You might also like
- Oral PathologyDocument9 pagesOral PathologyjanetNo ratings yet
- Cleaning of Dairy EquipmentDocument20 pagesCleaning of Dairy Equipmentmilind_vetyNo ratings yet
- Gotham Audio 1979 CatalogDocument16 pagesGotham Audio 1979 CatalogkeenastNo ratings yet
- Nematodes: Prepared By: Charriz A. AmoyanDocument81 pagesNematodes: Prepared By: Charriz A. AmoyanAudrie Allyson GabalesNo ratings yet
- AscarisDocument42 pagesAscarisمصطفي خندقاوي100% (1)
- (L-7) - Human Health and Disease - Dec 6, 2019Document68 pages(L-7) - Human Health and Disease - Dec 6, 2019Omar GillNo ratings yet
- Kuliah 17 - Nematoda Dan ProtozoaDocument72 pagesKuliah 17 - Nematoda Dan ProtozoaivaNo ratings yet
- INTESTINAL NEMATODES Hand Out 10 - 11Document6 pagesINTESTINAL NEMATODES Hand Out 10 - 11microperadeniyaNo ratings yet
- Para2020 10Document46 pagesPara2020 10Koko HashamNo ratings yet
- m1 - Helminthic InfectionDocument9 pagesm1 - Helminthic Infectionthe greatNo ratings yet
- Parasitology Helmit Print OutDocument64 pagesParasitology Helmit Print Outprabad dunusingheNo ratings yet
- Unit - Three: HelminthsDocument177 pagesUnit - Three: HelminthsDembalu NuguseNo ratings yet
- 12 - NematodaDocument44 pages12 - NematodaAnnisya MaharaniNo ratings yet
- Medical Helminthology DDSDocument85 pagesMedical Helminthology DDSMegbaruNo ratings yet
- Medical Helminthology-NematodesDocument134 pagesMedical Helminthology-NematodesKAYISIRE EMERYNo ratings yet
- Study of These Parasitic Worms and Their Medical ConsequenceDocument33 pagesStudy of These Parasitic Worms and Their Medical Consequenceabel semuNo ratings yet
- Introduction To HelminthsDocument39 pagesIntroduction To HelminthsEsther WanjukiNo ratings yet
- Tropical Medicine-1Document355 pagesTropical Medicine-1Fabb NelsonNo ratings yet
- Roun WormsDocument24 pagesRoun WormsBalach JanNo ratings yet
- Phylum Nematoda RoundwormsDocument22 pagesPhylum Nematoda Roundwormserica williamsNo ratings yet
- Protozoan Parasites: Gwy-Am Shin Office: Suite 2335, 4225 Roosevelt Phone: 206-543-9026 Email: Gwyam@u.washington - EduDocument35 pagesProtozoan Parasites: Gwy-Am Shin Office: Suite 2335, 4225 Roosevelt Phone: 206-543-9026 Email: Gwyam@u.washington - EduHazhar OmerNo ratings yet
- Medical Biology 6Document58 pagesMedical Biology 6Yusuf Yağız TimurNo ratings yet
- Pathogens in The Environment: - Viruses and Prions - Bacteria and Rickettsiae - Fungi and Algae - Protozoans - HelminthsDocument34 pagesPathogens in The Environment: - Viruses and Prions - Bacteria and Rickettsiae - Fungi and Algae - Protozoans - HelminthsEnaANo ratings yet
- Trichuris Trichiura: Lecture By: Maha Gamal AldeinDocument20 pagesTrichuris Trichiura: Lecture By: Maha Gamal AldeinMohammad DweibNo ratings yet
- Revision: Types of Life Cycle in Trematoda and CestodaDocument71 pagesRevision: Types of Life Cycle in Trematoda and CestodaMicroscopeGeekNo ratings yet
- Ascariasis & GiardiasisDocument34 pagesAscariasis & GiardiasisMuhammad ShahzadNo ratings yet
- Nematoda UsusDocument35 pagesNematoda Ususamanda fairuzNo ratings yet
- Defecating in The Morning, Because The Gravid Female Worms Usually Migrate at Night To The Perianal Region To Deposit EggsDocument4 pagesDefecating in The Morning, Because The Gravid Female Worms Usually Migrate at Night To The Perianal Region To Deposit EggsDaniella TupasNo ratings yet
- Ascaris LumbricoidesDocument32 pagesAscaris LumbricoideshassansjavaidNo ratings yet
- Material For Medicine pc2 StudentsDocument79 pagesMaterial For Medicine pc2 StudentskamaluNo ratings yet
- Mosquitoes & Their Related Diseases Day 1Document40 pagesMosquitoes & Their Related Diseases Day 1Yvonne RagguettNo ratings yet
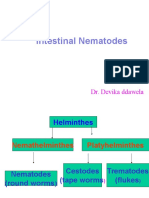
- Intestinal Nematodes: Dr. Devika DdawelaDocument127 pagesIntestinal Nematodes: Dr. Devika DdawelaPraveenKumarNo ratings yet
- HelminthsDocument17 pagesHelminthsur.yared21No ratings yet
- Ascaris Lumbricoides: Ascariasis. Infections Most Often Seen in Young Children byDocument7 pagesAscaris Lumbricoides: Ascariasis. Infections Most Often Seen in Young Children byThea GonzalesNo ratings yet
- Strongyloidiasis 2014Document33 pagesStrongyloidiasis 2014officialmwalusambaNo ratings yet
- Outline: 1. General Characteristics of Platyhelminthes 2. Classification of Platyhelminthes 3. Cestodes 4. TrematodesDocument73 pagesOutline: 1. General Characteristics of Platyhelminthes 2. Classification of Platyhelminthes 3. Cestodes 4. TrematodesAsxe CeeNo ratings yet
- N M To Es: Dr. Wafaa Ezz ElarabDocument31 pagesN M To Es: Dr. Wafaa Ezz Elarabshoroq zaki100% (1)
- Parasite Packet 1Document12 pagesParasite Packet 1api-595420397No ratings yet
- Arthropods of Medical ImportanceDocument33 pagesArthropods of Medical Importancecyrilsenior06No ratings yet
- Parasitic Infection in GI TractDocument123 pagesParasitic Infection in GI TractUtami HandayaniNo ratings yet
- Entomology - Members of Class Insecta, Order DipteraDocument88 pagesEntomology - Members of Class Insecta, Order Dipteramiki100% (1)
- Aljas&Bama (Microbm9evaluate)Document8 pagesAljas&Bama (Microbm9evaluate)Mary Clare Fuentes BamaNo ratings yet
- Helminths (Nematodes)Document42 pagesHelminths (Nematodes)RaunaNo ratings yet
- UntitledDocument51 pagesUntitledHesham MogicoNo ratings yet
- Infestation: ScabiesDocument16 pagesInfestation: ScabiesBrix ValdrizNo ratings yet
- 16 Performance Enhancement Sheet PDFDocument3 pages16 Performance Enhancement Sheet PDFSARA50% (2)
- NematoDocument15 pagesNematoRen Zo ImpelidoNo ratings yet
- AscariasisDocument44 pagesAscariasisMuhammad AuliaNo ratings yet
- NematodesDocument16 pagesNematodesBebreilynne LepartoNo ratings yet
- Lecture 7 - Parasitic Diseases - Bhunia - FS565 - 2023Document36 pagesLecture 7 - Parasitic Diseases - Bhunia - FS565 - 2023Anand KumarNo ratings yet
- AscarisDocument18 pagesAscarisHabib UllahNo ratings yet
- Nematodes & Infections of The SkinDocument39 pagesNematodes & Infections of The SkinHannah LaputNo ratings yet
- Kuliah Cacing WestyDocument63 pagesKuliah Cacing WestyIndra ToshiwayNo ratings yet
- Lect 2Document11 pagesLect 2Sara AliNo ratings yet
- Chapter 2.2.1 CestodesDocument73 pagesChapter 2.2.1 CestodesSufiyan AbduramanNo ratings yet
- Endoparasites Ectoparasites - LEC - 3Document16 pagesEndoparasites Ectoparasites - LEC - 3Medicine SWUNo ratings yet
- Project IN Parasitology: Submitted To: Dr. Ed de Vera Submitted By: Francesca Angela Nervar BSN - 2Document36 pagesProject IN Parasitology: Submitted To: Dr. Ed de Vera Submitted By: Francesca Angela Nervar BSN - 2Catherine MetraNo ratings yet
- Class Nematoda - The RoundwormsDocument76 pagesClass Nematoda - The RoundwormsLyraNo ratings yet
- Parasit Nematodes Summer 2012Document57 pagesParasit Nematodes Summer 2012Ilham SuryoNo ratings yet
- Phylum Platyhelminthes (Flatworms) : Important InformationDocument26 pagesPhylum Platyhelminthes (Flatworms) : Important InformationYoussef EmadNo ratings yet
- Lec 9 NematodesDocument11 pagesLec 9 NematodesMurtdha ArifNo ratings yet
- Adult - BLS - PPT 2Document49 pagesAdult - BLS - PPT 2urjaNo ratings yet
- Bone-LDocument34 pagesBone-LurjaNo ratings yet
- Muscle Tissue LectureDocument34 pagesMuscle Tissue LectureurjaNo ratings yet
- SkullDocument23 pagesSkullurjaNo ratings yet
- Thong So Banh RangDocument7 pagesThong So Banh RangVũ Trường LamNo ratings yet
- Simple Easy Daily Mantras For All Above 40 MantrasDocument45 pagesSimple Easy Daily Mantras For All Above 40 MantrasDr Naresh ChawhanNo ratings yet
- 6032 PDFDocument191 pages6032 PDFMuhammad KashifNo ratings yet
- RTS Chapter 2-3Document28 pagesRTS Chapter 2-3Anonymous 4iFUXUT100% (1)
- Rolliflex Cables: Field-Bus CablesDocument2 pagesRolliflex Cables: Field-Bus CablesnikhilbhorNo ratings yet
- To Trim An Artichoke: Don't Do It If There Are DistractionsDocument3 pagesTo Trim An Artichoke: Don't Do It If There Are DistractionsMary Joy JoniecaNo ratings yet
- Apqp Time Plan: Risk AnalysisDocument4 pagesApqp Time Plan: Risk AnalysisRakesh PandeyNo ratings yet
- Annual Report 2020 21Document268 pagesAnnual Report 2020 21David haughesNo ratings yet
- Bioavailability: A Pharmaceutical Review: January 2011Document18 pagesBioavailability: A Pharmaceutical Review: January 2011mahveen balochNo ratings yet
- Standards For Rolling Stock CablesDocument9 pagesStandards For Rolling Stock CablesNathathonNo ratings yet
- Tutorial 2 Ce5620Document2 pagesTutorial 2 Ce5620tulasi ramNo ratings yet
- E CROSSFIRE InstructionsDocument4 pagesE CROSSFIRE Instructionspraba_343No ratings yet
- Adventure - February 1938 PDFDocument148 pagesAdventure - February 1938 PDFulixesfoxNo ratings yet
- MDWF 2040 Practice Guideline Postpartum AnemiaDocument4 pagesMDWF 2040 Practice Guideline Postpartum Anemiaapi-442131145No ratings yet
- NITW RollingAdvt 2024Document8 pagesNITW RollingAdvt 2024Muthu KumarNo ratings yet
- ch2 PDFDocument49 pagesch2 PDFAndrew BorgNo ratings yet
- Simpsons 1/3 & 3/8 Rule. Cabajes ReportDocument7 pagesSimpsons 1/3 & 3/8 Rule. Cabajes ReportRbcabajes ButalonNo ratings yet
- Pharmac KineticsDocument30 pagesPharmac Kineticsimaslov16No ratings yet
- Ehnv1 Est1: EQP-, EP-and Two-Phase Titration Function FunctionsDocument2 pagesEhnv1 Est1: EQP-, EP-and Two-Phase Titration Function FunctionsFernando Chacmana LinaresNo ratings yet
- Theoretical Physics: Course Codes: Phys2325Document36 pagesTheoretical Physics: Course Codes: Phys2325kavimat20089274No ratings yet
- Genbio Smile Lp6 q1 Week6Document13 pagesGenbio Smile Lp6 q1 Week6Black Combat100% (1)
- Lung Volumes Lab ReportDocument11 pagesLung Volumes Lab ReportYani ManuelNo ratings yet
- ASTM F739 and EN 374 Product ComparisonDocument8 pagesASTM F739 and EN 374 Product Comparisonsimbua72No ratings yet
- Lecture 2Document51 pagesLecture 2degife deshaNo ratings yet
- Tutorial Práctico: Revit MEP 2013Document0 pagesTutorial Práctico: Revit MEP 2013Alfredo Castelo Suárez100% (2)
- Friday July 9, 2010 LeaderDocument48 pagesFriday July 9, 2010 LeaderSurrey/North Delta LeaderNo ratings yet
- Updated List of NGO 05.10.2016Document12 pagesUpdated List of NGO 05.10.2016Viraat SewrajNo ratings yet