You might also like
- Khyber Pakhtunkhwa Health Sector Review: Hospital CareFrom EverandKhyber Pakhtunkhwa Health Sector Review: Hospital CareNo ratings yet
- 008-Method ABC-VEN (Sudan) Pharmaceutical Inventory Control in Sudan (2019)Document6 pages008-Method ABC-VEN (Sudan) Pharmaceutical Inventory Control in Sudan (2019)Grace MeldiNo ratings yet
- 5-Year Inventory Management of Drug Products in The Pharmacy Store in VietnamDocument9 pages5-Year Inventory Management of Drug Products in The Pharmacy Store in VietnamGrace MeldiNo ratings yet
- BS Inventory ClassificationDocument6 pagesBS Inventory ClassificationAshish BhardwajNo ratings yet
- Always, Better and Control - Vital, Essential, Desirable Matrix Analysis of The Drug Store of A Tertiary Care Teaching Hospital of North IndiaDocument5 pagesAlways, Better and Control - Vital, Essential, Desirable Matrix Analysis of The Drug Store of A Tertiary Care Teaching Hospital of North IndiababyNo ratings yet
- Inventory Control Techniques in Medical StoresDocument9 pagesInventory Control Techniques in Medical StoresJasmeetsingh09No ratings yet
- LR 9Document4 pagesLR 9Raviraj KambleNo ratings yet
- Analysis of Pharmaceutical Inventory (2023)Document6 pagesAnalysis of Pharmaceutical Inventory (2023)Grace MeldiNo ratings yet
- Medical Store Management: An Integrated Economic Analysis of A Tertiary Care Hospital in Central IndiaDocument6 pagesMedical Store Management: An Integrated Economic Analysis of A Tertiary Care Hospital in Central IndiaSanjeev ChouguleNo ratings yet
- ABC and VED Analysis of The Pharmacy Store of A Tertiary Care Teaching, Research and Referral Healthcare Institute of IndiaDocument5 pagesABC and VED Analysis of The Pharmacy Store of A Tertiary Care Teaching, Research and Referral Healthcare Institute of IndiaManprita BasumataryNo ratings yet
- Sajc VypinDocument6 pagesSajc VypinVidya JhaNo ratings yet
- Evaluation of Pharmaceutical InventoryDocument16 pagesEvaluation of Pharmaceutical Inventorynanguh2004No ratings yet
- JYPharm 4 114Document6 pagesJYPharm 4 114awasthypranshuNo ratings yet
- Health 2013011116024790Document6 pagesHealth 2013011116024790Ehlpuffin Twenty8No ratings yet
- LR 4Document6 pagesLR 4Raviraj KambleNo ratings yet
- Abc and Ved Analyses of Free Drug Store in Drug and Pharmacy of Skims - A Tertiary Care Institute in Jammu and Kashmir, IndiaDocument8 pagesAbc and Ved Analyses of Free Drug Store in Drug and Pharmacy of Skims - A Tertiary Care Institute in Jammu and Kashmir, IndiaTJPRC PublicationsNo ratings yet
- Chapter For DianaDocument8 pagesChapter For Dianageorgeodhiambo840No ratings yet
- The Need For Pharmaceutical Care in An Intensive Care Unit at A Teaching Hospital in South AfricaDocument4 pagesThe Need For Pharmaceutical Care in An Intensive Care Unit at A Teaching Hospital in South AfricaAdibaNo ratings yet
- Demand in Health Care AnalysisDocument9 pagesDemand in Health Care AnalysisZewdu MinwuyeletNo ratings yet
- Healthcare DoDocument9 pagesHealthcare Doseife slassieNo ratings yet
- Continence AuditDocument6 pagesContinence Auditi can always make u smile :DNo ratings yet
- Health Care Waste Management in Two National Hospitals KenyaDocument6 pagesHealth Care Waste Management in Two National Hospitals KenyaFrancis Njihia KaburuNo ratings yet
- LR 8Document13 pagesLR 8Raviraj KambleNo ratings yet
- Factors Associated With The Ineffectiveness of Epidemiological Surveillance in The Health Districts of The South Cameroon RegionDocument9 pagesFactors Associated With The Ineffectiveness of Epidemiological Surveillance in The Health Districts of The South Cameroon RegionInternational Journal of Recent Innovations in Academic ResearchNo ratings yet
- Auditable Pharmaceutical Transaction and Service (APTS)Document11 pagesAuditable Pharmaceutical Transaction and Service (APTS)Abdi67% (3)
- J. Pharm. Biomed. Sci., 1 (6) 113-119, 2011Document7 pagesJ. Pharm. Biomed. Sci., 1 (6) 113-119, 2011Hanim MafulahNo ratings yet
- Effect of Inventory Management PracticesDocument12 pagesEffect of Inventory Management PracticesAddis TadesseNo ratings yet
- Utilization of Routine Health Data in Decision-Making by Management Teams in Selected Level 4 Hospitals in Nakuru County, KenyaDocument27 pagesUtilization of Routine Health Data in Decision-Making by Management Teams in Selected Level 4 Hospitals in Nakuru County, KenyathabitisadruNo ratings yet
- WHO Point Prevalence Survey To Describe The Use of Antimicrobials at A Tertiary Care Center in Pakistan - A Situation Analysis For Establishing An Antimicrobial Stewardship Program - PMCDocument18 pagesWHO Point Prevalence Survey To Describe The Use of Antimicrobials at A Tertiary Care Center in Pakistan - A Situation Analysis For Establishing An Antimicrobial Stewardship Program - PMCAbubakr AurangzebNo ratings yet
- Satisfaction of Nigerian Patients With Health Services: A Protocol For A Systematic ReviewDocument6 pagesSatisfaction of Nigerian Patients With Health Services: A Protocol For A Systematic Reviewsopha seyhaNo ratings yet
- Health Financing For Universal HealthDocument9 pagesHealth Financing For Universal HealthMirani BarrosNo ratings yet
- Ricky Felix Kwayi ReportDocument16 pagesRicky Felix Kwayi ReportmogreyNo ratings yet
- BMC Health Services Research: Choice of Healthcare Provider Following Reform in VietnamDocument9 pagesBMC Health Services Research: Choice of Healthcare Provider Following Reform in VietnamjlventiganNo ratings yet
- Drug Inventory ControlDocument5 pagesDrug Inventory ControlFetty NuzuliyahNo ratings yet
- Health-Seeking Behaviour and Health Outcome Among Uninsured Patients Attending A Primary Care Clinic of A Teaching Hospital in Southwestern NigeriaDocument7 pagesHealth-Seeking Behaviour and Health Outcome Among Uninsured Patients Attending A Primary Care Clinic of A Teaching Hospital in Southwestern NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Inventory Management Using Matrix Analysis and Inventory Index in An Oncology Pharmacy of A Tertiary Care Teaching HospitalDocument5 pagesInventory Management Using Matrix Analysis and Inventory Index in An Oncology Pharmacy of A Tertiary Care Teaching HospitalChrist GreatoNo ratings yet
- Evaluation of Outpatient Antibiotic Use in Beijing General Hospitals in 2015Document9 pagesEvaluation of Outpatient Antibiotic Use in Beijing General Hospitals in 2015UdtjeVanDerJeykNo ratings yet
- Editorial: Ethics in Biomedical Research C. RavindranDocument4 pagesEditorial: Ethics in Biomedical Research C. RavindranSudhakar DasariNo ratings yet
- Critical Analysis of Pharmaceuticals Inventory Management Using The ABC-VEN Matrix in Dessie Referral Hospital, EthiopiaDocument14 pagesCritical Analysis of Pharmaceuticals Inventory Management Using The ABC-VEN Matrix in Dessie Referral Hospital, EthiopiaGrace MeldiNo ratings yet
- Use of Medicine Pricing and Reimbursement Policies For Universal Health Coverage in IndonesiaDocument19 pagesUse of Medicine Pricing and Reimbursement Policies For Universal Health Coverage in IndonesiaAde IlmiNo ratings yet
- Impact of Public Procurement Policies and Procedures On The Health Delivery System in Zimbabwe: Chitungwiza Central HospitalDocument61 pagesImpact of Public Procurement Policies and Procedures On The Health Delivery System in Zimbabwe: Chitungwiza Central Hospitalnyeked6618100% (10)
- Jyp 7 2 4 1Document8 pagesJyp 7 2 4 1Duy ThắngNo ratings yet
- ABC - Ved AnalysisDocument6 pagesABC - Ved AnalysisFatimahNo ratings yet
- 2020-02-23 AWaRe - 2020 - PaperDraft - V17Document27 pages2020-02-23 AWaRe - 2020 - PaperDraft - V17Laurent UlrichNo ratings yet
- Analisis Minimalisasi Biaya (CMA)Document7 pagesAnalisis Minimalisasi Biaya (CMA)diahsaharaNo ratings yet
- 2020 Article 5771Document11 pages2020 Article 5771Nindie AulhieyaNo ratings yet
- Manuscript Draft 4Document22 pagesManuscript Draft 4Maganga ShimbiNo ratings yet
- LR 1 2012Document5 pagesLR 1 2012Raviraj KambleNo ratings yet
- ABC-VEN Matrix AnalysisDocument11 pagesABC-VEN Matrix AnalysisAndrés PáezNo ratings yet
- Factors Associated With Irrational Drug Use at A District Hospital in Zambia: Patient Record-Based ObservationsDocument6 pagesFactors Associated With Irrational Drug Use at A District Hospital in Zambia: Patient Record-Based ObservationsKevin SaulNo ratings yet
- Article 7yCODocument11 pagesArticle 7yCOAychluhm TatekNo ratings yet
- Mr. Hariom Rajput Mr. Ramsingh Ji Gmail-ID International Association of Oncology (IAO) Government of IndiaDocument6 pagesMr. Hariom Rajput Mr. Ramsingh Ji Gmail-ID International Association of Oncology (IAO) Government of IndiaHariom RajputNo ratings yet
- ABC Ved MatrixDocument9 pagesABC Ved MatrixZia AbidiNo ratings yet
- 359 ArticleText 1540 1 10 20201228Document7 pages359 ArticleText 1540 1 10 20201228Aidy StarkNo ratings yet
- Benefits - and - Challenges - of - Ele 6Document7 pagesBenefits - and - Challenges - of - Ele 6silfianaNo ratings yet
- 02 Factors Influencing Community Pharmacists' Recommendation of Over-The-counter Medications in Four Vietnam CitiesDocument7 pages02 Factors Influencing Community Pharmacists' Recommendation of Over-The-counter Medications in Four Vietnam CitiesTrần Văn ĐệNo ratings yet
- 1 s2.0 S1319016421001407 MainDocument8 pages1 s2.0 S1319016421001407 MainarafathNo ratings yet
- Analysis of Antibiotic Consumption by Aware Classi Fication in Shandong Province, China, 2012 - 2019: A Panel Data AnalysisDocument8 pagesAnalysis of Antibiotic Consumption by Aware Classi Fication in Shandong Province, China, 2012 - 2019: A Panel Data AnalysisBBD BBDNo ratings yet
- A Closed Loop Two Cycle Audit Assessing The Prescription Practice of Topical Antibiotics For Acute Infective Conjunctivitis in A Primary Care DepartmentDocument6 pagesA Closed Loop Two Cycle Audit Assessing The Prescription Practice of Topical Antibiotics For Acute Infective Conjunctivitis in A Primary Care DepartmentAthenaeum Scientific PublishersNo ratings yet
- International Journal of Pharmacy Practice AbstractsDocument40 pagesInternational Journal of Pharmacy Practice AbstractsFabiola NogaNo ratings yet
- Taller Sobre Preposiciones y Vocabulario - Exhibición Comercial SergioDocument5 pagesTaller Sobre Preposiciones y Vocabulario - Exhibición Comercial SergioYovanny Peña Pinzon100% (2)
- 1.2 Installation of SSH Keys On Linux-A Step-By Step GuideDocument3 pages1.2 Installation of SSH Keys On Linux-A Step-By Step GuideMada ChouchouNo ratings yet
- DPWH Cost EstimationDocument67 pagesDPWH Cost EstimationAj Abe92% (12)
- Introduction and Instructions: ForewordDocument20 pagesIntroduction and Instructions: ForewordDanang WidoyokoNo ratings yet
- Revamping An Integrated Hydrocracker and Lube Base Oil UnitDocument5 pagesRevamping An Integrated Hydrocracker and Lube Base Oil UnitVyacheslavNo ratings yet
- Job Description: Extensive ReadingDocument12 pagesJob Description: Extensive ReadingNatalia VivonaNo ratings yet
- Scrum Gantt Chart With BurndownDocument4 pagesScrum Gantt Chart With BurndownAsma Afreen ChowdaryNo ratings yet
- COMPLAINT - THE STAN J. CATERBONE 42 U.S.C. 14141 "POLICE MISCONDUCT PROVISION" COMPLAINT TO U.S. DEPARTMENT OF JUSTICE August 24, 2017Document435 pagesCOMPLAINT - THE STAN J. CATERBONE 42 U.S.C. 14141 "POLICE MISCONDUCT PROVISION" COMPLAINT TO U.S. DEPARTMENT OF JUSTICE August 24, 2017Stan J. CaterboneNo ratings yet
- Managerial Economics - 1Document36 pagesManagerial Economics - 1Deepi SinghNo ratings yet
- Allergies To Cross-Reactive Plant Proteins: Takeshi YagamiDocument11 pagesAllergies To Cross-Reactive Plant Proteins: Takeshi YagamisoylahijadeunvampiroNo ratings yet
- ETA-1 Service PDFDocument44 pagesETA-1 Service PDFgansolNo ratings yet
- Tarlac - San Antonio - Business Permit - NewDocument2 pagesTarlac - San Antonio - Business Permit - Newarjhay llave100% (1)
- Logbook) Industrial Attachment Brief To Students-3Document6 pagesLogbook) Industrial Attachment Brief To Students-3geybor100% (1)
- Central Bureau of Investigation ManualDocument2 pagesCentral Bureau of Investigation Manualcsudha38% (13)
- Roundup WG Bula MonsantoDocument16 pagesRoundup WG Bula MonsantodandanyddNo ratings yet
- Zone Controller: Th-LargeDocument1 pageZone Controller: Th-LargeIsmat AraNo ratings yet
- SecureCore Datasheet V2Document2 pagesSecureCore Datasheet V2chepogaviriaf83No ratings yet
- Inv69116728 45926324Document1 pageInv69116728 45926324dany.cantaragiuNo ratings yet
- Class B Digital Device Part 15 of The FCC RulesDocument7 pagesClass B Digital Device Part 15 of The FCC RulesHemantkumarNo ratings yet
- Pub 005940 PDFDocument31 pagesPub 005940 PDFkurniaNo ratings yet
- Fouzia AnjumDocument3 pagesFouzia AnjumAbdul SyedNo ratings yet
- Lecture Notes (Financial Economics)Document136 pagesLecture Notes (Financial Economics)americus_smile7474100% (2)
- Hortors Online ManualDocument11 pagesHortors Online Manualtshepang4228No ratings yet
- წყალტუბოს - სპა კურორტის განვითარების გეგმაDocument16 pagesწყალტუბოს - სპა კურორტის განვითარების გეგმაReginfoNo ratings yet
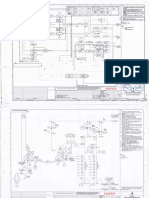
- Attachment 05 - BFD, ELD and P&I Diagrams-PearlDocument77 pagesAttachment 05 - BFD, ELD and P&I Diagrams-Pearlum er100% (1)
- Goat Farm ProjectDocument44 pagesGoat Farm ProjectVipin Kushwaha83% (6)
- Analisis Dan Perbandingan Jaringan Wifi Dengan Frekuensi 2.4 GHZ Dan 5 GHZ Dengan Metode QosDocument19 pagesAnalisis Dan Perbandingan Jaringan Wifi Dengan Frekuensi 2.4 GHZ Dan 5 GHZ Dengan Metode QosNoltujuh Nollapan (Congyang)No ratings yet
- Teacher Planner 2023 PDFDocument52 pagesTeacher Planner 2023 PDFitaNo ratings yet
- SAN MIGUEL CORPORATION, ANGEL G. ROA and MELINDA MACARAIG, vs. NATIONAL LABOR RELATIONS COMMISSION (Second Division), LABOR ARBITER EDUARDO J. CARPIO, ILAW AT BUKLOD NG MANGGAGAWA (IBM), ET ALDocument6 pagesSAN MIGUEL CORPORATION, ANGEL G. ROA and MELINDA MACARAIG, vs. NATIONAL LABOR RELATIONS COMMISSION (Second Division), LABOR ARBITER EDUARDO J. CARPIO, ILAW AT BUKLOD NG MANGGAGAWA (IBM), ET ALLaila Ismael SalisaNo ratings yet
- Ultra Wideband TechnologyDocument21 pagesUltra Wideband TechnologyAzazelNo ratings yet