMS Symptoms and CategoriesyyggvcNo ratings yet
- Caitlin Mariscal - Career Exploration WorksheetDocument2 pagesCaitlin Mariscal - Career Exploration Worksheetapi-389735946No ratings yet
- How to Get a Good Night's Sleep: Tips for Managing InsomniaDocument24 pagesHow to Get a Good Night's Sleep: Tips for Managing InsomniaUm ArNo ratings yet
- CA 125II: Assay SummaryDocument14 pagesCA 125II: Assay SummaryThế TuyềnNo ratings yet
- Interstitial Diffuse Lung Disease Patient QuestionnaireDocument4 pagesInterstitial Diffuse Lung Disease Patient QuestionnaireJamban08No ratings yet
- Prevention of Surgical Site Infections: Pola Brenner, Patricio NercellesDocument10 pagesPrevention of Surgical Site Infections: Pola Brenner, Patricio NercellesAmeng GosimNo ratings yet
- Shih Tzus: What A Unique Breed!Document5 pagesShih Tzus: What A Unique Breed!Jimmy YauNo ratings yet
- NCP BathingDocument3 pagesNCP BathingNICOLE TOLENTINONo ratings yet
- Mefenamic Acid Drug StudyDocument1 pageMefenamic Acid Drug StudyAj GoNo ratings yet
- Resume For KidDocument5 pagesResume For Kidnjoqvnjbf100% (2)
- 265 23686 1 10 20190515 PDFDocument10 pages265 23686 1 10 20190515 PDFanggiliaNo ratings yet
- Nursing Interventions for Fracture CareDocument2 pagesNursing Interventions for Fracture CareShekinah DomingoNo ratings yet
- Parasitology SummaryDocument7 pagesParasitology Summaryshiner99100% (1)
- Health and Skill Related Components of Physical FitnessDocument6 pagesHealth and Skill Related Components of Physical FitnessJovanne CabaluNo ratings yet
- 22 CR Protean NeurologicalDocument2 pages22 CR Protean NeurologicalCamii CvNo ratings yet
- Implementasi SPM Kesehatan Bayi Baru Lahir di Puskesmas DukuhsetiDocument10 pagesImplementasi SPM Kesehatan Bayi Baru Lahir di Puskesmas DukuhsetiFidia sariNo ratings yet
- LabaidDocument29 pagesLabaidBorhan UddinNo ratings yet
- 9966 Cons enDocument225 pages9966 Cons enOmz DonNo ratings yet
- ASTMDocument4 pagesASTMdeepsingh2304No ratings yet
- Mental Health EssayDocument2 pagesMental Health EssayROHITNo ratings yet