You might also like
- General Chemistry I Syllabus: Course InformationDocument4 pagesGeneral Chemistry I Syllabus: Course InformationSierra Skye MuganNo ratings yet
- CHEM 1004 Lab Schedule and Safety GuideDocument11 pagesCHEM 1004 Lab Schedule and Safety GuideGrant NilsonNo ratings yet
- Chem 124 SyllabusDocument4 pagesChem 124 SyllabuscuriousbookwormNo ratings yet
- CHM 2046L Syllabus-Fall 2014Document6 pagesCHM 2046L Syllabus-Fall 2014Amira CatoNo ratings yet
- Pain Medication Module Focuses on AnalgesicsDocument9 pagesPain Medication Module Focuses on AnalgesicsSheril MarekNo ratings yet
- Bronchial AsthmaDocument20 pagesBronchial AsthmaJuliet De GuzmanNo ratings yet
- Chem Lab ManualDocument64 pagesChem Lab ManualNiko PalNo ratings yet
- Nursing Flash CardsDocument5 pagesNursing Flash CardsJan Clarisse RamosNo ratings yet
- Seidel's Guide To Physical Examination, Chapter 16, 350-369 PDFDocument20 pagesSeidel's Guide To Physical Examination, Chapter 16, 350-369 PDFAlexandra PalagaNo ratings yet
- Internal MedicineDocument168 pagesInternal Medicinebolt boltNo ratings yet
- ManualDocument64 pagesManualBasil CorianderNo ratings yet
- Inicet Cbt1 Answer Sheet 2022v2Document137 pagesInicet Cbt1 Answer Sheet 2022v2Aakash SethiNo ratings yet
- Pharmacology of Heparin and Related Drugs: An UpdateDocument105 pagesPharmacology of Heparin and Related Drugs: An Updaterodcam1No ratings yet
- Ela Divisional Clinical Examination Purpose and RubricDocument9 pagesEla Divisional Clinical Examination Purpose and RubricKhuslen BatmandakhNo ratings yet
- A Systematic Review On Dementia CareDocument5 pagesA Systematic Review On Dementia CareInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Concept Map Aplastic Anemia 212 1Document1 pageConcept Map Aplastic Anemia 212 1S AustinNo ratings yet
- Drugs Affecting The Male and Female Reproductive SystemDocument24 pagesDrugs Affecting The Male and Female Reproductive SystemAngelica Pabello100% (2)
- RN NotesDocument119 pagesRN NotesJingyu SheNo ratings yet
- Assessment of Activities of Daily Living in Patients Post COVID-19: A Systematic ReviewDocument18 pagesAssessment of Activities of Daily Living in Patients Post COVID-19: A Systematic Reviewjavieron11No ratings yet
- Test Bank For Pharmacological Aspects of Nursing Care 7th Edition by BroylesDocument10 pagesTest Bank For Pharmacological Aspects of Nursing Care 7th Edition by Broylesa759488023No ratings yet
- Evidence Based Practice 1Document40 pagesEvidence Based Practice 1zeinabNo ratings yet
- Www.way2freshers.comDocument35 pagesWww.way2freshers.comsreenivasNo ratings yet
- QuestionDocument17 pagesQuestionAccey RamirezNo ratings yet
- Group 27 Day Care Duty Case StudyDocument14 pagesGroup 27 Day Care Duty Case StudyRaul GuzmanNo ratings yet
- Chronic care management goals for diabetes, hypertension, hyperlipidemiaDocument14 pagesChronic care management goals for diabetes, hypertension, hyperlipidemiaJuancho RiveraNo ratings yet
- Glucose TestingDocument5 pagesGlucose TestingMoira Julianne Serognas BrigoliNo ratings yet
- Nursing Assessment ToolDocument6 pagesNursing Assessment ToolRaniNo ratings yet
- College Final Paper 1Document6 pagesCollege Final Paper 1Rita PrinceNo ratings yet
- Ferguson 2014Document18 pagesFerguson 2014bordian georgeNo ratings yet
- Clinical Radiology Handbook v1.0Document162 pagesClinical Radiology Handbook v1.0Zulqarnain AbidNo ratings yet
- Anaesthetic Management of Posterior Mediastinal Mass in A Child. Case ReportDocument3 pagesAnaesthetic Management of Posterior Mediastinal Mass in A Child. Case ReporttcsariNo ratings yet
- Clinical Epidemiology DKA NOTESDocument22 pagesClinical Epidemiology DKA NOTESTris100% (1)
- Pain MedicationsDocument2 pagesPain MedicationsimirelaNo ratings yet
- Upper Limb Neurological Examination OSCE GuideDocument15 pagesUpper Limb Neurological Examination OSCE GuideLeen abusarhanNo ratings yet
- TCAR ManualDocument193 pagesTCAR ManualJoe Reed (Game Master)No ratings yet
- Fetal Heart TonesDocument1 pageFetal Heart TonesChristian Clyde N. JakosalemNo ratings yet
- UPump Pediatric NursingDocument21 pagesUPump Pediatric NursingJan Leslie VergaraNo ratings yet
- 2 History Is Not His StoryDocument424 pages2 History Is Not His StorydrsourabhsinghNo ratings yet
- Ivfluid Glines AdultDocument2 pagesIvfluid Glines AdultDilan Galary100% (1)
- Grammar clausesDocument48 pagesGrammar clausesPhan Xuân Yến NhiNo ratings yet
- Workbook On IV TherapyDocument24 pagesWorkbook On IV TherapyFATIMA MARYAMA USMANNo ratings yet
- StandardsDocument7 pagesStandardsHannah DuyagNo ratings yet
- Ati Reading Teas Final Study GuideDocument29 pagesAti Reading Teas Final Study GuideMmmm LlllNo ratings yet
- Nursing Care of Child With Thalassemia and LeukemiaDocument60 pagesNursing Care of Child With Thalassemia and LeukemiaJanicex FongNo ratings yet
- Iv Therapy With Edited RationaleDocument5 pagesIv Therapy With Edited RationaleKysha HuangNo ratings yet
- National TB ProgramDocument34 pagesNational TB ProgramASTR4 BABY100% (1)
- Normal Laboratory Values With Nursing Consideration - UsnganDocument8 pagesNormal Laboratory Values With Nursing Consideration - UsnganPrincess Nasima M. UsnganNo ratings yet
- Professional Skills Review Central Nervous System (CNS)Document25 pagesProfessional Skills Review Central Nervous System (CNS)Noora AlmuailiNo ratings yet
- Burnout Nurses: Concept PaperDocument3 pagesBurnout Nurses: Concept PaperdfgerbrcNo ratings yet
- PsychaitryDocument421 pagesPsychaitrylaraib emadNo ratings yet
- General Surgery Manual for Medical StudentsDocument381 pagesGeneral Surgery Manual for Medical StudentsRAZAANo ratings yet
- Family Medicine Clerkship EssentialsDocument17 pagesFamily Medicine Clerkship EssentialsjhhjjhNo ratings yet
- Common Medical AbbreviationsDocument78 pagesCommon Medical AbbreviationsRAISA N. RASIDNo ratings yet
- Student Activity - Nervous SystemDocument4 pagesStudent Activity - Nervous SystemSeth Khalil LardausNo ratings yet
- TFN Case ScenarioDocument13 pagesTFN Case ScenarioDUQUE, GEORGETTE FLOREANNE L.No ratings yet
- Assessing Physical HealthDocument41 pagesAssessing Physical HealthJaden QuimsonNo ratings yet
- 14 Steps To A Healthy LifestyleDocument3 pages14 Steps To A Healthy LifestyleLuise MauieNo ratings yet
- SuturingDocument89 pagesSuturingD YasIr Mussa100% (1)
- SUTURES AND SUTURING TECHNIQUES (Class)Document65 pagesSUTURES AND SUTURING TECHNIQUES (Class)Archana100% (4)
- Everything You Need to Know About Sutures and Suturing TechniquesDocument65 pagesEverything You Need to Know About Sutures and Suturing TechniquesRicha Bhosale100% (2)
- Nursing Procedure Checklist: Suctioning An Endotracheal Tube: Open SystemDocument2 pagesNursing Procedure Checklist: Suctioning An Endotracheal Tube: Open Systemmark OrpillaNo ratings yet
- Instillation of Eye MedicationDocument2 pagesInstillation of Eye MedicationissaiahnicolleNo ratings yet
- Materi 2 - ICS & HDP - Covid19Document21 pagesMateri 2 - ICS & HDP - Covid19devie apriliyantiNo ratings yet
- Edhi Foundation: M. Qasim Butt Babar Saadat C.J. Danyaal Bin RazaDocument20 pagesEdhi Foundation: M. Qasim Butt Babar Saadat C.J. Danyaal Bin RazaSyed ArslanNo ratings yet
- Tablet Manufacturing ProcessDocument8 pagesTablet Manufacturing ProcessNaveen KingNo ratings yet
- AHDP - Teenage Pregnancy NewDocument20 pagesAHDP - Teenage Pregnancy NewEdisa AsuncionNo ratings yet
- Histopathological and Immunohistochemical Study of The Polyserositis in Buffalo (Bubalus Bubalis)Document6 pagesHistopathological and Immunohistochemical Study of The Polyserositis in Buffalo (Bubalus Bubalis)ticianaNo ratings yet
- Medical Pro Form ADocument8 pagesMedical Pro Form ASamar SinghNo ratings yet
- 1 Making Occlusion - TerminologyDocument7 pages1 Making Occlusion - TerminologyAli QawasNo ratings yet
- Session PlanDocument9 pagesSession PlanKirsten Q. CaminongNo ratings yet
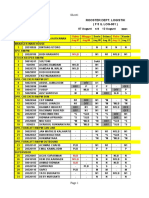
- Update Stok 05 Juli 2023Document8 pagesUpdate Stok 05 Juli 2023Lulut Hening PrasetyoNo ratings yet
- Ingles CuadroDocument6 pagesIngles Cuadroyemiliana aldanaNo ratings yet
- BHP Dan Obat Preputium-1Document2 pagesBHP Dan Obat Preputium-1Sayed Saiful WajirNo ratings yet
- G1P0, Placenta Previa: Discharge Plan DietDocument7 pagesG1P0, Placenta Previa: Discharge Plan DietRap De la CruzNo ratings yet
- Initial Efficacy and Tolerability of Early Enteral Nutrition With Immediate or Gradual Introduction in Intubated PatientsDocument6 pagesInitial Efficacy and Tolerability of Early Enteral Nutrition With Immediate or Gradual Introduction in Intubated PatientsUCI COVID Pediátrico HNGAINo ratings yet
- Dengue RachelDocument5 pagesDengue Rachellara candilosasNo ratings yet
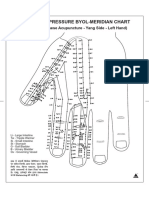
- Byol Maridian ChartDocument2 pagesByol Maridian ChartPranicHealingCentre63% (8)
- Sherlyn Pablo-Pablo - Rough DraftDocument4 pagesSherlyn Pablo-Pablo - Rough Draftapi-663260468No ratings yet
- Name Course DateDocument215 pagesName Course DateAdam RaynardNo ratings yet
- Tes Evaluasi - News Item TextDocument5 pagesTes Evaluasi - News Item TextSheyla PutriNo ratings yet
- Konsep Dasar, Optimalisasi, Dan Teknik Pengurangan Dosis Pada Pesawat CT ScanDocument31 pagesKonsep Dasar, Optimalisasi, Dan Teknik Pengurangan Dosis Pada Pesawat CT Scanrifqi anisaNo ratings yet
- JessaDocument4 pagesJessaRC CouponNo ratings yet
- Weekly Staff Schedule Sheet 1Document10 pagesWeekly Staff Schedule Sheet 1dywhenx papahrocknslowNo ratings yet
- Beckman Coulter PK TP Feb2012Document16 pagesBeckman Coulter PK TP Feb2012Inês LoboNo ratings yet
- Sediaan Oral Modified Release (Modified Release Delivery System)Document54 pagesSediaan Oral Modified Release (Modified Release Delivery System)Dwi Amalia husnaNo ratings yet
- Aconite PoisoningDocument15 pagesAconite PoisoningShagun TyagiNo ratings yet
- National University: College of ArchitectureDocument23 pagesNational University: College of ArchitectureAbygail MorenoNo ratings yet
- Aa Equipments and SuppliesDocument10 pagesAa Equipments and SuppliesAkshata BansodeNo ratings yet
- A Splitting of The MindDocument218 pagesA Splitting of The Mindapi-285617305No ratings yet
- Boq Medical Services Obs™ PDFDocument3 pagesBoq Medical Services Obs™ PDFKyle Levic SalaguintoNo ratings yet