You might also like
- Spinal Anaesthesia - Wikipedia, The Free EncyclopediaDocument4 pagesSpinal Anaesthesia - Wikipedia, The Free EncyclopediafujiNo ratings yet
- WFSAQ Labor Epidural - TroubleshootingDocument6 pagesWFSAQ Labor Epidural - TroubleshootingJaysonNo ratings yet
- Spinal AnaesthesiaDocument4 pagesSpinal Anaesthesiawasis wibowoNo ratings yet
- Regional Anesthesia and Eye SurgeryDocument7 pagesRegional Anesthesia and Eye SurgeryharumNo ratings yet
- Caudal Epidural InjectionDocument6 pagesCaudal Epidural InjectionRS BaptisNo ratings yet
- Fvets 04 00068Document12 pagesFvets 04 00068Didit HarysNo ratings yet
- 2.4 Regional AnesthesiaDocument6 pages2.4 Regional AnesthesiaLA BriguelaNo ratings yet
- Anaesthetic Considerations For Strabismus Surgery in Children and AdultsDocument12 pagesAnaesthetic Considerations For Strabismus Surgery in Children and AdultschdoankNo ratings yet
- Everything You Need to Know About Adhesive ArachnoiditisDocument8 pagesEverything You Need to Know About Adhesive ArachnoiditisStaporn KasemsripitakNo ratings yet
- Right Open Nephrectomy Under Combined Spinal and Peridural Operative Anesthesia and Analgesia (CSE) : A New Anesthetic Approach in Abdominal SurgeryDocument2 pagesRight Open Nephrectomy Under Combined Spinal and Peridural Operative Anesthesia and Analgesia (CSE) : A New Anesthetic Approach in Abdominal SurgeryPablo Segales BautistaNo ratings yet
- Sedation in The IcuDocument4 pagesSedation in The Icuprashsubbu100% (1)
- Articulo AnestesiaDocument36 pagesArticulo Anestesianavarrog90No ratings yet
- Fluoroscopy-Guided Periradicular Injections in SpineDocument8 pagesFluoroscopy-Guided Periradicular Injections in SpineAlvaro Perez HenriquezNo ratings yet
- Make Anesthesia EasyDocument47 pagesMake Anesthesia EasyRonika LepchaNo ratings yet
- Nabalde, Juana A - ReportDocument7 pagesNabalde, Juana A - ReportJuana Ablay NabaldeNo ratings yet
- Airway Management in Neurological PatientsDocument22 pagesAirway Management in Neurological PatientsReza ManefoNo ratings yet
- Workshop C 7Document14 pagesWorkshop C 7DellNo ratings yet
- New Epidural ProtocolDocument16 pagesNew Epidural ProtocolAndreea OanaNo ratings yet
- Akinosi (Tuberosity) Technique A Verity But Under-UtilisedDocument3 pagesAkinosi (Tuberosity) Technique A Verity But Under-UtilisedJorge López CaNo ratings yet
- ps03bp 2013 Guidelines For The Management of Major Regional Analgesia Background PaperDocument5 pagesps03bp 2013 Guidelines For The Management of Major Regional Analgesia Background PaperJane KoNo ratings yet
- HidrodiseksiDocument5 pagesHidrodiseksiRahmania Noor AdibaNo ratings yet
- Baru 2Document12 pagesBaru 2Bianca CaterinalisendraNo ratings yet
- Cervical Epidural For Total Thyroidectomy in A Patient With Large Thyroid Nodule With Retrosternal Extension With Superior Vena Caval Compression SyndromeDocument2 pagesCervical Epidural For Total Thyroidectomy in A Patient With Large Thyroid Nodule With Retrosternal Extension With Superior Vena Caval Compression SyndromeInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Irwan Lapsus Anest Siap 2Document2 pagesIrwan Lapsus Anest Siap 2Ade Irwan SuryadiNo ratings yet
- Segmental Spinal Anesthesia A Systematic ReviewDocument6 pagesSegmental Spinal Anesthesia A Systematic Reviewجعفر محمدNo ratings yet
- Cobb - Endoscopic Carpal Tunnel ReleaseDocument8 pagesCobb - Endoscopic Carpal Tunnel ReleaseJohnny WangNo ratings yet
- 1-s2.0-S1748681523006885-mainDocument2 pages1-s2.0-S1748681523006885-mainAlexandreNo ratings yet
- Tehnici de AnestezieDocument18 pagesTehnici de AnestezieMacsuta VladNo ratings yet
- IAN injury implant dentistry diagnosis causes prevention managementDocument7 pagesIAN injury implant dentistry diagnosis causes prevention managementmaxNo ratings yet
- AnesthesiaDocument54 pagesAnesthesiaNURDINI BINTI ZAMRI MoeNo ratings yet
- Evolution of The Surgical Management of Cauda Equina SyndromeDocument13 pagesEvolution of The Surgical Management of Cauda Equina SyndromeAtul JainNo ratings yet
- Working in A Hospital's Neurointensive Care Unit Treat Patients Suffering From Everything From Stroke To Traumatic Brain InjuriesDocument5 pagesWorking in A Hospital's Neurointensive Care Unit Treat Patients Suffering From Everything From Stroke To Traumatic Brain InjuriesRichlle CortesNo ratings yet
- Documento PDFDocument17 pagesDocumento PDFJose Miguel CastellonNo ratings yet
- Sign up to receive weekly ultrasound guided interscalene block tutorialsDocument10 pagesSign up to receive weekly ultrasound guided interscalene block tutorialsAnesthesiology FKUBNo ratings yet
- Introduction To AnaesthesiaDocument5 pagesIntroduction To AnaesthesiaAndrew CheongNo ratings yet
- 1-s2.0-S1878875018300159-mainDocument9 pages1-s2.0-S1878875018300159-mainAlexandreNo ratings yet
- Awake Craniotomy Anaesthesia GuideDocument7 pagesAwake Craniotomy Anaesthesia GuidePablo Sousa CasasnovasNo ratings yet
- Fneur 13 880814Document18 pagesFneur 13 880814Generation GenerationNo ratings yet
- Bilateral Bi-Level Erector Spinae Plane Blocks as a Part of Opioid-Sparing Multimodal Analgesia in Scoliosis Surgery: A Case Series of Six Pediatric PatientsDocument8 pagesBilateral Bi-Level Erector Spinae Plane Blocks as a Part of Opioid-Sparing Multimodal Analgesia in Scoliosis Surgery: A Case Series of Six Pediatric PatientsLetíciaNo ratings yet
- Ultrasound-Guided Fascial PlaneDocument19 pagesUltrasound-Guided Fascial PlaneEnano Narigudo TresNo ratings yet
- Combined Spinal Epidural Anesthesia and Analgesia: March 2012Document21 pagesCombined Spinal Epidural Anesthesia and Analgesia: March 2012Elaine LaizaNo ratings yet
- Risk of Nerve Injury After Spinal or Epidural InjectionDocument5 pagesRisk of Nerve Injury After Spinal or Epidural Injectionstarlette.haraNo ratings yet
- CombinedDocument3 pagesCombinedSolape Akin-WilliamsNo ratings yet
- VASG Epidural InjectionsDocument3 pagesVASG Epidural InjectionsAnaNo ratings yet
- Scalp Block and Cervical Plexus Block Techniques - UpToDateDocument28 pagesScalp Block and Cervical Plexus Block Techniques - UpToDateAna Belén Artero CastañoNo ratings yet
- 14Document10 pages14Juliana ObandoNo ratings yet
- Regional anaesthesia for ophthalmic surgeryDocument7 pagesRegional anaesthesia for ophthalmic surgeryirvan rahmanNo ratings yet
- Anaesthesia Introdection: Anesthetist DutyDocument13 pagesAnaesthesia Introdection: Anesthetist DutyHaider Nadhem AL-rubaiNo ratings yet
- An_Update_on_Treatment_Modalities_for_Ulnar_Nerve_Document7 pagesAn_Update_on_Treatment_Modalities_for_Ulnar_Nerve_kusumaningrum072No ratings yet
- Apm 20050Document6 pagesApm 20050hnzzn2bymdNo ratings yet
- Ch09 AnaestheticsDocument21 pagesCh09 AnaestheticsDonna MitchellNo ratings yet
- Surgical Removal of Spinal Cord TumorsDocument8 pagesSurgical Removal of Spinal Cord TumorsLuwiNo ratings yet
- Volatile Anaesthetics in IcuDocument4 pagesVolatile Anaesthetics in IcuSrinivas PingaliNo ratings yet
- Anestesi Jurnal 2Document11 pagesAnestesi Jurnal 2dewi rahmanNo ratings yet
- Anesthesia and TypesDocument6 pagesAnesthesia and TypesKat PerezNo ratings yet
- Anaesthesia - 2009 - Danelli - Ultrasound Vs Nerve Stimulation Multiple Injection Technique For Posterior Popliteal SciaticDocument5 pagesAnaesthesia - 2009 - Danelli - Ultrasound Vs Nerve Stimulation Multiple Injection Technique For Posterior Popliteal SciaticRama BayuNo ratings yet
- Bedah Buku InstrumenDocument12 pagesBedah Buku Instrumencoffe latteNo ratings yet
- Maronge Et Al-2018-AnaesthesiaDocument6 pagesMaronge Et Al-2018-AnaesthesiadefitranandaNo ratings yet
- Ultrasound and clinically guided Injection techniques on the musculoskeletal systemFrom EverandUltrasound and clinically guided Injection techniques on the musculoskeletal systemNo ratings yet
- Diagnosis and Treatment of Neurogenic Oropharyngeal DysphagiaFrom EverandDiagnosis and Treatment of Neurogenic Oropharyngeal DysphagiaNo ratings yet
- Membandingkan Recall 24 Jam Nutri Survey Dengan TkpiDocument7 pagesMembandingkan Recall 24 Jam Nutri Survey Dengan TkpiFransisca SihotangNo ratings yet
- Chronological OrderDocument5 pagesChronological OrderDharWin d'Wing-Wing d'AriestBoyzNo ratings yet
- Project Wise CSR Expenditure FY202223Document15 pagesProject Wise CSR Expenditure FY202223gowowor677No ratings yet
- Pebc CompilationDocument14 pagesPebc CompilationAarti AroraNo ratings yet
- InteliLite AMF20-25Document2 pagesInteliLite AMF20-25albertooliveira100% (2)
- Project Report On AdidasDocument33 pagesProject Report On Adidassanyam73% (37)
- Virtio-Fs - A Shared File System For Virtual MachinesDocument21 pagesVirtio-Fs - A Shared File System For Virtual MachinesLeseldelaterreNo ratings yet
- Soal Kelas 4 IIDocument5 pagesSoal Kelas 4 IIes tougeNo ratings yet
- Ek Pardesi Mera Dil Le Gaya Lyrics English Translation - Lyrics GemDocument1 pageEk Pardesi Mera Dil Le Gaya Lyrics English Translation - Lyrics Gemmahsa.molaiepanahNo ratings yet
- BarclaysDocument5 pagesBarclaysMehul KelkarNo ratings yet
- XXCCCDocument17 pagesXXCCCwendra adi pradanaNo ratings yet
- Useful Relations in Quantum Field TheoryDocument30 pagesUseful Relations in Quantum Field TheoryDanielGutierrez100% (1)
- Ktu Students: Principles of ManagementDocument22 pagesKtu Students: Principles of ManagementNidaNo ratings yet
- Ketchikan Shipyard Improvements Plan CompleteDocument230 pagesKetchikan Shipyard Improvements Plan CompleteOpó Ishak Bawias Adare100% (1)
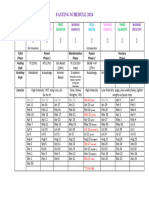
- Moon Fast Schedule 2024Document1 pageMoon Fast Schedule 2024mimiemendoza18No ratings yet
- A Summer Internship Project ON " To Study The Supply Chain Management On Amul Fresh Products" AT GCMMF, AmulDocument19 pagesA Summer Internship Project ON " To Study The Supply Chain Management On Amul Fresh Products" AT GCMMF, AmulweetrydhNo ratings yet
- Technical Description: BoilerDocument151 pagesTechnical Description: BoilerÍcaro VianaNo ratings yet
- Visualization BenchmarkingDocument15 pagesVisualization BenchmarkingRanjith S100% (1)
- An Overview of The FUPLA 2 Tools: Project DatabaseDocument2 pagesAn Overview of The FUPLA 2 Tools: Project DatabaseJulio Cesar Rojas SaavedraNo ratings yet
- Grace Lipsini1 2 3Document4 pagesGrace Lipsini1 2 3api-548923370No ratings yet
- The Unbounded MindDocument190 pagesThe Unbounded MindXtof ErNo ratings yet
- Inventory Storage and Retrieval System PatentDocument15 pagesInventory Storage and Retrieval System PatentdevanasokaNo ratings yet
- Vincent Ira B. Perez: Barangay Gulod, Calatagan, BatangasDocument3 pagesVincent Ira B. Perez: Barangay Gulod, Calatagan, BatangasJohn Ramsel Boter IINo ratings yet
- Answer Questions Only: Chemical Engineering DeptDocument2 pagesAnswer Questions Only: Chemical Engineering DepthusseinNo ratings yet
- Hanwha Engineering & Construction - Brochure - enDocument48 pagesHanwha Engineering & Construction - Brochure - enAnthony GeorgeNo ratings yet
- Multivariate Analysis Homework QuestionsDocument2 pagesMultivariate Analysis Homework Questions歐怡君No ratings yet
- 3 - Content - Introduction To Java, JVM, JDK PDFDocument8 pages3 - Content - Introduction To Java, JVM, JDK PDFAnonymous zdY202lgZYNo ratings yet
- Millennium Separation ReportDocument3 pagesMillennium Separation ReportAlexandra AkeNo ratings yet
- Class 7thDocument24 pagesClass 7thPriyaNo ratings yet
- Essene Moses Ten CommandmentsDocument4 pagesEssene Moses Ten Commandmentsjeryon91No ratings yet