You might also like
- Trauma and Human Existence PDFDocument76 pagesTrauma and Human Existence PDFMónica Garza100% (3)
- Dysarthria Assessment and TreatmentDocument6 pagesDysarthria Assessment and Treatmentapi-3705274100% (4)
- Infection, Silicosis, Diabetes Mellitus, Chronic Renal Insufficiency, Malignancy, Malnutrition, and Other Forms of EtanerceptDocument4 pagesInfection, Silicosis, Diabetes Mellitus, Chronic Renal Insufficiency, Malignancy, Malnutrition, and Other Forms of EtanerceptyoshiNo ratings yet
- Risk Factor PneumoniaDocument6 pagesRisk Factor Pneumoniaali subchanNo ratings yet
- ROJOSON-PEP-TALK: Home Management of COVID19 Patient (May 22, 2021)Document45 pagesROJOSON-PEP-TALK: Home Management of COVID19 Patient (May 22, 2021)rojosonNo ratings yet
- UtiDocument28 pagesUtiDrShweta SainiNo ratings yet
- Pediatric Urinary Tract Infection: Practice EssentialsDocument14 pagesPediatric Urinary Tract Infection: Practice EssentialsPutu Arimarta Irianta HerosNo ratings yet
- 05.infeksi TuberkulosisDocument46 pages05.infeksi TuberkulosisIntan PermatasariNo ratings yet
- TonsillitisDocument6 pagesTonsillitisAngelica BernalesNo ratings yet
- Management of Adult PUI With ILI 30042013-1Document3 pagesManagement of Adult PUI With ILI 30042013-1Rudzahan RamliNo ratings yet
- Coursera ABSDocument8 pagesCoursera ABSevanoNo ratings yet
- Group 2 - Renal CSDocument49 pagesGroup 2 - Renal CSStephany Dela CruzNo ratings yet
- Poster CHIKV DENV Comparison Healthcare Providers PDFDocument2 pagesPoster CHIKV DENV Comparison Healthcare Providers PDFJawad HaiderNo ratings yet
- Anti Tubercular AgentsDocument22 pagesAnti Tubercular AgentsKakai Ablanque LopozNo ratings yet
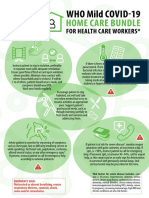
- WHO COVID-19-Home-Care-BundleDocument2 pagesWHO COVID-19-Home-Care-BundleOCSAF - P2LT PUNSALAN MCNo ratings yet
- Perioperative Care of A Pediatric Surgical PatientDocument60 pagesPerioperative Care of A Pediatric Surgical Patienthabtsh habshaNo ratings yet
- Acute Pyelonephritis AdultDocument1 pageAcute Pyelonephritis AdultMeagan SotoNo ratings yet
- Acute PyelonephritisDocument9 pagesAcute Pyelonephritistaekado-1No ratings yet
- Chronic Obstructive Pulmonary Disease Acute Exacerbation Antimicrobial Prescribing PDF 66141598418629Document28 pagesChronic Obstructive Pulmonary Disease Acute Exacerbation Antimicrobial Prescribing PDF 66141598418629NoahNo ratings yet
- PSM Supplement by DR Vivek JainDocument5 pagesPSM Supplement by DR Vivek JainVivek Jain100% (14)
- Neumonia y Bronquiolitis 22Document14 pagesNeumonia y Bronquiolitis 22Rafael Florez HernandezNo ratings yet
- CSS DHFDocument40 pagesCSS DHFDina SofianaNo ratings yet
- TyphoidDocument3 pagesTyphoidunagraciaNo ratings yet
- Uti CPG 2Document36 pagesUti CPG 2Yohan VeissmanNo ratings yet
- CCO COVID19 Resources Center Treatment Downloadable 1Document185 pagesCCO COVID19 Resources Center Treatment Downloadable 1YoshimuneNo ratings yet
- Referral Guide Lines For Patient With HeadacheDocument13 pagesReferral Guide Lines For Patient With HeadacheImad Q. KhaleelNo ratings yet
- UTI GuidelineDocument10 pagesUTI Guidelinecatalin petreNo ratings yet
- Acute Exacerbation of AsthmaDocument28 pagesAcute Exacerbation of AsthmaMike singhNo ratings yet
- Anesthesia Services For Gastrointestinal Endoscopic ProceduresDocument6 pagesAnesthesia Services For Gastrointestinal Endoscopic ProceduresHidayati IdaNo ratings yet
- Infections in The Elderly: Jérôme Fennell, Jerome - Fennell@amnch - IeDocument71 pagesInfections in The Elderly: Jérôme Fennell, Jerome - Fennell@amnch - IeA G I T ONo ratings yet
- PGuidelines Enteric. FeverDocument4 pagesPGuidelines Enteric. FeverSara Ilyas KhanNo ratings yet
- Whooping Cough: Dr. MwendwaDocument39 pagesWhooping Cough: Dr. MwendwaAlvin OmondiNo ratings yet
- Pediatric Urinary Tract InfectionDocument29 pagesPediatric Urinary Tract InfectionFenty IswarNo ratings yet
- Bangladesh National Guidelines and Operational Manual For Tuberculosis ControlDocument48 pagesBangladesh National Guidelines and Operational Manual For Tuberculosis ControlAshraf Uddin AhmedNo ratings yet
- TB Case Finding (Slide)Document15 pagesTB Case Finding (Slide)Emman Acosta DomingcilNo ratings yet
- Acute Asthma Paed WaniDocument16 pagesAcute Asthma Paed WaniNurul Syazwani RamliNo ratings yet
- UTI Treatment Algorithm - Sharp Mesa Vista 2Document3 pagesUTI Treatment Algorithm - Sharp Mesa Vista 2Fitri 1997No ratings yet
- 853 PDFDocument122 pages853 PDFTammy StephanieNo ratings yet
- Guillain Barre SyndromeDocument49 pagesGuillain Barre SyndromeDavid SugiartoNo ratings yet
- Day 2 Panel UTI - Saniel Abu MarianoDocument66 pagesDay 2 Panel UTI - Saniel Abu MarianoRye CalderonNo ratings yet
- Clinical Management Protocol PDFDocument7 pagesClinical Management Protocol PDFAJEET KUMAR PANDEYNo ratings yet
- Paediatric Infections in Neutropenic EpisodesDocument20 pagesPaediatric Infections in Neutropenic EpisodesjellyjohnNo ratings yet
- Typhoid Fever: by DR .. Magdi Elbaloola Ahmed Physcian & GastrohepatologistDocument25 pagesTyphoid Fever: by DR .. Magdi Elbaloola Ahmed Physcian & GastrohepatologistÅbübâkêř Äbd-ëřhēēm BãřřîNo ratings yet
- Acute Glomerulonephritis 1Document19 pagesAcute Glomerulonephritis 1Jane Ann AlolodNo ratings yet
- Acute Otitis Media Management Guideline-1 - 1Document4 pagesAcute Otitis Media Management Guideline-1 - 1Melly Syafrida PutriNo ratings yet
- Pneumonia: Recent Evidence Based UpdatesDocument30 pagesPneumonia: Recent Evidence Based UpdatesAli AzamNo ratings yet
- Kawasaki DiseaseDocument22 pagesKawasaki DiseaseGemma FUERTESNo ratings yet
- Criterii de Trimitere ImunologieDocument7 pagesCriterii de Trimitere ImunologieRoxana HuțanuNo ratings yet
- Tuberculosis: Angeles University FoundationDocument10 pagesTuberculosis: Angeles University FoundationBob Joyce Dela PeñaNo ratings yet
- Typhoid Fever DR Moses KazevuDocument12 pagesTyphoid Fever DR Moses KazevuMoses Jr KazevuNo ratings yet
- EJMCM - Volume 8 - Issue 3Document12 pagesEJMCM - Volume 8 - Issue 3Grahita Y. AprihatinoNo ratings yet
- Paediatric CAP Appendix 4Document22 pagesPaediatric CAP Appendix 4Dr. TomNo ratings yet
- 2009-10-16 Current Antiviral Recommendations For Influenza TreatmentDocument2 pages2009-10-16 Current Antiviral Recommendations For Influenza Treatmenttamiprior5294No ratings yet
- Brajac - ProtocolDocument13 pagesBrajac - Protocolthanh ngôNo ratings yet
- Antivirals Patient FlyerDocument1 pageAntivirals Patient Flyermortxyt7No ratings yet
- Case Study UrtiDocument9 pagesCase Study UrtiHomework PingNo ratings yet
- Pediatric Case Sheet: IdentificationDocument10 pagesPediatric Case Sheet: Identificationabnamariq17No ratings yet
- Standard Treatment Guidelines On Acute SinusitisDocument27 pagesStandard Treatment Guidelines On Acute SinusitisnikeNo ratings yet
- TuberculosisDocument19 pagesTuberculosisdipendrakumarkushawaha44No ratings yet
- ZegenDocument9 pagesZegenJefferson ManasanNo ratings yet
- Treatment of Pulmonary and Extra-Pulmonary Tuberculosis in AdultsDocument65 pagesTreatment of Pulmonary and Extra-Pulmonary Tuberculosis in AdultsLloyd Daniel BarrantesNo ratings yet
- Alcohol Cetoestearilico MsdsDocument6 pagesAlcohol Cetoestearilico MsdsJoha Darwin ChNo ratings yet
- Digestive System Lesson PlanDocument6 pagesDigestive System Lesson PlanRosselle May JumayaoNo ratings yet
- Teenagers Eating HabitsDocument3 pagesTeenagers Eating HabitsMaria Jose Sanz0% (1)
- Handbook of Children With Special Health Care NeedsDocument443 pagesHandbook of Children With Special Health Care Needsحسين منصورNo ratings yet
- Home Care in ElderlyDocument18 pagesHome Care in ElderlyshodhgangaNo ratings yet
- PPS Bab 7Document44 pagesPPS Bab 7EgieAprianNo ratings yet
- The Flaw of Averages in Flattening The CurveDocument7 pagesThe Flaw of Averages in Flattening The CurveFahad IzharNo ratings yet
- Reliance Health Claim FormDocument4 pagesReliance Health Claim FormarijitnirmalNo ratings yet
- Form 10: (See Rule 19 (1) )Document2 pagesForm 10: (See Rule 19 (1) )ommetalomNo ratings yet
- Common Nail Diseases and DisordersDocument19 pagesCommon Nail Diseases and DisordersAijeleth Shahar Gunay AwacayNo ratings yet
- AneurysmDocument22 pagesAneurysmRaymond SorianoNo ratings yet
- Alexander Technique EssayDocument2 pagesAlexander Technique EssayMathematicus MathematicaNo ratings yet
- Lab Emergency ProcedureDocument16 pagesLab Emergency ProcedureFre HanyaqNo ratings yet
- Natco 2016 PDFDocument101 pagesNatco 2016 PDFSagar BhardwajNo ratings yet
- 2018 Global Consensus Guidelines For The Injection of Diluted and Hyperdiluted Calcium Hydroxylapatite For Skin TighteningDocument10 pages2018 Global Consensus Guidelines For The Injection of Diluted and Hyperdiluted Calcium Hydroxylapatite For Skin Tighteningletty3gapeNo ratings yet
- Safety Norms in Construction SiteDocument13 pagesSafety Norms in Construction Sitesantoshspav100% (1)
- Css 2015 Selected ListDocument24 pagesCss 2015 Selected ListSrinivas ChintuNo ratings yet
- Materi Policy Analysis TriangleDocument6 pagesMateri Policy Analysis TriangleRegina Marsha100% (1)
- Quick Reference GuideDocument2 pagesQuick Reference Guideapi-56341082No ratings yet
- April BaseDocument3 pagesApril BaseDinesh Chandramohan CNo ratings yet
- Development and Maintenance of Standards and Accreditation ofDocument6 pagesDevelopment and Maintenance of Standards and Accreditation ofsrimalathiNo ratings yet
- Vibrio & Aeromonas & PlesiomonasDocument48 pagesVibrio & Aeromonas & PlesiomonasOscar PeñaNo ratings yet
- Study - COMPETENCES - UDL, Gifted C, ADHD, Autism, Etc..Document10 pagesStudy - COMPETENCES - UDL, Gifted C, ADHD, Autism, Etc..angela castroNo ratings yet
- M2LP3 - Gender Based ViolenceDocument98 pagesM2LP3 - Gender Based ViolenceLuz LabeniaNo ratings yet
- Skull RadiographyDocument12 pagesSkull RadiographyMohamed AufNo ratings yet
- Biesalski - Hidden HungerDocument265 pagesBiesalski - Hidden HungerEnzo Ubaque AhumadaNo ratings yet
- Recreatinal SlidesDocument28 pagesRecreatinal Slidesnerlyn100% (1)
- Chapter 2: Population: The Cultural LandscapeDocument50 pagesChapter 2: Population: The Cultural LandscapeAlan nguyenNo ratings yet