You might also like
- MedTech ReviewersDocument2 pagesMedTech ReviewersGlydenne Glaire Poncardas Gayam100% (1)
- Screenshot 2021-10-27 at 13.19.13Document74 pagesScreenshot 2021-10-27 at 13.19.13Kenny MgulluNo ratings yet
- Value Analysis Guide Vol 5Document56 pagesValue Analysis Guide Vol 5r.benouhoudNo ratings yet
- Khmer Friendship HospitalDocument3 pagesKhmer Friendship Hospitalខៃសិញ- KhaisinhNo ratings yet
- PONCHO TrialDocument8 pagesPONCHO Trialrahul krishnanNo ratings yet
- Stadhouder PDFDocument7 pagesStadhouder PDFPramod N KNo ratings yet
- Jurnal Anestesi "RCT"Document9 pagesJurnal Anestesi "RCT"Feri AprizalNo ratings yet
- Pain Intensity On The First Day After Surgery: A Prospective Cohort Study Comparing 179 Surgical ProceduresDocument11 pagesPain Intensity On The First Day After Surgery: A Prospective Cohort Study Comparing 179 Surgical ProceduresCuenta LastNo ratings yet
- Tonsillar Fossa ClosureDocument7 pagesTonsillar Fossa ClosureChristin LapadjiNo ratings yet
- Lampiran Jurnal CA Mammae Sessler-2019Document9 pagesLampiran Jurnal CA Mammae Sessler-2019Tulus BukhoriNo ratings yet
- AnesDocument8 pagesAnesrachma30No ratings yet
- Obstetrics AnesthesiaDocument31 pagesObstetrics AnesthesiaNorfarhanah ZakariaNo ratings yet
- Pediatric Tonsillectomy PatientsDocument3 pagesPediatric Tonsillectomy PatientsRainer MujicaNo ratings yet
- 2017.multimodal Intrathecal Analgesia in Refractory Cancer PainDocument5 pages2017.multimodal Intrathecal Analgesia in Refractory Cancer Paintidarat.aimNo ratings yet
- e507d2a9-15d1-4ffe-96d4-dccb4188b121Document12 pagese507d2a9-15d1-4ffe-96d4-dccb4188b121Julio AltamiranoNo ratings yet
- Early Use of TIPS in Cirrhosis and Variceal BleedingDocument10 pagesEarly Use of TIPS in Cirrhosis and Variceal Bleedingray liNo ratings yet
- 1 s2.0 S0015028218305685 PDFDocument8 pages1 s2.0 S0015028218305685 PDFYoza FirdaozNo ratings yet
- Control of Endometriosis-Associated Pain With Etonogestrel-Releasing Contraceptive Implant and 52mg Levonogestrel ReleaDocument8 pagesControl of Endometriosis-Associated Pain With Etonogestrel-Releasing Contraceptive Implant and 52mg Levonogestrel ReleaYudhistira AdhiNo ratings yet
- Marty 2018Document6 pagesMarty 2018rihatseravatNo ratings yet
- Priska Febriandini P - Is Inguinal Hernia SafeDocument4 pagesPriska Febriandini P - Is Inguinal Hernia SafeAbraham WilliamNo ratings yet
- Intrathecal Ziconotide in The Treatment of Refractory Pain in Patients With Cancer or AIDSDocument8 pagesIntrathecal Ziconotide in The Treatment of Refractory Pain in Patients With Cancer or AIDSSérgio TavaresNo ratings yet
- Tugas RCT SenaDocument10 pagesTugas RCT SenaArfad El HabibieNo ratings yet
- Bahan KedkelDocument8 pagesBahan KedkelUliza Nur AiniNo ratings yet
- The Impact of Preemptive Perianal Anaesthetic Block in Open Haemorrhoidectomy - A Randomised Controlled TrialDocument3 pagesThe Impact of Preemptive Perianal Anaesthetic Block in Open Haemorrhoidectomy - A Randomised Controlled TrialhrtfdnbzvwNo ratings yet
- TAP Paper PublishedDocument8 pagesTAP Paper PublishedMotaz AbusabaaNo ratings yet
- Analgesia en Apendicitis AgudaDocument3 pagesAnalgesia en Apendicitis Agudasilvia barbosaNo ratings yet
- Journal Medicine: The New EnglandDocument7 pagesJournal Medicine: The New England'Muhamad Rofiq Anwar'No ratings yet
- Acup Utk TonsiltektomiDocument7 pagesAcup Utk Tonsiltektominewanda1112No ratings yet
- Protocol oDocument8 pagesProtocol oCynthia ChávezNo ratings yet
- Thoracic Segmental Spinal Anaesthesia/ General Anaesthesia For Laproscopy SurgeryDocument8 pagesThoracic Segmental Spinal Anaesthesia/ General Anaesthesia For Laproscopy SurgeryIJAR JOURNALNo ratings yet
- 10 - (Rahman) The Relationship Between Chest Tube Size and Clinical Outcome in Pleural InfectionDocument8 pages10 - (Rahman) The Relationship Between Chest Tube Size and Clinical Outcome in Pleural InfectionfaisaldanyaniNo ratings yet
- Tencate Hoek2018Document9 pagesTencate Hoek2018Han's OfficialNo ratings yet
- Effects of propofol versus sevoflurane anesthesia on postoperative pain after gastrectomyDocument33 pagesEffects of propofol versus sevoflurane anesthesia on postoperative pain after gastrectomyJuwita PratiwiNo ratings yet
- 2017 Intercostal Nerve Cryo Vs Thoracic Epidural Cath For Postop Analgesia 26 Cryo PatientsDocument6 pages2017 Intercostal Nerve Cryo Vs Thoracic Epidural Cath For Postop Analgesia 26 Cryo PatientsIevgen DanylchukNo ratings yet
- Repetitive Transcranial Magnetic Stimulation Therapy (RTMS) For Endometriosis Patients With Refractory Pelvic Chronic Pain: A Pilot StudyDocument11 pagesRepetitive Transcranial Magnetic Stimulation Therapy (RTMS) For Endometriosis Patients With Refractory Pelvic Chronic Pain: A Pilot StudyM C B ESPAÇO TERAPÊUTICO LTDA AUTISMO EM GOIÂNIANo ratings yet
- Effect of Epidural Analgesia IDocument14 pagesEffect of Epidural Analgesia IRhandy SeptiantoNo ratings yet
- Rectal Stenosis After Procedures For Prolapse and Hemorrhoids (PPH) - A Report From ChinaDocument5 pagesRectal Stenosis After Procedures For Prolapse and Hemorrhoids (PPH) - A Report From ChinaAmriansyah PranowoNo ratings yet
- Effect of Scrotal Hitching in Reducing Scrotal Edema After Inguinoscrotal Hernia RepairDocument4 pagesEffect of Scrotal Hitching in Reducing Scrotal Edema After Inguinoscrotal Hernia RepairIOSRjournalNo ratings yet
- 2011 JET FedorDocument3 pages2011 JET FedorronnyNo ratings yet
- Bed Angels On PainDocument12 pagesBed Angels On PainNiken AninditaNo ratings yet
- Anes 10Document8 pagesAnes 10Fuchsia ZeinNo ratings yet
- International Journal of Obstetric AnesthesiaDocument6 pagesInternational Journal of Obstetric Anesthesiaanita pratiwiNo ratings yet
- Spinal vs. General Anesthesia For Percutaneous Nephrolithotomy: A Prospective Randomized TrialDocument5 pagesSpinal vs. General Anesthesia For Percutaneous Nephrolithotomy: A Prospective Randomized TrialDella Puspita SariNo ratings yet
- 3Document8 pages3Agung SentosaNo ratings yet
- Anesthesia & ClinicalDocument4 pagesAnesthesia & Clinicalreinhard fourayNo ratings yet
- Kumar S.Document4 pagesKumar S.Van DaoNo ratings yet
- The Scalp Block For Postoperative Pain Control in Craniosynostosis Surgery: A Case Control StudyDocument8 pagesThe Scalp Block For Postoperative Pain Control in Craniosynostosis Surgery: A Case Control StudyTheresa JulietNo ratings yet
- Randomized Clinical Trial of Intraosseous Methylprednisolone Injection For Acute Pulpitis PainDocument6 pagesRandomized Clinical Trial of Intraosseous Methylprednisolone Injection For Acute Pulpitis PainFrançois BronnecNo ratings yet
- Outcomes of Selective Non-Operative Management for Penetrating Splenic InjuryDocument44 pagesOutcomes of Selective Non-Operative Management for Penetrating Splenic Injuryমোহাম্মদ আবীর100% (1)
- Initial Experience Using Incisional Anesthetic Catheter in Abdominal Wall Ambulatory SurgeryDocument6 pagesInitial Experience Using Incisional Anesthetic Catheter in Abdominal Wall Ambulatory SurgeryilhamNo ratings yet
- PIIS014067361261900XDocument10 pagesPIIS014067361261900X呂鍇東No ratings yet
- Ortho - PediaDocument6 pagesOrtho - PediaKayeNo ratings yet
- Effect of Intraoperative Dexmedetomidine On Post-Craniotomy PainDocument9 pagesEffect of Intraoperative Dexmedetomidine On Post-Craniotomy PainIva SantikaNo ratings yet
- El Sayed2006Document1 pageEl Sayed2006yalocim666No ratings yet
- Randomized trial finds depth of anesthesia has no effect on postoperative painDocument6 pagesRandomized trial finds depth of anesthesia has no effect on postoperative painIntan PurnamasariNo ratings yet
- International Journal of Anesthetics and Anesthesiology Ijaa 7 118Document7 pagesInternational Journal of Anesthetics and Anesthesiology Ijaa 7 118Ferdy RahadiyanNo ratings yet
- Práctica 18 - Delirium in Older Patients After Anesthesia (Artículo para La Discusión)Document15 pagesPráctica 18 - Delirium in Older Patients After Anesthesia (Artículo para La Discusión)HENRY MAYKOL PAZ INOCENTENo ratings yet
- Transversus Abdominis Plane Block For Laparoscopic Inguinal Hernia Repair: A Randomized TrialDocument8 pagesTransversus Abdominis Plane Block For Laparoscopic Inguinal Hernia Repair: A Randomized TrialAYŞE GÜLŞAH ATASEVERNo ratings yet
- Is It Safe To Discharge Intussusception Patients After Successful Hydrostatic Reduction?Document5 pagesIs It Safe To Discharge Intussusception Patients After Successful Hydrostatic Reduction?DaGiTrVel'zNo ratings yet
- Comparison of Preventive Analgesia Techniques in Circumcision Cases Dorsal Penile Nerve Block, Caudal Block, or Subcutaneous MorphineDocument7 pagesComparison of Preventive Analgesia Techniques in Circumcision Cases Dorsal Penile Nerve Block, Caudal Block, or Subcutaneous MorphinenatamkpNo ratings yet
- Predictors of Pain Resolution After Varicocelectomy For Painful VaricoceleDocument5 pagesPredictors of Pain Resolution After Varicocelectomy For Painful VaricoceleMuhammad AndilaNo ratings yet
- A Non-Operative Treatment of Perforated Peptic Ulcer: A Prospective Study With 50 CasesDocument4 pagesA Non-Operative Treatment of Perforated Peptic Ulcer: A Prospective Study With 50 CasesSake Cinema21No ratings yet
- Damage Control in Trauma Care: An Evolving Comprehensive Team ApproachFrom EverandDamage Control in Trauma Care: An Evolving Comprehensive Team ApproachJuan DuchesneNo ratings yet
- Postoperative Pain Management in The Era of ERAS - An Overview 2019Document9 pagesPostoperative Pain Management in The Era of ERAS - An Overview 2019valerio.messinaNo ratings yet
- Ketamine Produces Effective and Long-Term Pain Relief in Patients With Complex Regional Pain Syndrome Type 1Document8 pagesKetamine Produces Effective and Long-Term Pain Relief in Patients With Complex Regional Pain Syndrome Type 1valerio.messinaNo ratings yet
- Intrathecal Hydrophilic Opioids For Abdominal SurgeryDocument15 pagesIntrathecal Hydrophilic Opioids For Abdominal Surgeryvalerio.messinaNo ratings yet
- Ketorolac 10 Vs 30mgDocument2 pagesKetorolac 10 Vs 30mgvalerio.messinaNo ratings yet
- Gastrointestinal Complications After Pancreatoduodenectomy With Epidural Vs Patient-Controlled Intravenous AnalgesiaDocument12 pagesGastrointestinal Complications After Pancreatoduodenectomy With Epidural Vs Patient-Controlled Intravenous Analgesiavalerio.messinaNo ratings yet
- Evidence That Intrathecal Morphine-3-Glucuronide May Cause Pain EnhancementDocument15 pagesEvidence That Intrathecal Morphine-3-Glucuronide May Cause Pain Enhancementvalerio.messinaNo ratings yet
- A Comparison of Intrathecal and Intravenous Morphine For Analgesia After HepatectomyDocument10 pagesA Comparison of Intrathecal and Intravenous Morphine For Analgesia After Hepatectomyvalerio.messinaNo ratings yet
- Hiperalgesia y ToleranciaDocument13 pagesHiperalgesia y ToleranciaKaren OsorioNo ratings yet
- Effect of Intrathecally Administered Ketamine, Morphine, and Their Combination Added To Bupivacaine in Patients Undergoing Major Abdominal Cancer Surgery A Randomized, Double-Blind StudyDocument8 pagesEffect of Intrathecally Administered Ketamine, Morphine, and Their Combination Added To Bupivacaine in Patients Undergoing Major Abdominal Cancer Surgery A Randomized, Double-Blind Studyvalerio.messinaNo ratings yet
- Pancreatoduodenectomy - Enhanced Recovery After Surgery (ERAS) Recommendations 2019Document29 pagesPancreatoduodenectomy - Enhanced Recovery After Surgery (ERAS) Recommendations 2019Jorge OsorioNo ratings yet
- Evidence-Based Practices For Safe & Quality Care of Birthing Mothers & Their NewbornsDocument15 pagesEvidence-Based Practices For Safe & Quality Care of Birthing Mothers & Their NewbornsLore Anne Mhae SantosNo ratings yet
- Evidence-Based Clinical Practice Guidelines For Gastroesophageal Reflux Disease 2015Document17 pagesEvidence-Based Clinical Practice Guidelines For Gastroesophageal Reflux Disease 2015carolina.rahardjaNo ratings yet
- The New York Otolaryngology Group (NYOG) Go Live With SurgiMateDocument2 pagesThe New York Otolaryngology Group (NYOG) Go Live With SurgiMateAlexandra HartNo ratings yet
- Unit 4, Hospital FormularyDocument14 pagesUnit 4, Hospital FormularyNavya Sara SanthoshNo ratings yet
- NTP Referral FormDocument2 pagesNTP Referral FormCarl RamosNo ratings yet
- Cover Letter Heidi BosmansDocument1 pageCover Letter Heidi Bosmansapi-283672381No ratings yet
- Admin Volunteer RoleDocument2 pagesAdmin Volunteer RoleDotaKINGNo ratings yet
- San Pablo City Health Office Program Accomplishment Jan-Nov 2014 PDFDocument26 pagesSan Pablo City Health Office Program Accomplishment Jan-Nov 2014 PDFChoSanPabloNo ratings yet
- Ob NCP 2Document2 pagesOb NCP 2Kimberly Mondala (SHS)No ratings yet
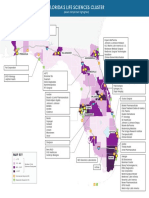
- Florida's Life Sciences Cluster MapDocument1 pageFlorida's Life Sciences Cluster MapCocoNo ratings yet
- Language Revitalization and The Problem of Development in Guatemala: Case Studies From Health CareDocument16 pagesLanguage Revitalization and The Problem of Development in Guatemala: Case Studies From Health CareWuqu' KawoqNo ratings yet
- Health Income and Poverty - Where We Are and What Could HelpDocument1 pageHealth Income and Poverty - Where We Are and What Could Helpapi-466415791No ratings yet
- Erin Wesolowski Resume 2021Document2 pagesErin Wesolowski Resume 2021api-544181914No ratings yet
- Dhikr Therapy For Reducing Anxiety in Cancer PatientDocument6 pagesDhikr Therapy For Reducing Anxiety in Cancer PatientRisfialdo Lily WidiatamaNo ratings yet
- OPD Psychiatric AssessmentDocument3 pagesOPD Psychiatric Assessmentraad_alghamdi_1No ratings yet
- Challenges To Implementation of The Pharmaceutical Care Practice in Davao City.Document11 pagesChallenges To Implementation of The Pharmaceutical Care Practice in Davao City.JessieLynMolinaNo ratings yet
- Lifestyle Coach Hiring Process at Goqii Technology PVTDocument9 pagesLifestyle Coach Hiring Process at Goqii Technology PVTAnkita SutarNo ratings yet
- Chapter 8 Drug Administration Throughout The LifespanDocument45 pagesChapter 8 Drug Administration Throughout The LifespanDiane VillegasNo ratings yet
- Fundamentals: From Taylor's Video Guide To Clinical Nursing SkillsDocument8 pagesFundamentals: From Taylor's Video Guide To Clinical Nursing SkillsMary Ann Lumbay PayeNo ratings yet
- Matthew Nippins PT, DPT, CCS: June 2007 To PresentDocument4 pagesMatthew Nippins PT, DPT, CCS: June 2007 To PresentPurush PeriyasamiNo ratings yet
- DOH Updates For PHA - May 6 Baguio PDFDocument49 pagesDOH Updates For PHA - May 6 Baguio PDFKaren BalanayNo ratings yet
- Statement of Purpose HDocument2 pagesStatement of Purpose HSamuel John IyanuoluwaNo ratings yet
- GPA Calculator (Pharmacy)Document4 pagesGPA Calculator (Pharmacy)MOHAMMED MNo ratings yet
- Dental Anxietyand Pain Perceptionassociatedwiththeuseof Miniscrew Implantsfor Orthodontics AnDocument6 pagesDental Anxietyand Pain Perceptionassociatedwiththeuseof Miniscrew Implantsfor Orthodontics Andruzair007No ratings yet
- Report of The Technical Consultation On Innovative Clinical Trial Designs For Evaluating New TB Preventive TreatmentsDocument59 pagesReport of The Technical Consultation On Innovative Clinical Trial Designs For Evaluating New TB Preventive TreatmentscarolNo ratings yet
- Validity WorksheetDocument4 pagesValidity WorksheetnaufalakbarNo ratings yet