You might also like
- 2023 - Mechanical Characterization of A NovelDocument9 pages2023 - Mechanical Characterization of A NovelAbdelrahman AbdelgawadNo ratings yet
- Posterior Subaxial Cervical Spine Screw Fixation: A Review of TechniquesDocument10 pagesPosterior Subaxial Cervical Spine Screw Fixation: A Review of TechniquesJaime XavierNo ratings yet
- Case Presentation of Sagital BalanceDocument1 pageCase Presentation of Sagital BalanceAndrés Urrego NietoNo ratings yet
- LWBK836 Ch117 p1265-1278Document14 pagesLWBK836 Ch117 p1265-1278metasoniko81No ratings yet
- Feature: An Introduction To Cranial Movement and OrthodonticsDocument4 pagesFeature: An Introduction To Cranial Movement and OrthodonticsabeNo ratings yet
- Artigo ClamshellDocument15 pagesArtigo ClamshellbritocirurgiadamaoNo ratings yet
- Basic Arthroplasty - Unit 3 - Varus TKa Balance SalehDocument9 pagesBasic Arthroplasty - Unit 3 - Varus TKa Balance SalehShu Yang HuNo ratings yet
- LWBK836 Ch98 p1021-1030Document10 pagesLWBK836 Ch98 p1021-1030metasoniko81No ratings yet
- Modul Hip Disarticulation ProstheticsDocument67 pagesModul Hip Disarticulation ProstheticsCapt KidsNo ratings yet
- Letters To The Editor: Rationale Behind Twin-Block InclineDocument1 pageLetters To The Editor: Rationale Behind Twin-Block InclineHARITHA H.PNo ratings yet
- Sitting and Low Back Disorders: An Overview of The Most Commonly Suggested Harmful MechanismsDocument7 pagesSitting and Low Back Disorders: An Overview of The Most Commonly Suggested Harmful MechanismsHana Laila NabilahNo ratings yet
- Rehabilitation in The Dynamic Stabilization of The Lumbosacral Spine PDFDocument41 pagesRehabilitation in The Dynamic Stabilization of The Lumbosacral Spine PDFAndrei100% (1)
- Spinal Cord Injury: Causation & PathophysiologyDocument10 pagesSpinal Cord Injury: Causation & Pathophysiologycpradheep100% (3)
- Concepts in Cervical TractionDocument6 pagesConcepts in Cervical TractionmritunjayNo ratings yet
- Article 5Document10 pagesArticle 5Rangga InktaenNdoek'sNo ratings yet
- Diagnostic Challenges in Musculoskeletal Radiology PDFDocument182 pagesDiagnostic Challenges in Musculoskeletal Radiology PDFphuong mai leNo ratings yet
- Winters 2014Document12 pagesWinters 2014TOMAS DAVID CHICA LLAMASNo ratings yet
- Chapter 19Document25 pagesChapter 19MuhammadMusa47No ratings yet
- Rib FractureDocument6 pagesRib FracturenasyilaputriNo ratings yet
- SMR 00275 ShoulderDocument15 pagesSMR 00275 ShoulderIulian FrunzăNo ratings yet
- Posterior Approaches To The Tibial PlateauDocument5 pagesPosterior Approaches To The Tibial Plateauana starcevicNo ratings yet
- Postlaminectomy Deformities in The Thoracic and Lumbar SpineDocument6 pagesPostlaminectomy Deformities in The Thoracic and Lumbar Spinemetasoniko81No ratings yet
- Biomechanics and Shape of The Above-Knee Socket Considered in Light of The Ischial Containment ConceptDocument13 pagesBiomechanics and Shape of The Above-Knee Socket Considered in Light of The Ischial Containment ConceptBapina Kumar RoutNo ratings yet
- Fronto-Orbital Advancement Using An en Bloc Frontal Bone CraniectomyDocument7 pagesFronto-Orbital Advancement Using An en Bloc Frontal Bone Craniectomyandredwijaya8No ratings yet
- Mechanical Loading of The Intervertebral Disc: From The Macroscopic To The Cellular LevelDocument12 pagesMechanical Loading of The Intervertebral Disc: From The Macroscopic To The Cellular LevelDaniel FreireNo ratings yet
- Acdf CervicalDocument8 pagesAcdf CervicalRhonda Lynne GriffithNo ratings yet
- Benzakour-Benzakour2019 Article DiscHerniationAndDiscDiseaseTh PDFDocument6 pagesBenzakour-Benzakour2019 Article DiscHerniationAndDiscDiseaseTh PDFLee제노No ratings yet
- Kne20 25302 v1 Biosure Opt Tg-FinalDocument16 pagesKne20 25302 v1 Biosure Opt Tg-FinalJuan Martinez Del AngelNo ratings yet
- Surgical Stabilization of SpineDocument4 pagesSurgical Stabilization of SpineMaria Jonnalin SantosNo ratings yet
- Completely thoracoscopic surgical stabilizationDocument9 pagesCompletely thoracoscopic surgical stabilizationduke3443No ratings yet
- Surgical Repair and Rehabilitation ProtocolsDocument28 pagesSurgical Repair and Rehabilitation ProtocolsSiti FahwizaNo ratings yet
- Kibler Et Al 2012 Scapula Dyskinesis and Its Relation To Shoulder Injury PDFDocument9 pagesKibler Et Al 2012 Scapula Dyskinesis and Its Relation To Shoulder Injury PDFPamela DíazNo ratings yet
- CH 32Document16 pagesCH 32willyoueverlovemenkNo ratings yet
- Rehabilitation in The Dynamic Stabilization of Lumbar SpineDocument41 pagesRehabilitation in The Dynamic Stabilization of Lumbar SpineYip Song ChongNo ratings yet
- Beltran - Diagnostic Challenges Musculoskeletal RadiologyDocument181 pagesBeltran - Diagnostic Challenges Musculoskeletal RadiologyAndrei GianinaNo ratings yet
- Treatment Scapular Winging 2007Document7 pagesTreatment Scapular Winging 2007YassineNo ratings yet
- Evaluation and Management of PDocument14 pagesEvaluation and Management of PIndra YudhaNo ratings yet
- Traction : LumbarDocument10 pagesTraction : LumbarAkshaya MistryNo ratings yet
- Surgical Challenges in Complex Primary Total Hip ADocument9 pagesSurgical Challenges in Complex Primary Total Hip Aehabede6445No ratings yet
- 1 s2.0 S1356689X16000400 MainDocument12 pages1 s2.0 S1356689X16000400 MainRelviGuzmanApazaNo ratings yet
- Estabildiad EspinalDocument9 pagesEstabildiad EspinalLuis Carlos Avellaneda CurchoNo ratings yet
- Reverse ShoulderreplacementDocument8 pagesReverse ShoulderreplacementagniosaiNo ratings yet
- Acta 92 26Document14 pagesActa 92 26Gustavo BECERRA PERDOMONo ratings yet
- Deen 2017Document5 pagesDeen 2017GERARDO TORRES RUIZNo ratings yet
- Aldrirdge - SurgicalTechDocument16 pagesAldrirdge - SurgicalTechÇağdaş PamukNo ratings yet
- History of Spine InstrumentationDocument35 pagesHistory of Spine InstrumentationSyarifNo ratings yet
- FX Pelvic Rim Injury17Document8 pagesFX Pelvic Rim Injury17Antonio PáezNo ratings yet
- Gust Ke 2005Document4 pagesGust Ke 2005Akshay DudhanaleNo ratings yet
- A Century of Tibial Intramedullary NailingDocument12 pagesA Century of Tibial Intramedullary NailingLi A VélezNo ratings yet
- Querleu 2017Document7 pagesQuerleu 2017Zaniru Raúl Marín MartínezNo ratings yet
- Luthringer 2019Document14 pagesLuthringer 2019Cristian Diaz KooNo ratings yet
- Femoral Shaft Fractures in AdultsDocument12 pagesFemoral Shaft Fractures in AdultsDiego BellingNo ratings yet
- Instructional: Course LecturesDocument25 pagesInstructional: Course LecturesIan GallardoNo ratings yet
- Manual Therapy: Jeremy LewisDocument12 pagesManual Therapy: Jeremy LewisMariano OsorioNo ratings yet
- Glenohumeral Joint Instability: ReviewDocument15 pagesGlenohumeral Joint Instability: ReviewOrto MespNo ratings yet
- Proximal Humerus Fracture Fixation Surgical TechnicDocument6 pagesProximal Humerus Fracture Fixation Surgical TechnicAdhimas WicaksanaNo ratings yet
- Arthroplasty TodayDocument7 pagesArthroplasty TodaySanty OktavianiNo ratings yet
- Operative Brachial Plexus Surgery: Clinical Evaluation and Management StrategiesFrom EverandOperative Brachial Plexus Surgery: Clinical Evaluation and Management StrategiesAlexander Y. ShinNo ratings yet
- 10-22-14 EditionDocument32 pages10-22-14 EditionSan Mateo Daily JournalNo ratings yet
- CDH Sextant II ST Mdt18802Document48 pagesCDH Sextant II ST Mdt18802Choong Tze ShanNo ratings yet
- Platelet-Rich Plasma Injections: An Emerging Therapy For Chronic Discogenic Low Back PainDocument8 pagesPlatelet-Rich Plasma Injections: An Emerging Therapy For Chronic Discogenic Low Back PainNoura RoseNo ratings yet
- Differential Diagnosis of Low Back Pain: Elizabeth Huntoon, MD, and Marc Huntoon, MDDocument7 pagesDifferential Diagnosis of Low Back Pain: Elizabeth Huntoon, MD, and Marc Huntoon, MDGangsar DamaiNo ratings yet
- Degenerative Disc DiseaseDocument3 pagesDegenerative Disc DiseaseNikolas LawrenceNo ratings yet
- Torillos V Eastgate Maritime CorpDocument22 pagesTorillos V Eastgate Maritime CorpanitaNo ratings yet
- DEGENERATIVE SPINE DISEASE and HomeopathyDocument21 pagesDEGENERATIVE SPINE DISEASE and Homeopathypawajee100% (3)
- Low Back PainDocument15 pagesLow Back PainwidiaNo ratings yet
- Diagnosis and Treatment of Cervical SpondylosisDocument170 pagesDiagnosis and Treatment of Cervical SpondylosisMihai Costache100% (1)
- Daily Diary Stress and Mood Variation/TITLEDocument103 pagesDaily Diary Stress and Mood Variation/TITLEFilsa Putri AnwarNo ratings yet
- Blue Manila DigestDocument5 pagesBlue Manila DigestLenette LupacNo ratings yet
- Percutaneous Imaging-Guided Spinal Facet Joint InjectionsDocument6 pagesPercutaneous Imaging-Guided Spinal Facet Joint InjectionsAlvaro Perez HenriquezNo ratings yet
- Clinical Observation On Greeva StambhaDocument10 pagesClinical Observation On Greeva StambhaSanjay SoniNo ratings yet
- 1 s2.0 S1529943016309226 MainDocument6 pages1 s2.0 S1529943016309226 Mainhakan sonsuzlukluNo ratings yet
- The Enciclopedia of The Back and Spine Systems and Disorders 2007 UCLADocument369 pagesThe Enciclopedia of The Back and Spine Systems and Disorders 2007 UCLAOana CristeaNo ratings yet
- Manchikanti 2015Document14 pagesManchikanti 2015Jose PerezNo ratings yet
- Test Bank For Physical Agents Theory and Practice 3rd Edition Barbara J Behrens Holly Beinert DownloadDocument11 pagesTest Bank For Physical Agents Theory and Practice 3rd Edition Barbara J Behrens Holly Beinert Downloadryanparker18011988fno100% (20)
- SPINE Supplement April 2017 PDFDocument33 pagesSPINE Supplement April 2017 PDFGuna KalanjiyamNo ratings yet
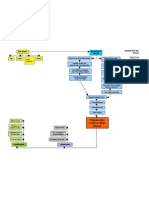
- Degenerative Disc Disease Concept MapDocument1 pageDegenerative Disc Disease Concept MapashleydeanNo ratings yet
- Saunders Lumbar TractionDocument12 pagesSaunders Lumbar TractionIra AdventiaNo ratings yet
- LDDDDocument21 pagesLDDDIvha RifaiNo ratings yet
- Degenerative Disc Disease GuideDocument13 pagesDegenerative Disc Disease Guidehouki shanaNo ratings yet
- Degenerative Spine DiseaseDocument17 pagesDegenerative Spine DiseasekidrocksbodydblNo ratings yet
- Lumbar Degenerative Disk Disease - StatPearls - NCBI BookshelfDocument6 pagesLumbar Degenerative Disk Disease - StatPearls - NCBI BookshelfAhmad SyahmiNo ratings yet
- Icd 10 Dan 9 Rehab MedikDocument78 pagesIcd 10 Dan 9 Rehab MedikAndrean Bagus MahendraNo ratings yet
- TlifDocument8 pagesTlifmichael gimenezNo ratings yet
- Pathology ReviewDocument430 pagesPathology Reviewpatriciacaf100% (2)
- Thesis-MECHANICAL EVALUATION OF POLYCARBONATEDocument185 pagesThesis-MECHANICAL EVALUATION OF POLYCARBONATEWahyu DwilestariNo ratings yet
- Cheap Steroid Injection Cost GuideDocument2 pagesCheap Steroid Injection Cost GuideMarielaNo ratings yet
- Degenerative Disc Disease - Adrienne Ingalls PDFDocument34 pagesDegenerative Disc Disease - Adrienne Ingalls PDFVenkatesanSelvarajan100% (1)