You might also like
- Modern Methods for Affordable Clinical Gait Analysis: Theories and Applications in Healthcare SystemsFrom EverandModern Methods for Affordable Clinical Gait Analysis: Theories and Applications in Healthcare SystemsNo ratings yet
- Keisha Ferrell: Digital UI & UX LeadDocument67 pagesKeisha Ferrell: Digital UI & UX LeadKeisha FNo ratings yet
- Promotion Gamification: How and Why It Works: A Talon - One White PaperDocument16 pagesPromotion Gamification: How and Why It Works: A Talon - One White PaperAlexander GombergNo ratings yet
- BSBLDR403 Student Assessment Tasks V1.0Document29 pagesBSBLDR403 Student Assessment Tasks V1.0Mahamood Faisal100% (1)
- Final Draft Project Gamification CapstoneDocument34 pagesFinal Draft Project Gamification Capstoneapi-290871487No ratings yet
- VR 2Document9 pagesVR 2dindasaviraNo ratings yet
- Evaluation Mental Workload of Cognitive Tasks in Virtual Reality Using EOG Eye Tracker and EEG SignalsDocument16 pagesEvaluation Mental Workload of Cognitive Tasks in Virtual Reality Using EOG Eye Tracker and EEG SignalsJ Andrés SalasNo ratings yet
- Aricò 2018 Physiol. Meas. 39 08TR02Document20 pagesAricò 2018 Physiol. Meas. 39 08TR02Centro OrientaciónNo ratings yet
- A Review of Upper Limb Robot Assisted Therapy Techniques and Virtual Reality ApplicationsDocument11 pagesA Review of Upper Limb Robot Assisted Therapy Techniques and Virtual Reality ApplicationsIAES IJAINo ratings yet
- Research Paper On BciDocument7 pagesResearch Paper On Bcifysfs7g3100% (1)
- A Brain-Controlled Interface Based On Augmented Reality For Evolutionary Artificial IntelligenceDocument8 pagesA Brain-Controlled Interface Based On Augmented Reality For Evolutionary Artificial IntelligenceIJRASETPublicationsNo ratings yet
- Neurotechnology and Brain Computing InterfaceDocument12 pagesNeurotechnology and Brain Computing Interfaceurtanmayshuklaofficial1913No ratings yet
- Progress in Brain Computer Interface: Challenges and OpportunitiesDocument20 pagesProgress in Brain Computer Interface: Challenges and OpportunitiesSarammNo ratings yet
- TrainingofHandRehabilitation PDFDocument3 pagesTrainingofHandRehabilitation PDFYassine TazoutiNo ratings yet
- Exploring The Potential of Brain-Computer Interfaces in Managing Alzheimer's DiseaseDocument13 pagesExploring The Potential of Brain-Computer Interfaces in Managing Alzheimer's DiseaseIJRASETPublicationsNo ratings yet
- ArmeoPower HocomaDocument4 pagesArmeoPower HocomaralphholingsheadNo ratings yet
- Combine CogcomDocument13 pagesCombine CogcomdeasyNo ratings yet
- Fpubh 08 479431 PDFDocument7 pagesFpubh 08 479431 PDFdemon.akuma06No ratings yet
- Fneur 12 661816Document12 pagesFneur 12 661816Varadharajan RNo ratings yet
- EEG Robot PDFDocument21 pagesEEG Robot PDFDavid De Luna MartínezNo ratings yet
- Cognitive and Functional Outcomes Following Inpatient Rehabilitation in Patients With Acquired Brain Injury: A Prospective Follow Up StudyDocument8 pagesCognitive and Functional Outcomes Following Inpatient Rehabilitation in Patients With Acquired Brain Injury: A Prospective Follow Up Studyu3505483No ratings yet
- 2022 JNE Smart Bionic Eye CleanDocument20 pages2022 JNE Smart Bionic Eye CleanN R RaajanNo ratings yet
- An EEG Database For The CognitDocument16 pagesAn EEG Database For The Cognit911205josephNo ratings yet
- Quadcopter Control in Three-Dimensional Space Using A Noninvasive Motor Imagery-Based Brain-Computer InterfaceDocument16 pagesQuadcopter Control in Three-Dimensional Space Using A Noninvasive Motor Imagery-Based Brain-Computer InterfaceReza Ardiansyah MahedaNo ratings yet
- Brain Disease Detection Using Machine LearningDocument7 pagesBrain Disease Detection Using Machine LearningIJRASETPublications100% (1)
- Playstation Rehabilitation PDFDocument8 pagesPlaystation Rehabilitation PDFVivek Edamuriyil RamesanNo ratings yet
- Multimodal Signal Dataset For 11 Intuitive MovementDocument15 pagesMultimodal Signal Dataset For 11 Intuitive MovementVinicius SedrimNo ratings yet
- Brain Computer Interface BCI and The Rol PDFDocument12 pagesBrain Computer Interface BCI and The Rol PDFTARMIZI THALIBNo ratings yet
- 1 s2.0 S2667242122000628 MainDocument9 pages1 s2.0 S2667242122000628 Mainadam wilsonNo ratings yet
- Occupational Neuroplasticity BrainDocument15 pagesOccupational Neuroplasticity BrainGabriiella ChaviraNo ratings yet
- IOMT - Artigo Com Contribuição Do ProfessorDocument2 pagesIOMT - Artigo Com Contribuição Do ProfessorMarcio FilhoNo ratings yet
- A Fuzzy C Means Clustering Approach For Gesture Recognition in HealthcareDocument8 pagesA Fuzzy C Means Clustering Approach For Gesture Recognition in HealthcarekrishnanandNo ratings yet
- Survey of Human Gait Analysis and Recognition For Medical and Forensic ApplicationsDocument20 pagesSurvey of Human Gait Analysis and Recognition For Medical and Forensic ApplicationsSIRTE CSENo ratings yet
- Effect of Kinesio Taping On Hand Function in Hemiparetic PatientsDocument10 pagesEffect of Kinesio Taping On Hand Function in Hemiparetic PatientsZidni Ilma TianaNo ratings yet
- Music Game For Rehab With KinectDocument4 pagesMusic Game For Rehab With Kinectdorien82No ratings yet
- Gym Trainer Application Using Machine Learning.Document7 pagesGym Trainer Application Using Machine Learning.IJRASETPublicationsNo ratings yet
- Adaptive Robotic Neuro-Rehabilitation Haptic Device For Motor and Sensory Dysfunction PatientsDocument8 pagesAdaptive Robotic Neuro-Rehabilitation Haptic Device For Motor and Sensory Dysfunction PatientssnowdewdropNo ratings yet
- An Upper-Limb Rehabilitation Exoskeleton System Controlled by MI Recognition Model With Deep Emphasized Informative FeaDocument12 pagesAn Upper-Limb Rehabilitation Exoskeleton System Controlled by MI Recognition Model With Deep Emphasized Informative Fea911205josephNo ratings yet
- Liu 2020Document9 pagesLiu 2020barti koksNo ratings yet
- Rodríguez-Hernández Et Al. - 2021 - Effects of Specific Virtual Reality-Based TherapyDocument15 pagesRodríguez-Hernández Et Al. - 2021 - Effects of Specific Virtual Reality-Based TherapyMARIA TERAPEUTANo ratings yet
- Panagiotis Kourtesis, Danai Korre, Simona Collina, Leonidas A. A. Doumas and Sarah E. MacphersonDocument24 pagesPanagiotis Kourtesis, Danai Korre, Simona Collina, Leonidas A. A. Doumas and Sarah E. MacphersonYishuai ZhangNo ratings yet
- Behaviour Analysis For People With Mental Illness Using Machine LearningDocument7 pagesBehaviour Analysis For People With Mental Illness Using Machine LearningIJRASETPublicationsNo ratings yet
- Terapia Do Espelho Na Fratura de RadioDocument11 pagesTerapia Do Espelho Na Fratura de RadiodanfisiofoxNo ratings yet
- Virtualworlds 02 00001Document15 pagesVirtualworlds 02 00001Anonymous HUY0yRexYfNo ratings yet
- Myoelectric Control With Abstract DecodersDocument16 pagesMyoelectric Control With Abstract DecodersLaura PasqualNo ratings yet
- User-Guided 3D Active Contour Segmentation of Anatomical Structures: Significantly Improved Efficiency and ReliabilityDocument49 pagesUser-Guided 3D Active Contour Segmentation of Anatomical Structures: Significantly Improved Efficiency and ReliabilityNicholas KimNo ratings yet
- Sensors 20 05083 v2Document36 pagesSensors 20 05083 v2Sarani2 kalpanaNo ratings yet
- Abiri 2019 J. Neural Eng. 16 011001Document22 pagesAbiri 2019 J. Neural Eng. 16 011001xiansheng FNo ratings yet
- A Collaborative Brain-Computer Interface For Improving Human PerformanceDocument11 pagesA Collaborative Brain-Computer Interface For Improving Human Performancehyperion1No ratings yet
- Clinical Study: Rehabilitation of Children With Hemiparesis: A Pilot Study On The Use of Virtual RealityDocument5 pagesClinical Study: Rehabilitation of Children With Hemiparesis: A Pilot Study On The Use of Virtual RealityAitana Castro BravoNo ratings yet
- Articulo Febrero 25Document13 pagesArticulo Febrero 25Matthew PhillipsNo ratings yet
- Scientific Research Paper (Draft 2)Document9 pagesScientific Research Paper (Draft 2)condoleeza smithNo ratings yet
- A 3D Printed, Bionic Hand Powered by EMG Signals and Controlled by An Online Neural NetworkDocument33 pagesA 3D Printed, Bionic Hand Powered by EMG Signals and Controlled by An Online Neural NetworkDr Edward PeterNo ratings yet
- AI Application For Body Stiffness in Parkinsons DiseaseDocument6 pagesAI Application For Body Stiffness in Parkinsons DiseaseIJRASETPublicationsNo ratings yet
- 1 s2.0 S016926071730113X MainDocument6 pages1 s2.0 S016926071730113X MainGabriella CsernákNo ratings yet
- Castells-Sánchez 2022Document14 pagesCastells-Sánchez 2022Juan Pablo Espinoza PuellesNo ratings yet
- Rega Sugianto - J120190031 - EJHD Article Review 1Document20 pagesRega Sugianto - J120190031 - EJHD Article Review 1j130235024No ratings yet
- Fnhum 09 00716Document6 pagesFnhum 09 00716Monica Arellano LlacsaNo ratings yet
- Ieee Research Paper On Brain Computer InterfaceDocument10 pagesIeee Research Paper On Brain Computer Interfacefvgy6fn3100% (1)
- Efficacy of Virtual Reality in Upper Limb Rehabilitation in Patients With Spinal Cord Injury: A Pilot Randomized Controlled TrialDocument8 pagesEfficacy of Virtual Reality in Upper Limb Rehabilitation in Patients With Spinal Cord Injury: A Pilot Randomized Controlled TrialElsi Nursyahdin MayaranaNo ratings yet
- Clinical Features To Predict The Use of A SEMG Wearable Device (Remo) For Hand Motor Training of Stroke Patients A Cross-Sectional Cohort StudyDocument15 pagesClinical Features To Predict The Use of A SEMG Wearable Device (Remo) For Hand Motor Training of Stroke Patients A Cross-Sectional Cohort Studydaniele riminiNo ratings yet
- Xóa 2Document21 pagesXóa 2Rin TohsakaNo ratings yet
- Wearable Assistive Devices.: ArticleDocument18 pagesWearable Assistive Devices.: ArticleMegahakeNo ratings yet
- Research Paper Artificial Intelligence in Medical JEEV AI-IJRASETDocument8 pagesResearch Paper Artificial Intelligence in Medical JEEV AI-IJRASETIJRASETPublicationsNo ratings yet
- Chi-Tsong Chen-Linear System Theory Design-Oxford University Press-1998Document176 pagesChi-Tsong Chen-Linear System Theory Design-Oxford University Press-1998Alison Rocha100% (1)
- System Grounding of Wind Farm Medium Voltage Cable Grids: Hansen, Peter Østergaard, Jacob Christiansen, Jan SDocument6 pagesSystem Grounding of Wind Farm Medium Voltage Cable Grids: Hansen, Peter Østergaard, Jacob Christiansen, Jan SAlison RochaNo ratings yet
- Safety of Wind Farm Grounding Systems Under Fault and Lightning CurrentsDocument7 pagesSafety of Wind Farm Grounding Systems Under Fault and Lightning CurrentsAlison RochaNo ratings yet
- Windfarm Grounding: March 2016Document7 pagesWindfarm Grounding: March 2016Alison RochaNo ratings yet
- Masterarbeit DoGood - A Gamified Mobile App To Promote Civic EngagementDocument10 pagesMasterarbeit DoGood - A Gamified Mobile App To Promote Civic EngagementMichaelaNo ratings yet
- METUIGA "Methodology For The Design of Systems Based On Tangible User Interfaces and Gamification Techniques"Document21 pagesMETUIGA "Methodology For The Design of Systems Based On Tangible User Interfaces and Gamification Techniques"Uriel CarbajalNo ratings yet
- Using ClassCraft To Improve Primary SchoDocument21 pagesUsing ClassCraft To Improve Primary SchoJuan PedroNo ratings yet
- Cell Deal: An Instructional Card Game in Teaching Cellular Respiration in Selected Grade 12 Stem Students of Higher School NG Umak A.Y. 2018-2019Document19 pagesCell Deal: An Instructional Card Game in Teaching Cellular Respiration in Selected Grade 12 Stem Students of Higher School NG Umak A.Y. 2018-2019Ana Jone PulidoNo ratings yet
- A Systematic Mapping Study On Game-Related Methods For Software Engineering EducationDocument18 pagesA Systematic Mapping Study On Game-Related Methods For Software Engineering EducationSaptari WijayaNo ratings yet
- TTL2 Final RequirementDocument6 pagesTTL2 Final RequirementLyle ClaudetteNo ratings yet
- Ethical Issues in Gaming: A Literature Review: October 2018Document19 pagesEthical Issues in Gaming: A Literature Review: October 2018Zarfan HussainNo ratings yet
- Handout Webinar Session 1Document77 pagesHandout Webinar Session 1Vivian VillacortesNo ratings yet
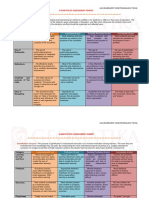
- Assessment Rubric For Class ProjectDocument3 pagesAssessment Rubric For Class ProjectJack OoiNo ratings yet
- ENHANCING LEARNING INTEREST IN ARALING PANLIPUNAN 3 THROUGH THE USE OF MULTIMEDIA BASED INSTRUCTION Ijariie21299Document14 pagesENHANCING LEARNING INTEREST IN ARALING PANLIPUNAN 3 THROUGH THE USE OF MULTIMEDIA BASED INSTRUCTION Ijariie21299Jiewel Rich BelmonteNo ratings yet
- Designing E-Courses For Hearing Impaired StudentsDocument14 pagesDesigning E-Courses For Hearing Impaired Studentssaffuan saadNo ratings yet
- Prodhive: B.A.S.H 5.0Document9 pagesProdhive: B.A.S.H 5.0Goverdhan Gupta 4-Yr B.Tech.: Mechanical Engg., IIT(BHU)No ratings yet
- Course Syllabus Gamification RevisedDocument4 pagesCourse Syllabus Gamification RevisedHeather Burnett100% (1)
- Gamification Elements and Their Impacts PDFDocument10 pagesGamification Elements and Their Impacts PDFAkmad Ali AbdulNo ratings yet
- The Application of Gamification in Education, Does It Effective?Document8 pagesThe Application of Gamification in Education, Does It Effective?Rofi AriawanNo ratings yet
- Gamification Using Game Design Elements in Non-GamDocument5 pagesGamification Using Game Design Elements in Non-GamMermaid ArielNo ratings yet
- Gamification Application in Different Business Software Systems - State of ArtDocument10 pagesGamification Application in Different Business Software Systems - State of ArtZornitsa YordanovaNo ratings yet
- A Preliminary Taxonomy of Gamification Elements For Varying Anticipated CommitmentDocument6 pagesA Preliminary Taxonomy of Gamification Elements For Varying Anticipated CommitmentM. MelendresNo ratings yet
- The Effects of Game Dynamics On User Engagement in Gamified SystemsDocument10 pagesThe Effects of Game Dynamics On User Engagement in Gamified SystemsCristian Alexander ospinaNo ratings yet
- The Design and Implementation of Gamified Classroom Through Schoology PlatformDocument9 pagesThe Design and Implementation of Gamified Classroom Through Schoology PlatformTony GomezNo ratings yet
- BBVA Innovation Edge Gamification EnglishDocument64 pagesBBVA Innovation Edge Gamification Englisherick_pacheco_38100% (1)
- Morrison DHI 2022 Emerging Innovations in Digital Health A Deeper DiveDocument21 pagesMorrison DHI 2022 Emerging Innovations in Digital Health A Deeper DiveRaquel Simões de AlmeidaNo ratings yet
- The Disruption of EducationDocument91 pagesThe Disruption of EducationhellojaimeNo ratings yet
- (Innoduction Group) 「中學IT創新實驗室計劃 」Info. for SchoolDocument19 pages(Innoduction Group) 「中學IT創新實驗室計劃 」Info. for SchoolKwok TerenceNo ratings yet
- Open Social Buying Guide 1Document28 pagesOpen Social Buying Guide 1Syazwan SamuraiNo ratings yet
- HBRCase GasBuddy2.0Document24 pagesHBRCase GasBuddy2.0ShankarNo ratings yet