You might also like
- Focus 3 2nd Word StoreDocument19 pagesFocus 3 2nd Word StoreSvetlana Bykovshchenko-Tymoshok0% (1)
- Service BulletinDocument16 pagesService BulletinFaizani Rahman100% (4)
- CMP Bengaluru - Final ReportDocument242 pagesCMP Bengaluru - Final ReportSajjad HossainNo ratings yet
- Rehabilitation After Total Joint Replacement: A Scoping StudyDocument15 pagesRehabilitation After Total Joint Replacement: A Scoping StudyAlvaro AlarconNo ratings yet
- Physiotherapy As An Initial Treatment Option For Femoroacetabular ImpingementDocument9 pagesPhysiotherapy As An Initial Treatment Option For Femoroacetabular ImpingementNicolas ParejaNo ratings yet
- 10 1016@j JHT 2017 02 001 PDFDocument10 pages10 1016@j JHT 2017 02 001 PDFGusti Ayu KrisnayantiNo ratings yet
- Overview:: Book Title:-Strategic Management Author:-Michael A. Hitt - R. Duane Ireland - Robert E. HoskissonDocument2 pagesOverview:: Book Title:-Strategic Management Author:-Michael A. Hitt - R. Duane Ireland - Robert E. HoskissonSuvid Sharma0% (1)
- KrckateDocument12 pagesKrckateKONJ VELIKINo ratings yet
- The Impact of Long-Term Follow-Up On Total Hip Arthroplasty: A Systematic ReviewDocument7 pagesThe Impact of Long-Term Follow-Up On Total Hip Arthroplasty: A Systematic ReviewIJAR JOURNALNo ratings yet
- Functional Outcome of Total Hip Arthroplasty With Dual Mobility Cups in Hip Arthritis-A Prospective Cohort StudyDocument7 pagesFunctional Outcome of Total Hip Arthroplasty With Dual Mobility Cups in Hip Arthritis-A Prospective Cohort StudyIJAR JOURNALNo ratings yet
- PRP Versus Aspirado de MedulaDocument9 pagesPRP Versus Aspirado de Medulajulionline7No ratings yet
- 16 Han (2019) IA PRP Vs IA HA - MADocument12 pages16 Han (2019) IA PRP Vs IA HA - MARevina BustamiNo ratings yet
- Operative Trends in The Treatment of Hip Fractures and The Role of ArthroplastyDocument10 pagesOperative Trends in The Treatment of Hip Fractures and The Role of ArthroplastyDonnaNo ratings yet
- GR Up: SM Orthopedics & Muscular SystemDocument6 pagesGR Up: SM Orthopedics & Muscular SystemValerie BpNo ratings yet
- Palmer 2019Document13 pagesPalmer 2019EricNo ratings yet
- Forgotten Joint Score PDFDocument8 pagesForgotten Joint Score PDFdeepakNo ratings yet
- BasilDocument17 pagesBasilvatra cristiNo ratings yet
- Bsms 6Document6 pagesBsms 6Filip starcevicNo ratings yet
- Biologic Options For Articular Cartilage Wear (Platelet-Rich Plasma, Stem C 2017Document12 pagesBiologic Options For Articular Cartilage Wear (Platelet-Rich Plasma, Stem C 2017drdabielmaderacNo ratings yet
- Meta Analysis Fusion ATCDocument4 pagesMeta Analysis Fusion ATCElPejelagartoNo ratings yet
- Revisión Sistematica Con Ma de Epicondilitis LateralDocument10 pagesRevisión Sistematica Con Ma de Epicondilitis LateralJorge GámezNo ratings yet
- The Journal of ArthroplastyDocument8 pagesThe Journal of Arthroplasty阿欧有怪兽No ratings yet
- Bot 0000000000002494Document9 pagesBot 0000000000002494Lukman Al NomaniNo ratings yet
- Consensus Statement For Perioperative Care in Total Hip Replacement and Total Knee Replacement Surgery: Enhanced Recovery After Surgery (ERAS®) Society RecommendationsDocument18 pagesConsensus Statement For Perioperative Care in Total Hip Replacement and Total Knee Replacement Surgery: Enhanced Recovery After Surgery (ERAS®) Society RecommendationsJuliana Moreno LadinoNo ratings yet
- Prevention of Dislocation After Total Hip ArthroplastyDocument9 pagesPrevention of Dislocation After Total Hip ArthroplastyAndrés MardonesNo ratings yet
- Functional Exercise After Total Hip Replacement FE PDFDocument8 pagesFunctional Exercise After Total Hip Replacement FE PDFRizqy DwitamaNo ratings yet
- ProposalDocument16 pagesProposalapi-450654874No ratings yet
- Assessing Results After Distal Radius Fracture TreDocument7 pagesAssessing Results After Distal Radius Fracture TreChristopher Freddy Bermeo RiveraNo ratings yet
- Outcomes of Hip Arthroscopy in Patients Aged 50 Years or Older Compared With A Matched-Pair Control of Patients Aged 30 Years or YoungerDocument8 pagesOutcomes of Hip Arthroscopy in Patients Aged 50 Years or Older Compared With A Matched-Pair Control of Patients Aged 30 Years or Youngersuad5stambulieNo ratings yet
- Effects of Orthopaedic Manual Therapy in Knee Osteoarthritis: A Systematic Review and Meta-AnalysisDocument13 pagesEffects of Orthopaedic Manual Therapy in Knee Osteoarthritis: A Systematic Review and Meta-AnalysisCollin AndrusNo ratings yet
- Educating Patients About The Benefits of Physical Activty and Exercise For Their Hip and Knee OA SDocument10 pagesEducating Patients About The Benefits of Physical Activty and Exercise For Their Hip and Knee OA SjotaNo ratings yet
- THA Polyethylene SurvivalDocument5 pagesTHA Polyethylene SurvivalCleff FlowersNo ratings yet
- BBRC Vol 14 No 04 2021-80Document5 pagesBBRC Vol 14 No 04 2021-80Dr Sharique AliNo ratings yet
- Intentional Weight Loss For Overweight and Obese KneeDocument16 pagesIntentional Weight Loss For Overweight and Obese Kneeafernandezd28No ratings yet
- Effectiveness of An 11-Week Exercise Intervention For Patients With Hip or Knee OsteoarthritisDocument17 pagesEffectiveness of An 11-Week Exercise Intervention For Patients With Hip or Knee Osteoarthritisyago.pessoaNo ratings yet
- Robotic Arm-Assisted Versus Manual Total Hip Arthroplasty A Propensity Score Matched Cohort StudyDocument9 pagesRobotic Arm-Assisted Versus Manual Total Hip Arthroplasty A Propensity Score Matched Cohort StudyShiv KolheNo ratings yet
- Raeissadat 2021Document14 pagesRaeissadat 2021gustamasindram17No ratings yet
- 2017 Article 528Document12 pages2017 Article 528Marios GhobrialNo ratings yet
- JCM 11 05091Document15 pagesJCM 11 05091Greice Westphal NardoNo ratings yet
- Comparative Efficacy of Neuraxial and General Anesthesia For Hip Fracture SurgeryDocument12 pagesComparative Efficacy of Neuraxial and General Anesthesia For Hip Fracture Surgeryangelama1783riosNo ratings yet
- 1 s2.0 S1877065718300915 Main PDFDocument1 page1 s2.0 S1877065718300915 Main PDFKasra AlborziNo ratings yet
- Osteoarthritis of The HipDocument2 pagesOsteoarthritis of The HipDewi WulansariNo ratings yet
- Prótese No JoelhoDocument17 pagesPrótese No JoelhoPaula SampaioNo ratings yet
- Remo V S Fijo 2Document12 pagesRemo V S Fijo 2Fiorella Gladys Rojas SalasNo ratings yet
- (2009) LAVIGNE - The Functional Outcome of Hip Resurfacing and Large-Head THA Is The SameDocument12 pages(2009) LAVIGNE - The Functional Outcome of Hip Resurfacing and Large-Head THA Is The SameSandro Luiz Machado CarvalhoNo ratings yet
- Loc BFRDocument6 pagesLoc BFRapi-290917332No ratings yet
- Physical Therapy in Sport: Cornelia Neuhaus, Christian Appenzeller-Herzog, Oliver FaudeDocument10 pagesPhysical Therapy in Sport: Cornelia Neuhaus, Christian Appenzeller-Herzog, Oliver FaudeBreechesNo ratings yet
- Total Disc Replacement in The Lumbar Spine: A Systematic Review of The LiteratureDocument9 pagesTotal Disc Replacement in The Lumbar Spine: A Systematic Review of The LiteratureEpi Vargas AlcarazNo ratings yet
- 2021 Dextrose Prolotherapy in Knee Osteoarthritis A Systematic Review and Meta-AnalysisDocument10 pages2021 Dextrose Prolotherapy in Knee Osteoarthritis A Systematic Review and Meta-AnalysiswanhsiorthopedicsNo ratings yet
- Scott 2015Document20 pagesScott 2015Raíla SoaresNo ratings yet
- Physiotherapy After Reconstruction of Anterior Cruciate LigamentDocument4 pagesPhysiotherapy After Reconstruction of Anterior Cruciate LigamentRmeMreErmNo ratings yet
- Tobert 2023Document8 pagesTobert 2023Will CKNo ratings yet
- Manual TheraManual Therapy For Osteoarthritis of The Hip or KneepDocument9 pagesManual TheraManual Therapy For Osteoarthritis of The Hip or KneepBwizerNo ratings yet
- 10 1016@j Otsr 2019 12 020Document8 pages10 1016@j Otsr 2019 12 020Wild EagleNo ratings yet
- Gebremariam 2013Document9 pagesGebremariam 2013Jailson CamposNo ratings yet
- JRRD 2014 05 0132Document12 pagesJRRD 2014 05 0132Jivanjot S. KohliNo ratings yet
- Physiotherapy For Patients With Hip and Knee Osteoarthritis in Germany: A Survey of Current PracticeDocument11 pagesPhysiotherapy For Patients With Hip and Knee Osteoarthritis in Germany: A Survey of Current PracticeJhonathan ErazoNo ratings yet
- Physiotherapy For Patients With Sciatica Awaiting Lumbar Micro-Discectomy Surgery - A Nested, Qualitative Study of Patients' Views and ExperiencesDocument10 pagesPhysiotherapy For Patients With Sciatica Awaiting Lumbar Micro-Discectomy Surgery - A Nested, Qualitative Study of Patients' Views and ExperiencesLindapratama SaifuddinNo ratings yet
- The Study To Assess The Effect of Prehabilitation On Postoperative Outcome of The Patients On Total Knee Arthroplasty at Selected HospitalDocument4 pagesThe Study To Assess The Effect of Prehabilitation On Postoperative Outcome of The Patients On Total Knee Arthroplasty at Selected HospitalEditor IJTSRDNo ratings yet
- InpingimenteDocument8 pagesInpingimenteFernandoVdklgAraujoNo ratings yet
- Pone 0179867Document18 pagesPone 0179867wirasenaNo ratings yet
- THR-morbid ObesityDocument5 pagesTHR-morbid ObesityMohan DesaiNo ratings yet
- The ASMBS Textbook of Bariatric Surgery: Volume 1: Bariatric SurgeryFrom EverandThe ASMBS Textbook of Bariatric Surgery: Volume 1: Bariatric SurgeryNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 17: OncologyFrom EverandComplementary and Alternative Medical Lab Testing Part 17: OncologyNo ratings yet
- KP06 - KP06 - Primary Cost Planning On Cost Centers: Cost Center Accounting Cost Center AccountingDocument8 pagesKP06 - KP06 - Primary Cost Planning On Cost Centers: Cost Center Accounting Cost Center AccountingbiggyjengNo ratings yet
- Present Status and Future Directions Microbiology of Endodontic Infections - 2021Document19 pagesPresent Status and Future Directions Microbiology of Endodontic Infections - 2021bogdimNo ratings yet
- October Month Vocabulary The Hindu Editorial Part-1Document10 pagesOctober Month Vocabulary The Hindu Editorial Part-1sauravNo ratings yet
- Environmental StudiesDocument2 pagesEnvironmental StudiesBlessy BlessyNo ratings yet
- 112 1971 Guitar NewsDocument32 pages112 1971 Guitar NewsMichel BrousseauNo ratings yet
- Morris and TschicholdDocument7 pagesMorris and TschicholdWhitney McCaskillNo ratings yet
- Political Cartoon Lesson PlanDocument9 pagesPolitical Cartoon Lesson PlanNicolas SawickyNo ratings yet
- 4 - Accounting For OverheadDocument12 pages4 - Accounting For Overheadjeams vidalNo ratings yet
- Bases - TopologyDocument7 pagesBases - TopologyRaja Ghufran ArifNo ratings yet
- 07 Subject Verb AgreementDocument14 pages07 Subject Verb AgreementMehak SrivastavaNo ratings yet
- Instructional Design Project Outline Christy HughesDocument3 pagesInstructional Design Project Outline Christy Hughesapi-560842067No ratings yet
- Help Seeking As A Self-Regulated Learning Strategy: January 2013Document14 pagesHelp Seeking As A Self-Regulated Learning Strategy: January 2013Agus PratomoNo ratings yet
- Anesthesia For Laparoscopy in The Pediatric PatientDocument20 pagesAnesthesia For Laparoscopy in The Pediatric PatientfathiahusainNo ratings yet
- (HOW-To) How To Update BIOS and EC For U2442 - v1Document20 pages(HOW-To) How To Update BIOS and EC For U2442 - v1anon_664289275No ratings yet
- HDFC Software Requirement Specification SrsDocument24 pagesHDFC Software Requirement Specification SrsAshish Roushan100% (1)
- Unit 3 Controlling The ConversationDocument2 pagesUnit 3 Controlling The ConversationdefiaaaNo ratings yet
- Weekly Learning Plan Science 7Document7 pagesWeekly Learning Plan Science 7sofia gamer girlNo ratings yet
- GeM Bidding 3656858 PDFDocument4 pagesGeM Bidding 3656858 PDFrip111176No ratings yet
- This Study Resource WasDocument4 pagesThis Study Resource WasDinesh tallaparthiNo ratings yet
- Dwnload Full Discovering Computers Essentials 2018 Digital Technology Data and Devices 1st Edition Vermaat Test Bank PDFDocument31 pagesDwnload Full Discovering Computers Essentials 2018 Digital Technology Data and Devices 1st Edition Vermaat Test Bank PDFjapitserre5100% (16)
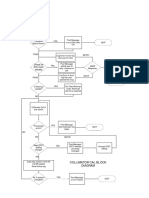
- Check For Dirty Mylar Window: Collimator Cal Block DiagramDocument1 pageCheck For Dirty Mylar Window: Collimator Cal Block DiagramMai Thanh SơnNo ratings yet
- Living With The Himalayan MastersDocument27 pagesLiving With The Himalayan MastersLauren Hughes0% (3)
- Verbal and Non Verbal2Document49 pagesVerbal and Non Verbal2Allana RayosNo ratings yet
- Postmortem Examination: Causes of Sudden Death in Animals. Collection and Dispatch of Materials For Chemical ExaminationDocument19 pagesPostmortem Examination: Causes of Sudden Death in Animals. Collection and Dispatch of Materials For Chemical Examinationkushal NeupaneNo ratings yet
- Verse 1: @0:11: HappierDocument2 pagesVerse 1: @0:11: HappierKristian GatchalianNo ratings yet
- Kabale University Government Sponsorship Admission List For Academic Year 2020Document9 pagesKabale University Government Sponsorship Admission List For Academic Year 2020The Campus Times100% (1)