You might also like
- Treatment Strategy of Terrible Triad of The Elbow - Experience in Shanghai 6th People's HospitalDocument7 pagesTreatment Strategy of Terrible Triad of The Elbow - Experience in Shanghai 6th People's HospitalAndrea OsborneNo ratings yet
- Bulut 2018Document5 pagesBulut 2018José Luis Velasquez UrregoNo ratings yet
- Cole 2013Document5 pagesCole 2013Angie MorrisNo ratings yet
- The Incidence of Posterior Tibial Plateau Fracture: An Investigation of 525 Fractures by Using A CT-based Classification SystemDocument6 pagesThe Incidence of Posterior Tibial Plateau Fracture: An Investigation of 525 Fractures by Using A CT-based Classification SystemJuan GomezNo ratings yet
- 264 2014 Article 2282Document4 pages264 2014 Article 2282fm123165464No ratings yet
- Ulnar Variance As A Predictor of Persistent Instability Following Galeazzi Fracture-DislocationsDocument6 pagesUlnar Variance As A Predictor of Persistent Instability Following Galeazzi Fracture-DislocationsGus AbellaNo ratings yet
- Clasificación de HertelDocument7 pagesClasificación de HertelLuis Arturo Orozco MendozaNo ratings yet
- DL TPSFDocument5 pagesDL TPSFPramod N KNo ratings yet
- JCM 12 06172Document12 pagesJCM 12 06172Taulant MukaNo ratings yet
- iCVTPFDocument5 pagesiCVTPFErwin Chiquete, MD, PhDNo ratings yet
- Short Versus Long Outcome RadiologisDocument7 pagesShort Versus Long Outcome Radiologisandy ardiansyahNo ratings yet
- Quantification of Fracture Healing From Radiographs Using The Maximum Callus IndexDocument6 pagesQuantification of Fracture Healing From Radiographs Using The Maximum Callus IndexFaheem AhmedNo ratings yet
- Position Syndesmotic ScrewDocument4 pagesPosition Syndesmotic ScrewRoger WatersNo ratings yet
- Paper 38Document6 pagesPaper 38Dr Vineet KumarNo ratings yet
- McGonagle2019 Article TibiaPlateauFractureMappingAndDocument6 pagesMcGonagle2019 Article TibiaPlateauFractureMappingAndFarizka Dwinda HNo ratings yet
- Periprosthetic Femoral Fractures Above Total Knee ReplacementsDocument10 pagesPeriprosthetic Femoral Fractures Above Total Knee ReplacementsSpelliardNo ratings yet
- Demi RelDocument4 pagesDemi RelChrysi TsiouriNo ratings yet
- Chloros2008 231022 130529Document12 pagesChloros2008 231022 130529Cristian SanchezNo ratings yet
- Ueki 2007Document7 pagesUeki 2007abhishekjha0082No ratings yet
- Fsurg 10 1085636Document7 pagesFsurg 10 1085636zxiaoxing087No ratings yet
- Low Thoracic and Lumbar Burst Fractures - Radiographic and Functional OutcomesDocument10 pagesLow Thoracic and Lumbar Burst Fractures - Radiographic and Functional Outcomesmuhammad bayu wicaksonoNo ratings yet
- Jurnal Zygomatic 2013Document7 pagesJurnal Zygomatic 2013Defri ChanNo ratings yet
- Giacalone 2015Document7 pagesGiacalone 2015Joseval FilhoNo ratings yet
- Articulo DanielaDocument5 pagesArticulo DanielaSonsiret ReeveNo ratings yet
- Stabilization of Distal Humerus Fractures by Precontoured Bi-Condylar Plating in A 90-90 PatternDocument5 pagesStabilization of Distal Humerus Fractures by Precontoured Bi-Condylar Plating in A 90-90 PatternmayNo ratings yet
- Resection Arthroplasty of The Sternoclavicular Joint: J Bone Joint Surg AmDocument8 pagesResection Arthroplasty of The Sternoclavicular Joint: J Bone Joint Surg AmPersonil MonkthreeysNo ratings yet
- Vol29 - No2 - 59 - 63Document5 pagesVol29 - No2 - 59 - 63Kagiso Gigfreak Urban RoccoNo ratings yet
- BJR 20140542Document8 pagesBJR 20140542Sava Marius ConstantinNo ratings yet
- Medi 96 E5936Document5 pagesMedi 96 E5936arm.solis32No ratings yet
- 2309499017692700Document5 pages2309499017692700calinNo ratings yet
- 264 2013 Article 2112Document6 pages264 2013 Article 2112Anil KumarNo ratings yet
- Cui 2013Document6 pagesCui 2013endNo ratings yet
- 2021 - Chronic Isolated Radial Head DislocationDocument9 pages2021 - Chronic Isolated Radial Head Dislocationjuan pablo aguirreNo ratings yet
- Clavicle FractureDocument121 pagesClavicle FractureMuhamad Agung SupriyantoNo ratings yet
- Operative Treatment of Peritrochanteric Osteoporotic Fractures With Proximal Femur Locking Compression Plate A Consecutive StudyDocument6 pagesOperative Treatment of Peritrochanteric Osteoporotic Fractures With Proximal Femur Locking Compression Plate A Consecutive StudyAthenaeum Scientific PublishersNo ratings yet
- A Study On Management of Bothbones Forearm Fractures With Dynamic Compression PlateDocument5 pagesA Study On Management of Bothbones Forearm Fractures With Dynamic Compression PlateIOSRjournalNo ratings yet
- Zygomatic Arch Deformation - An Anatomic and Clinical StudyDocument8 pagesZygomatic Arch Deformation - An Anatomic and Clinical StudyGabriel LeviNo ratings yet
- Intramedullary Nailing of Distal Metaphyseal.5Document9 pagesIntramedullary Nailing of Distal Metaphyseal.5Joël Clarck EkowongNo ratings yet
- Accuracy and Longitudinal Reproducibility of QuantDocument18 pagesAccuracy and Longitudinal Reproducibility of QuantChristian Huapaya ContrerasNo ratings yet
- Results: (KAJ) Kurdistan Academician Journal, Sept 2003, 2 (1) Part ADocument6 pagesResults: (KAJ) Kurdistan Academician Journal, Sept 2003, 2 (1) Part AAcademecian groupNo ratings yet
- The Epidemiology of Open Long Bone FracturesDocument6 pagesThe Epidemiology of Open Long Bone FracturesLuigi Paolo Zapata DelgadoNo ratings yet
- Does Subacromial Osteolysis Affect Shoulder Function After Clavicle Hook Plating 2016Document5 pagesDoes Subacromial Osteolysis Affect Shoulder Function After Clavicle Hook Plating 2016陳韋傑No ratings yet
- Jurnal 1Document5 pagesJurnal 1Yakobus Anthonius SobuberNo ratings yet
- OTA Highlight Paper Predicting Future Displacement of Nonoperatively Managed Lateral Compression Sacral Fractures - Can It Be DoneDocument6 pagesOTA Highlight Paper Predicting Future Displacement of Nonoperatively Managed Lateral Compression Sacral Fractures - Can It Be Doneakb601No ratings yet
- Artrosis Glenohumeral Despues de Artroscopia Bankart Repair A Long-Term Follow-Up of 13 YearsDocument6 pagesArtrosis Glenohumeral Despues de Artroscopia Bankart Repair A Long-Term Follow-Up of 13 Yearsmarcelogascon.oNo ratings yet
- 2016 Article 9341 PDFDocument8 pages2016 Article 9341 PDFJulenda CintarinovaNo ratings yet
- Necrosis Avascular de Humero Criterios de HertelDocument7 pagesNecrosis Avascular de Humero Criterios de Hertelluis perezNo ratings yet
- Acute Rockwood Type III ACJ Dislocation, Conservative Vs SurgicalDocument8 pagesAcute Rockwood Type III ACJ Dislocation, Conservative Vs SurgicalEdison MesacheNo ratings yet
- Computerized Medical Imaging and Graphics: Jianhua Yao, Joseph E. Burns, Hector Mu Noz, Ronald M. SummersDocument11 pagesComputerized Medical Imaging and Graphics: Jianhua Yao, Joseph E. Burns, Hector Mu Noz, Ronald M. SummersMasithaNo ratings yet
- 3D in Vivo Cervical Spine Kinematis: Preliminary Comparison of Fusion Patients and Control SubjectsDocument2 pages3D in Vivo Cervical Spine Kinematis: Preliminary Comparison of Fusion Patients and Control SubjectsAnthony OrtegaNo ratings yet
- Fracture of Distal RadiusDocument14 pagesFracture of Distal RadiusadibahNo ratings yet
- Stav SoucasnyDocument14 pagesStav SoucasnyTommysNo ratings yet
- (Journal of Neurosurgery - Pediatrics) Long-Term Motor Outcome Analysis Using A Motor Score Composite Following Surgical Brachial Plexus RepairDocument6 pages(Journal of Neurosurgery - Pediatrics) Long-Term Motor Outcome Analysis Using A Motor Score Composite Following Surgical Brachial Plexus RepairaliceNo ratings yet
- Open Reduction and Internal Fixation ORIF of ComplDocument6 pagesOpen Reduction and Internal Fixation ORIF of ComplAnnisa AnggrainiNo ratings yet
- Three-Dimensional Motion Analysis of The Cervical Spine For Comparison of Anterior Cervical Decompression and FusionDocument11 pagesThree-Dimensional Motion Analysis of The Cervical Spine For Comparison of Anterior Cervical Decompression and FusionLusiana PratiwiNo ratings yet
- Proximal Pole Scaphoid Fractures: A Computed Tomographic Assessment of OutcomesDocument5 pagesProximal Pole Scaphoid Fractures: A Computed Tomographic Assessment of OutcomesantoanetaNo ratings yet
- Reliability of Classification For Post Traumatic Ankle OsteoarthritisDocument6 pagesReliability of Classification For Post Traumatic Ankle OsteoarthritisDewi RoziqoNo ratings yet
- 3 Column AnkleDocument8 pages3 Column AnkleJosé Eduardo Fernandez RodriguezNo ratings yet
- A Galeazzi-Variant Type Fracture-Dislocation in Adults: Results: All Cases Were Followed Up For 24 Weeks. TheDocument3 pagesA Galeazzi-Variant Type Fracture-Dislocation in Adults: Results: All Cases Were Followed Up For 24 Weeks. TheTruly GracevaNo ratings yet
- Surgery of the Cranio-Vertebral JunctionFrom EverandSurgery of the Cranio-Vertebral JunctionEnrico TessitoreNo ratings yet
- What Exactly Are Period PantiesDocument2 pagesWhat Exactly Are Period PantiesJay Jay KamgaNo ratings yet
- Mission and VissionDocument11 pagesMission and VissionPradeep Kumar V PradiNo ratings yet
- Ranitidine + OndansetronDocument7 pagesRanitidine + OndansetronAllicia PutriNo ratings yet
- Buoyancy Calculation Report For 10INCH PipelineDocument7 pagesBuoyancy Calculation Report For 10INCH PipelineEmmanuel LawrenceNo ratings yet
- International Journal of Trend in Scientific Research and Development (IJTSRD)Document4 pagesInternational Journal of Trend in Scientific Research and Development (IJTSRD)Editor IJTSRDNo ratings yet
- CoC VampireCharacterPrimerPDFDocument5 pagesCoC VampireCharacterPrimerPDFDavid Alexander TomblinNo ratings yet
- Final Report On WaterproofingDocument35 pagesFinal Report On WaterproofingAlOk100% (2)
- May 2 Homework Solutions: S M X CDocument3 pagesMay 2 Homework Solutions: S M X CClerry SamuelNo ratings yet
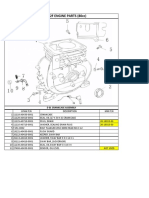
- Lifan 152F Engine Parts (80Cc) : E 01 Crankcase AssemblyDocument13 pagesLifan 152F Engine Parts (80Cc) : E 01 Crankcase AssemblySean MurrayNo ratings yet
- 1103-1104 RepairDocument120 pages1103-1104 RepairCristobal Sanchez91% (23)
- JSLHR Author InstructionsDocument14 pagesJSLHR Author InstructionsChanyanit CharoenpholNo ratings yet
- Batch Records HandoDocument39 pagesBatch Records HandoNiranjan SinghNo ratings yet
- Laboratory Manual For Microbiology Fundamentals A Clinical Approach 4Th Edition Susan Finazzo Full ChapterDocument51 pagesLaboratory Manual For Microbiology Fundamentals A Clinical Approach 4Th Edition Susan Finazzo Full Chapterlinda.ferguson121100% (7)
- EpidemiologyDocument26 pagesEpidemiologymohildasadiaNo ratings yet
- SyllabusDocument2 pagesSyllabusPrakash KumarNo ratings yet
- Benefits of SwimmingDocument3 pagesBenefits of Swimmingaybi pearlNo ratings yet
- Electrochemistry NotesDocument4 pagesElectrochemistry NotesAyush RorNo ratings yet
- Mini Dental ImplantsDocument11 pagesMini Dental ImplantsDario PuljićNo ratings yet
- Reading ComprehensionDocument9 pagesReading Comprehensionxifres i lletres xifres i lletres100% (1)
- Lab 5 - ReportDocument9 pagesLab 5 - ReportScarlet ErzaNo ratings yet
- Gastrointestinal Tract PDFDocument3 pagesGastrointestinal Tract PDFAlexandra Suan CatambingNo ratings yet
- ADPKDDocument75 pagesADPKDVenkataramanan KrishnamoorthyNo ratings yet
- PR Project - 3rd FinalDocument26 pagesPR Project - 3rd FinalLavish ChanodiaNo ratings yet
- ProposalDocument3 pagesProposalAbdullahAlmasNo ratings yet
- PGS 504 Notes Part IIDocument3 pagesPGS 504 Notes Part IISejal PriyaNo ratings yet
- QPD - Post-Discharge Follow-Up Phone Call Script SampleDocument3 pagesQPD - Post-Discharge Follow-Up Phone Call Script Samplejphinazee218No ratings yet
- Compact Water Treatment 200 m3Document3 pagesCompact Water Treatment 200 m3civil eng915No ratings yet
- FCA Problems RevisedDocument12 pagesFCA Problems RevisedRomelle Jane M. VelascoNo ratings yet
- Year Test - Ii: (Batch - A)Document11 pagesYear Test - Ii: (Batch - A)sachin sakuNo ratings yet
- 1978 - Behavior Analysis and Behavior Modification - Mallot, Tillema & Glenn PDFDocument499 pages1978 - Behavior Analysis and Behavior Modification - Mallot, Tillema & Glenn PDFKrusovice15No ratings yet