Professional Documents
Culture Documents
ARTG - 2011 - PT Practice in Acute Care Setting
Uploaded by
SM199021Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
ARTG - 2011 - PT Practice in Acute Care Setting
Uploaded by
SM199021Copyright:
Available Formats
Research Report
Physical Therapist Practice in the
Acute Care Setting:
A Qualitative Study
Downloaded from https://academic.oup.com/ptj/article/91/6/906/2735037 by guest on 12 March 2023
Pauline M. Masley, Carey-Leah Havrilko, Mark R. Mahnensmith, Molly Aubert,
Diane U. Jette
P.M. Masley, PT, DPT, was a stu-
dent in the Department of Reha-
bilitation and Movement Science,
Background. Physical therapist practice in the acute care setting is not thor-
University of Vermont, Burlington, oughly understood, and it has been argued that skilled care is not required.
Vermont, at the time of the study.
C.-L. Havrilko, PT, DPT, was a stu-
Objectives. The objective of this study was to describe the role of physical
dent in the Department of Reha- therapists, the clinical reasoning processes used by physical therapists, and the
bilitation and Movement Science, context for providing physical therapy services in the acute care setting.
University of Vermont, at the time
of the study. Design. A convenience sample of 18 physical therapists working in 3 academic
M.R. Mahnensmith, PT, DPT, was medical centers in the United States was included in this qualitative study with
a student in the Department of grounded-theory methods.
Rehabilitation and Movement Sci-
ence, University of Vermont, at Methods. Semistructured interviews were conducted. Transcripts were coded,
the time of the study.
and a constant comparative process of analysis was used to determine common
M. Aubert, PT, DPT, was a student themes. A theoretical model was derived.
in the Department of Rehabilita-
tion and Movement Science, Uni-
versity of Vermont, at the time of
Results. Eight themes were identified: collection and analysis of medical informa-
the study. tion, application of specialized physical therapy knowledge, communication to gain
information, communication to provide information, continual dynamic assessment,
D.U. Jette, PT, DSc, is Professor
professional responsibility, complex environment, and decision making for patient
and Chair, Department of Rehabil-
itation and Movement Science, care. Among the limitations of this study were that the sample and method limited the
University of Vermont, Rowell generalizability of the findings, the participants were not observed in their practices,
Building, 106 Carrigan Rd, Burl- and researchers’ preconceived views may have influenced the interpretation and
ington, VT 05401 (USA). Address derivation of themes.
all correspondence to Dr Jette at:
diane.jette@uvm.edu.
Conclusions. Physical therapists in the acute care setting used clinical reasoning
[Masley PM, Havrilko C-L, Mah- that required the ability to integrate medical information with physical therapy
nensmith MR, et al. Physical ther-
knowledge. Clinical reasoning required continual dynamic assessment of patients in
apist practice in the acute care set-
ting: a qualitative study. Phys Ther. a crowded, complex, fast-paced environment and resulted in rapid decision making.
2011;91:906 –919.] Constant communication with many people was critical to the process. The major
concerns for physical therapists in the acute care setting, like physical therapists in
© 2011 American Physical Therapy
Association other settings, were patients’ mobility and safety. The goals were an optimal plan of
care and an appropriate discharge setting for each patient. The therapists’ roles
reflected professional core values applied in ways unique to the acute care setting.
Post a Rapid Response to
this article at:
ptjournal.apta.org
906 f Physical Therapy Volume 91 Number 6 June 2011
Physical Therapist Practice in the Acute Care Setting
T
he American Physical Therapy Indeed, in the context of so many apists than for patients discharged to
Association’s annual Rothstein interventions from various health settings not in concert with physical
Debate in 20071 revealed vari- care providers in the acute care set- therapists’ recommendations, sug-
ous thoughts and opinions regarding ting, one might ask how much gesting the importance of physical
the role of physical therapists in patient improvement can be attrib- therapists’ input in outcomes for
acute care settings. Although many uted to physical therapy alone. patients.5 However, these studies did
participants engaged in the debate There appears to be little informa- not explore the clinical reasoning
believed that it was clear why phys- tion describing the distinctive processes that physical therapists
ical therapists should provide care in knowledge and skills that physical used in managing their patients’
hospitals, many noted that the role therapists use in the care of patients overall care during acute care stays.
of physical therapists in acute care in the acute care setting. Further- Additionally, the role of physical
settings was not clearly understood more, as evidenced by comments at therapists and the context of their
Downloaded from https://academic.oup.com/ptj/article/91/6/906/2735037 by guest on 12 March 2023
by others and that physical therapy the 2007 Rothstein Debate, physical practice were not investigated. A
might be overutilized or underuti- therapists are aware of the percep- recent study described the broad
lized. Some participants suggested tion that patient care in the acute characteristics of physical therapists’
that ambiguity about the role of care setting does not require skilled, clinical decision making in the acute
physical therapists in acute care set- professional physical therapy care setting,6 but that study was lim-
tings might be partially attributed to personnel.1 ited to physical therapists providing
shortfalls in education, whereas oth- cardiorespiratory care in Australia.
ers discussed the possibility that Skilled services imply a need for The purpose of the qualitative study
physical therapists were simply not complex and sophisticated reason- reported here was to expand the
being asked to practice at a high skill ing and decision making that can be breadth of understanding of the role
level in those settings. What accomplished only by people who of physical therapists, the clinical
emerged from this debate was a are educated as physical therapists. reasoning processes used by physi-
sense of the need to better define Several recent studies described var- cal therapists, and the context for
and describe the role of physical ious aspects of physical therapy providing physical therapy services
therapists in acute care settings, to practice in the acute care setting that in the acute care setting.
educate patients and other health suggested this high level of problem
care professionals about the scope of solving. In 2003, Jette et al3 Method
practice, and to advance the under- described the decision-making pro- Design
standing of patient outcomes attrib- cesses of both physical therapists Qualitative research methods with a
utable to physical therapy manage- and occupational therapists as grounded-theory approach were
ment in acute care settings. Physical related specifically to patient dis- used. This design engaged partici-
therapists at the 2007 Rothstein charge recommendations in the pants (physical therapists) in
Debate provided only anecdotal evi- acute care setting. In that study, the describing, interpreting, and analyz-
dence in support of their work, not- process of decision making appeared ing various aspects of their clinical
ing that they observed patients get- to require high-level thinking to practice. Grounded theory is based
ting better and leaving the hospital draw conclusions by analyzing and on a method of systematic collection
every day. synthesizing findings related to and analysis of qualitative informa-
patients’ activity and participation
The acute care setting is character- restrictions, needs and wants, life
ized by short patient stays brought context, and ability to participate in Available With
about by 2 decades of changing eco- therapy. A more recent study This Article at
nomics in the US health care system. describing the content of physical ptjournal.apta.org
These changes have demanded therapy services in 3 academic med-
increased efficiency and effective- ical centers in the United States in • Discussion Podcast with Gail
ness of patient care and have 2008 indicated that practice cen- Jensen, Sharon Gorman, and
resulted in both fewer physical ther- tered on identifying and managing author Diane Jette. Moderated by
apy sessions for patients and changes limitations in function, on educating Rebecca Craik.
in the types of goals set for an epi- patients, and on discharge planning.4 • Audio Abstracts Podcast
sode of care.2 Such changes in prac- A study published in 2010 reported a This article was published ahead of
tice have given rise to the question lower incidence of hospital readmis- print on April 21, 2011, at
of whether physical therapy is valu- sion for patients discharged to set- ptjournal.apta.org.
able in such a limited time frame. tings recommended by physical ther-
June 2011 Volume 91 Number 6 Physical Therapy f 907
Physical Therapist Practice in the Acute Care Setting
Table 1. convenience sample based on the
Facility Characteristics principal investigator’s acquaintance
Data for Facility:
with managers at the 3 academic
medical centers and their willingness
Characteristic 1 2 3
to facilitate the study. Data were
Size (no. of licensed beds) 430 675 777
available from 18 of the 20 physical
Average patient length of stay (d) 5.2 4.1 4.5 therapists who initially agreed to
Average daily full-time equivalents (physical therapists participate; 1 therapist was unavail-
and physical therapist assistants) on: able during the data collection
Weekdays 14 19 13 period, and 1 therapist could not
Weekends 4 10 5 be reached. The participants are
described in Table 2.
Downloaded from https://academic.oup.com/ptj/article/91/6/906/2735037 by guest on 12 March 2023
tion with the purpose of generating a Participants Procedure
theory that explains a social or psy- A purposive sample of 20 physical Semistructured interviews were con-
chological phenomenon.7 Using the therapists practicing in the acute ducted via telephone or in person,
participants’ perspective, investiga- care setting at 3 academic medical depending on the availability of par-
tors attempt to explain how people centers in the northeastern United ticipants and researchers. One
in a specific setting understand, take States agreed to participate in this interview was conducted with
action, manage, and interact in day- study. The facilities are described in each participant. Each interview
to-day situations. A guiding assump- Table 1. Participants signed informed was recorded with a digital voice
tion of grounded theory is that there consent forms approved by the Com- recorder and transcribed verbatim
is a “basic social psychological pro- mittee on Human Subjects at the Uni- by the investigators. Before the
cess” that members of a group use in versity of Vermont and their own insti- data collection period, we com-
resolving a specific problem.8 tutions, if required. This was a
Table 2.
Participant Characteristics
Years
Practicing
in Acute Highest
Participant Years Care Professional Certified
No. Institution Sex Practicing Settings Degree Specialization
1 1 Female 2.5 2.5 DPT None
2 1 Female 9 9 DPT Neurology
3 1 Female 5 5 MSPT None
4 1 Female 9 9 DPT Geriatrics
5 1 Female 32 12 DPT Neurology
6 1 Female 6 3 MSPT None
7 1 Female 6.5 6.5 MSPT None
8 1 Female 3 3 MSPT None
9 2 Female 4 4 DPT None
10 2 Female 3 3 DPT None
11 2 Female 4.5 4.5 MSPT None
12 2 Male 2.5 2.5 DPT None
13 2 Male 7 7 DPT Cardiopulmonary
14 3 Female 24 21 BS None
15 3 Female 13 10 DPT None
16 3 Female 22 10 BS None
17 3 Male 29 29 DPT Cardiopulmonary
18 3 Female 13 12 MSPT None
908 f Physical Therapy Volume 91 Number 6 June 2011
Physical Therapist Practice in the Acute Care Setting
piled a list of potential questions to his or her management of patients’ became evident that no new infor-
ask the participants (Appendix). mobility was different from that of mation was emerging from inter-
The questions were derived from nurses, a follow-up question might views with the 18 participants.
information in the literature that be, “Tell me a bit more about those
suggested the types of decisions differences.” The order of questions When the interviews were com-
made by physical therapists and and the specific wording varied on pleted, we searched the transcripts
their roles in the acute care set- the basis of the dialogue during the for the prime indicators of various
ting.3– 6 However, consistent with interview and follow-up questions. concepts, confirming or disconfirm-
grounded theory and to limit our The interviews lasted, on average, 1 ing our original labels and determin-
biases, we completed a relatively hour. ing whether all concepts had been
superficial literature review.9(p32) discovered. Meetings progressed
During the analysis of data, we con- Analysis through an iterative process in
Downloaded from https://academic.oup.com/ptj/article/91/6/906/2735037 by guest on 12 March 2023
ducted a more thorough literature As the interviews proceeded, a con- which themes were proposed;
review in an attempt to find and stant comparative process was used: debated to determine overlaps, gaps,
explain links between the existing we read transcripts, labeled text, and clarity, and relationships with one
literature and the themes emerging met weekly to analyze and discuss another; and then revised. Once the
from our work.9(p32) The questions interview content and strategies, general themes were agreed upon,
also were derived from anecdotal adjust questions, and determine their specific titles and definitions
information from physical thera- emerging concepts and themes.8,11 were determined through an itera-
pists who worked in the acute care Through this process, we refined the tive process of proposal, debate,
setting and who described their interview questions to better address refinement and, finally, group con-
approaches to patient care and the the overall purpose of the investiga- sensus. We then reassessed the tran-
changes that they had seen in their tion. For example, when a new con- scripts to confirm or refute the
practice settings in recent years. cept was mentioned by a participant, themes that were agreed upon. We
we discussed whether the concept also sought to compare themes
The process of questioning was required more explicit exploration within each setting and across set-
designed to facilitate deep discus- with subsequent participants. In tings.11 Next, we selected specific
sion and provide rich descriptions of addition, we read each transcript quotations that supported and best
the clinical reasoning processes and critiqued the interview to iden- exemplified the themes. Using the
underlying physical therapists’ deci- tify ways in which subsequent inter- themes and their hypothesized rela-
sions and actions, the context or views could be improved to provide tionships, we developed a working
environment in which they prac- additional detail and depth of infor- theoretical model to describe the
ticed, and their perceptions of the mation. The constant comparative decision-making process, the role of
roles that they played in their prac- process ensured the saturation of physical therapists, and the context
tice settings. That is, questions were data. This process involved reading for providing physical therapy ser-
designed to elicit more than simple each transcript as it was produced vices in the acute care setting.
“yes” or “no” responses, and and discussing the connections
follow-up questions were asked to among statements made by the par- After we defined the themes and
solicit details to enhance the initial ticipant during the interview and the developed a working theoretical
answer to a question.10(p94) Partici- similarities and differences between model, we summarized the themes
pants controlled the flow of informa- the information provided during the and their meanings with support-
tion so as to limit the extent to interview and the information ing quotes and provided this
which the interviewer led the discus- obtained from previous transcripts. material to participants for their
sion. For example, we asked partici- At each reading, we identified review.12(pp275–276) Participants
pants what criteria they used to words, phrases, and concepts that were invited to confirm, refute, elab-
decide whether a patient received were reiterated as well as newly orate on, or suggest edits for the
physical therapy service. If a partici- expressed ideas. This process led us themes and the meanings that we
pant said that he or she first deter- to decide what, if any, additional had assigned. This process of mem-
mined whether a patient was medi- information we wanted to obtain ber checking was conducted to
cally stable, then the interviewer from subsequent interviews and ensure that none of the participants’
asked the participant to talk more how to phrase questions to solicit responses was misinterpreted or
about what medical stability meant the desired information.11 We deter- omitted and, most importantly, that
and how to determine medical sta- mined that no new participant our interpretations were viewed as
bility. If a participant mentioned that recruitment was required when it being accurate. Sixteen participants
June 2011 Volume 91 Number 6 Physical Therapy f 909
Physical Therapist Practice in the Acute Care Setting
responded, and their feedback patient’s presentation and what their Participants believed that their
largely confirmed the themes that approach to patient care might be knowledge and skills in this area
we had identified. Three provided before they met the patient: “You were unique and essential to the role
suggestions for further refinement of start making decisions from the min- that they played in the acute care
the theme definitions, and these ute you start looking at the chart” setting, noting physical therapists
were incorporated. Finally, an (PT-14). Participants expressed the may be the only providers asking
expert qualitative researcher who need to apprise themselves of diag- questions such as, “. . . can they
was not one of the investigators was nostic test results, imaging reports, move in bed, and do they do safe
asked to review the participant surgical procedures, and other data transitional movements? Do they
transcripts, themes, and the that might indicate activity precau- need an assistive device?” (PT-17).
model.12(pp281–282) She provided feed- tions, such as weight-bearing status, Participants noted that their special-
back about the relationships of the blood pressure, heart rate, and oxy- ized knowledge about movement
Downloaded from https://academic.oup.com/ptj/article/91/6/906/2735037 by guest on 12 March 2023
themes and suggested 1 additional gen saturation. They also identified and function was what separated
theme that was incorporated into the need to understand the implica- them from nurses or technicians
the model. tions of these data for their selection who might walk up and down a hall-
of interventions as well as the way with a patient for the sake of
Results patient’s ability to participate. One getting the patient out of bed. One
Eight themes that described the clin- participant stated, “I look through participant described this difference
ical reasoning processes used by those lab values looking for any as follows: “A nurse might just look
physical therapists, their role, and trends and sort of start building a at a patient and see them walking,
the context for providing physical picture of what this person looks but a PT [physical therapist] might
therapy services in the acute care like” (PT-13). Another said, “If we look at a patient and see subtle dif-
setting were identified. get somebody for chest PT, I usually ferences in their gait and step length
look at whether they have lab tests and stride and be able to assess that
Core Constructs that would indicate that they have an in connection with their safety and
Four themes— collection and analy- infection” (PT-5). baseline” (PT-2). Another participant
sis of medical information, applica- described physical therapists’ dis-
tion of specialized physical therapy Application of specialized physi- tinct role in facilitating patients’
knowledge, communication to gain cal therapy knowledge. Partici- independent mobility: “I think that
information, and communication to pants reported the importance of the nurses. . .tend to do more for the
provide information—suggested the their expertise in mobility and move- patient than the patient may actually
fundamental core from which clini- ment dysfunction in the care of need, whereas we go in with the
cal reasoning proceeded during each patients: “We’re the experts in mind-set of letting the patient do as
encounter with a patient as well as mobility and safety from a mobility much as they can on their own” (PT-
over the entire episode of care. standpoint. So, we’re consulted in 4). Participants believed that their
order to give our opinion on a specialized knowledge and focus on
Collection and analysis of medical patient’s ability to move and func- safe, effective, and independent
information. Participants stated tion” (PT-4). This specialized knowl- functional mobility were what made
the need to collect and reflect on edge is used to create a plan of care physical therapists’ role in the acute
medical information as an important and to inform prognosis. Participants care setting unique. Put succinctly
first step in analyzing the appropri- also described physical therapy– by one participant, “I don’t think
ateness of therapy for a patient. specific knowledge about a patient’s anyone has the training we have as
Their approach to securing this movement gained and applied dur- far as movement dysfunction”
information was characterized by ing a treatment session. Participants (PT-2).
statements such as the following: “I noted that physical therapists are
look at the chart to determine if I concerned with the quality, effi- Communication to gain informa-
think that they are medically stable ciency, and functionality of move- tion. Participants noted that they
for PT [physical therapy]” [stated by ment, not just the ability to move. perpetually acquired information
participant 7 (PT-7)] and “If a per- For example, when informed by a about their patients from a number
son’s hematocrit is very low, then nurse that a patient had gotten out of of sources. Physical therapists rou-
we may want to wait until they get a bed and “walked around,” a partici- tinely spoke with patients, families,
blood transfusion” (PT-9). Partici- pant noted, “I want to see what that and team members such as nurses,
pants also used medical information ‘walking around’ means. I want to physicians, and case managers to col-
to formulate an overall image of a see the quality of it” (PT-5). lect information regarding patients’
910 f Physical Therapy Volume 91 Number 6 June 2011
Physical Therapist Practice in the Acute Care Setting
status and progress: “I may go up and rate, oxygen level—let them know if [computed tomography] scan, and
verify with the nurse what the I weaned the patent off of oxygen, she had multiple sclerosis” (PT-17).
patient is actually doing. I may call anything like that” (PT-7). Partici-
the resident and . . . I’ll talk to the pants believed that it was necessary Encompassing Constructs
patient” (PT-14). Speaking with to provide nursing staff with infor- Three themes— continual dynamic
nurses and physicians to gain infor- mation to help them understand a assessment, professional responsibil-
mation about a patient’s status and patient’s functional abilities and ity, and complex environment—
progress since the previous session allow nurses to continue the mobil- encompassed and incorporated the
was thought to be essential to effi- ity plan that the physical therapist fundamental core, suggesting the
cient and effective care. had recommended: “[I] let them influence of perceived role and envi-
know how a patient did with us so ronment on clinical reasoning
Gaining information from patients that they can carry it over or [tell processes.
Downloaded from https://academic.oup.com/ptj/article/91/6/906/2735037 by guest on 12 March 2023
and family members regarding the them] how they can help the patient
living situation and the amount of back to bed” (PT-16). Continual dynamic assessment.
assistance a patient would have at We conceptualized continual
home influenced the interventions Participants reported the need to dynamic assessment as on-the-spot,
selected during the course of the speak with physicians and other reiterative clinical reasoning. Contin-
patient’s stay in the acute care set- members of the health care team. As ual dynamic assessment involved a
ting, as well as discharge planning: one participant noted, “It takes com- within-session, moment-to-moment
“We want to know about their pre- munication because maybe the process of recurring evaluation,
vious level of function. We want to medical doctors think someone will adaptation of interventions, and
know their home environment and be able to go home but then they adjustment of goals as a session pro-
how their home setup is. We want to don’t progress as well. . . .” (PT-12). ceeded and a patient responded to
know their equipment needs” (PT- Another participant said, “I’ll also an intervention. It required analysis
12). Similarly, another participant check in with the case manager, so of medical data, use of specialized
stated, “I need to know from the that they can start planning” (PT-7). knowledge, and integration of infor-
family, ‘How much support are you In general, the participants believed mation gleaned from reading a med-
capable of providing?’” (PT-11). that their communication was val- ical record and from communication
ued and respected and that they with the patient and other health
Communication to provide infor- were consulted and asked for their care team members. Participants
mation. In addition to acquiring opinions about patients’ status and noted the need to continually moni-
information about their patients, par- needs. As noted by one participant, tor their patients and assess their
ticipants consistently spoke with “[Some physicians] will call you spe- physiological responses throughout
patients, families, and team members cifically, ‘You were a great help with each treatment session regardless of
to report patients’ status and prog- this last patient. What do you think the severity of their conditions. As
ress. Participants agreed that it was about. . .?’” (PT-18). Participants also one participant explained, “I look at
important to keep the patient and indicated that communication with heart rate response to exercise, . . .
the patient’s family informed of physicians was required if anything blood pressure response, . . . oxygen
progress being made in therapy, was unclear or if “red flags” saturation, . . . balance, and RPE
short-term and long-term goals, and appeared during therapy. One par- [rate of perceived exertion]”
the physical therapist’s recommen- ticipant described a situation in (PT-11). Participants explained that
dations for placement after acute which he was asked to provide a they needed to be ready to make
care: “I’ll say to them, ‘Based on how quick safety screen before a 40-year- quick decisions about alterations in
you performed today, I think you’ll old patient who had fallen was sent their care at any given time, depend-
be able to go home from here’ or ‘I home from the emergency depart- ing on how a patient was reacting:
think you’ll need to go to rehab’” ment: “Her reflexes were inconsis- “When you’re [with the patient]
(PT-7). Participants expressed the tent from right lower extremity to you’re always thinking about should
need to provide nursing staff with left lower extremity. Her coordina- I proceed to the next step, physio-
information about a patient’s prog- tion was off; her proprioception was logically? Where to stop, when to
ress, especially if anything significant off . . . taking one step forward, she stop, or how can I proceed safely?”
changed: “I would also check in with completely lost her balance. I gave (PT-5). Participants also described a
the nurses to let them know how the the doctor all this data. I said she similar session-to-session process of
patient performed and alert them to needs a neuro consult. She had a CT recurring evaluation to determine
any changes in blood pressure, heart goals as well as types and intensities
June 2011 Volume 91 Number 6 Physical Therapy f 911
Physical Therapist Practice in the Acute Care Setting
of interventions, asking the question, supporting my prognostic indicators sessions actually involved: “I think
“Do I need to modify what I’m or my discharge plans as often as I that sometimes other health care
doing?” (PT-14). One participant can.” professionals underestimate what
gave an example of this process we do because I think we make it
when revisiting one of her patients: As part of their professional respon- look easy” (PT-5). “Interns and resi-
“Her sats (oxyhemoglobin satura- sibility, participants noted the need dents think our role is purely just
tion) were only 92%, and so I to contribute to high-quality care. walking, as opposed to doing true
thought that was a little bit For example, participants described assessments of gait, of balance, of
odd. . . . So that made me think, ‘I’m developing standards of care for mental status, of safety” (PT-10). Par-
going to make sure I check her patients: “We have a patient care ticipants believed that these situa-
breath sounds’” (PT-2). standard for pretty much every sin- tions were opportunities to uphold
gle thing that we do . . . updated their professional responsibility by
Downloaded from https://academic.oup.com/ptj/article/91/6/906/2735037 by guest on 12 March 2023
Professional responsibility. Par- with [supporting] literature” (PT-4). educating others about the role of
ticipants described to us a strong Participants also described physical physical therapists and how and
sense of professional responsibility therapists’ roles in providing care when to utilize their services: “What
to their patients, coworkers, and through clinical pathways for some we should be doing if we get an
institutions and to the profession as a types of conditions. In other cases, inappropriate referral is trying to
whole. This sense of responsibility participants noted following track down the resident . . . and
defined their roles and influenced physician-driven protocols for cer- helping to educate them” (PT-15).
the way in which they collected and tain types of conditions. It was not
used information, their communica- clear whether physical therapists Participants discussed another com-
tions with others, their clinical rea- had input into these protocols. ponent of professional responsibility
soning, and the decisions they made. as advocating for patients’ best inter-
We conceptualized professional Participants also demonstrated an ests, even if their professional
responsibility as exercising profes- awareness of their accountability for recommendations differed from
sional expertise to advocate for good outcomes for patients: “Basi- those of physicians: “If you feel
patients and contribute to the quality cally you don’t [want to] end up strongly about it and you feel it’s
of patient care. Participants upheld with somebody who’s disabled important for your patient, you’ll
this responsibility through various because we didn’t move them when advocate for it regardless of the
means, including maintaining stan- we could have” (PT-5). High-quality response that you’re worried about
dards of practice, educating others care also meant ensuring that skilled getting” (PT-18).
about their practice, providing edu- and appropriate physical therapy
cation to other health care profes- care was delivered. This responsibil- Physical therapists’ responsibilities
sionals to enhance their safety, and ity included making decisions about were also noted to include contrib-
advocating for the best patient care which patients should receive phys- uting to the safety of health care
and outcomes. ical therapy services and how best to team members through education
provide that care. We heard partici- about mobilizing patients. As noted
Participants viewed maintaining pants express concern about some- by one participant, “After we evalu-
competence as a way in which to times improper utilization of physi- ate their mobility, we’re going to
promote professional responsibility: cal therapy in the hospital: “I feel like make recommendations for the
“Our job requires us to maintain pro- we can be inappropriately used as a nurses on how we think it’s safe for
fessional competence and our pro- walking service” (PT-2). Another par- them to be mobilizing the patient”
fessionalism, and part of that is main- ticipant noted, “Sometimes we get (PT-2). The same participant contin-
taining our knowledge” (PT-13). more consults than are necessary ued, “That’s kind of our job to make
Participants also noted the obligation because people kind of see us as, you sure that the patient is safe and that
to use evidence in practice to uphold know, ‘you call, we haul’” (PT-5). the nurses are safe helping them
standards and provide the best care mobilize.”
for their patients: “I think everything Participants indicated that the scope
should be evidence based. That’s the of practice for physical therapists Complex environment. Partici-
only proof that we have that certain was not understood by health care pants described the acute care set-
things are effective” (PT-3). The team members, possibly because of ting as a complex environment char-
same participant went on to say, “I the discrepancy between what it acterized by a fast pace, multiple
try to cite evidence from the litera- looked like they were doing with interactions, ubiquitous high-tech
ture in my assessment statements patients and what their treatment equipment, and the precarious
912 f Physical Therapy Volume 91 Number 6 June 2011
Physical Therapist Practice in the Acute Care Setting
nature of patients’ health and physi- stuff” (PT-5). At the same time, par- patients want . . . and trying to com-
ological states. The environment ticipants remarked that, unlike phys- bine all that into what the therapist
influenced all aspects of physical ical therapy in other settings, physi- needs to be able to do” (PT-8).
therapy care in the acute care setting cal therapy in the acute care setting
as well as the roles and responsibili- must have a multisystem focus. That Decision making appeared to take 2
ties of the physical therapists work- is, participants’ concerns were never forms. One form we labeled as
ing in it. The environment required limited to 1 body part or system micro-level decision making. We
the understanding of medical infor- but revolved around patients’ overall defined this type of decision making
mation and the application of spe- function and physiological state: as a minute-to-minute and day-to-
cialized knowledge and dictated the “We’re trying to prevent . . . range of day process. Micro-level decisions
need for continual and rapid assess- motion issues . . . skin breakdowns included within-session decisions
ments: “In this environment some of . . . pneumonias . . . severe decondi- regarding the content of examina-
Downloaded from https://academic.oup.com/ptj/article/91/6/906/2735037 by guest on 12 March 2023
the decisions are life and death. You tioning” (PT-5). tions, intensity of exercise, or dura-
could make a clinical decision that tion of session and between-session
literally could kill somebody. So, you Participants noted that providing decisions about frequency of treat-
have to understand the equipment, patient care in this complex environ- ment. As an example, one partici-
the bolts, the drains, the lines, the ment required they have not only pant said she might, “[ask a patient
science behind things” (PT-16). effective communication skills but about] lightheadedness, any increase
Some examples of situations in also an ability to adapt those skills in pain, any shortness of breath,
which participants needed to make to interact with a large number and [then] retak[e] vital signs, assessing
critical decisions included recogniz- a wide variety of people through- his sitting balance while he’s there. If
ing worsening of mental status as out the day: “So, [I do] a lot of he’s ok, then we move on; if he’s
potential recurrence of hemorrhag- communication with other health not, then we can always lie back
ing in the brain, recognizing abnor- care providers . . . we work with the down” (PT-8). Another participant
mal neurological findings that physi- team . . . MDs and the nurses . . . discussed this type of decision mak-
cians had not noted, understanding and care coordinators” (PT-12). Addi- ing as it related to considering the
the need to defer treatment when tionally, communication was viewed impact of patients’ medications after
blood pressure was unstable, and as being critical to the safety of cardiac surgery on her management
knowing precautions for avoiding patients in an environment in which decisions: “If they’re requiring blood
negative effects on surgical patients’ physiological status could pressure support with pressor med-
procedures. rapidly change. Participants per- ications, then I’m probably not going
ceived the level and diversity of com- to see them, . . . . I would be cau-
Participants noted that decisions munication as being much different tious of a patient [who] was requir-
about patient care were made much from what occurs in other practice ing medication to control chest pain.
more quickly and that the total time settings. [These situations] would indicate
frame in which they cared for an that they’re not hemodynamically
individual patient was much shorter Result of Clinical Reasoning: stable and they might require further
than in other practice settings: “I Decision Making for Patient Care medical or surgical intervention”
need to be able to make decisions Decision making for patient care (PT-11).
much quicker and be able to antici- involved formulating and executing
pate the patient’s progress much an optimal plan of care on a moment- We labeled a second form of deci-
quicker” (PT-7). With regard to to-moment, within-session basis as sion making as macro level. We
deciding the most effective interven- well as over the entire episode of viewed this form of decision making
tions for a patient, one participant care. Our participants described ful- as a process related to longer-term
stated, “You have such a short time filling their professional role and goal setting and discharge planning.
with patients that it’s really, ‘OK, responsibilities and using continual At the macro level, the major focus
what are the big bangs for today?’” dynamic assessment while integrat- of participants’ decision making was
(PT-18). We also heard participants ing the information collected from determining goals that supported
say that they were working within a the medical record, from the patient discharge plans and moved patients
crowded and physically complex examination, and from communica- toward leaving the hospital. Macro-
space to deliver care for patients: tion with various parties to develop level decision making was based on
“It’s moving them safely with all the the best plan of care: “There’s a lot of the “big picture” and went beyond
lines and the tubes and the monitors thinking [about] what the doctors patients’ stays in the acute care set-
and making sure we don’t dislodge want, the nurses want, and the ting: “I see us as sort of being the
June 2011 Volume 91 Number 6 Physical Therapy f 913
Physical Therapist Practice in the Acute Care Setting
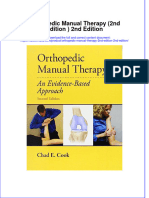
care setting. The theoretical model
shown in the Figure represents the
themes and their relationships and
interactions. The complex practice
environment interacted with partici-
pants’ sense of professional respon-
sibility and shaped their clinical rea-
soning processes and their decisions
regarding patient care. As evidenced
by the descriptions of our partici-
pants and as noted by Edwards and
Jones,13 the process of clinical rea-
Downloaded from https://academic.oup.com/ptj/article/91/6/906/2735037 by guest on 12 March 2023
soning was influenced by the larger
social context, that is, shaped by the
environment and the perspectives
and values of the physical therapists
working in the environment.
Although an episode of care in the
acute setting has a well-defined
beginning and end, our model sug-
gests that participants did not view
their care of a patient as a linear,
stepwise process leading from
admission to discharge. The process
required continuous, repetitive clin-
ical reasoning and decision making
and a willingness to change a plan
instantaneously during a single treat-
ment session as well as across the
episode of care. The process contin-
Figure. ued until the ultimate patient out-
Theoretical model. come in the acute care setting: dis-
charge to the next, appropriate level
of care. Similarly, Smith et al,6 in
describing decision making by car-
triage system for all of the other ther- leans on us to make a decision diorespiratory physical therapists in
apies that they may need when they whether a patient can go home or go the acute care setting, and Edwards
leave. We’re going to plan out [the to rehab to get their process mov- et al,14 in describing the clinical rea-
patient’s] rehab process from our ing” (PT-4). “We’re widely respected soning of orthopedic and neurologic
first initial meeting with him until as far as our input . . . they want us physical therapists in private prac-
the planned discharge day” (PT-13). to make an assessment to say where tice and physical therapists in home
Participants indicated a broad range does this patient need to go” (PT-17). health care settings, found that the
of factors considered in macro-level processes were multifaceted, com-
decisions: “It depends on the diagno- Discussion plex, and cyclical in nature.
sis, it depends on discharge plan, Theoretical Model
also what their status is at the time of Eight themes described core ele- Core constructs. We found 4
the evaluation and what their status ments necessary for clinical reason- themes at the core of the clinical
was prior to coming in” (PT-16). ing and its reiterative quality, the reasoning process in the acute care
Finally, participants emphasized the environment in which clinical rea- setting: (1) collection and analysis
importance of macro-level decision soning was accomplished, the of medical information, (2) applica-
making, particularly in relation to results of the clinical reasoning pro- tion of specialized physical therapy
recommendations for discharge cess, and physical therapists’ per- knowledge, (3) communication to
planning: “Most of the medical team spective on their role in the acute gain information, and (4) commu-
914 f Physical Therapy Volume 91 Number 6 June 2011
Physical Therapist Practice in the Acute Care Setting
nication to provide information. collect and quickly interpret medical nia, and pressure ulcers related to
These were the crucial elements of information for decision making in bed rest. Our participants reported
each treatment session and the other physical therapist practice set- focusing on total body function or
entire episode of care, and each tings as in acute care settings.14 –16 broad concerns about health, safety,
potentially influenced the others. and mobility; this result confirms the
For example, obtaining information In the clinical reasoning process findings of a previous quantitative
about a patient’s medical status from described by our participants, medi- study indicating that more than 80%
a nurse might lead the physical ther- cal knowledge and specialized phys- of the patients seen by physical ther-
apist to attend to certain data from ical therapy knowledge interacted in apists in acute care settings had goals
monitoring equipment as he or she several ways. For example, partici- and interventions related to func-
analyzed the patient’s safety and abil- pants considered how movement tion, regardless of the type of diag-
ity to move from a supine position might compromise medical stability nosis.4 Similarly, participants in an
Downloaded from https://academic.oup.com/ptj/article/91/6/906/2735037 by guest on 12 March 2023
to a sitting position. Changes in the or how medical conditions or medi- earlier study examining the changing
monitored physiological data during cations might affect patients’ physi- roles of physical therapists after
the intervention might then deter- ological responses to movement or hospital restructuring noted an
mine the parameters of the treat- compound safety issues. The physi- increased focus on the functional
ment session and what was com- cal therapists understood, antici- needs of patients.18
municated back to the nurse or pated, and planned for these various
physician. possibilities. Once the medical status The physical therapists in our study
of a patient was understood and integrated medical information and
Because, by its nature, the acute care anticipatory preparations were specialized knowledge in originating
setting is one in which patients who made, the physical therapists in our bidirectional communications. That
are medically unstable are treated, study used their specialized knowl- is, they formulated questions to gain
the physical therapists in our study edge and skills to evaluate safety and relevant information from patients
needed to use knowledge about independence in functional mobil- and members of the health care team
pathophysiology, symptoms and ity. This approach represented diag- and provided information to them.
findings related to red flags, treat- nostic reasoning in that it included Participants seemed to view their
ment precautions and contraindica- gathering and interpreting of infor- communications in these 2 forms,
tions, pharmaceutical benefits, mation to determine the type or each with distinct content and pur-
adverse effects and interactions, and extent of a problem.13,14 pose. Their communications formed
normal versus abnormal physiologi- elements of both diagnostic and nar-
cal responses to movement both Most of the information used in this rative clinical reasoning.13,14 In the
before and during treatment ses- part of the clinical reasoning process context of the acute care setting, nar-
sions. The physical therapists in our was derived from watching patients rative, or patient-centered, reasoning
study also needed to know the move and assessing the quality of the appears to take the form of under-
appropriate information to collect movement and the physiological standing the impact of patients’
to derive an analytically sound plan response to the movement. Simi- needs and wants, culture, and the
of care. The physical therapists larly, Smith et al6 described how social-economic environment on dis-
monitored, quickly interpreted, and cardiorespiratory physical therapists charge recommendations.3
responded to various types of data to used the response to an interven-
ensure the safety of their patients. tion to improve their understand- The physical therapists in our study
Perhaps not surprisingly, Smith et al6 ing of a patient’s condition. Watch- interacted with physicians, nurses,
described similar attributes related ing patients move has also been case managers, and others on more
to decision making in acute care shown to be an important source of than a daily basis. In other settings,
cardiorespiratory physical therapy, information for physical therapists’ communication with patients both
such as the consideration of large decision making in other care set- to gain information about their his-
amounts of data and the immediacy tings16,17 but may focus on impair- tory, goals, and social support as well
of decisions. Although Edwards et ments in a specific body structure or as to educate them about treatment
al14 found that physical therapists region.15 The physical therapists in interventions and options may be
in private practice and home health our study were interested in getting similar or identical, but it is unlikely
care settings considered tissue patients moving for many reasons, that physical therapists communi-
pathology in their diagnostic reason- including those that likely are less cate with the number and variety of
ing, there did not appear to be as common in other settings, such as other health care providers regard-
strong an emphasis on the need to preventing deconditioning, pneumo- ing each patient in other settings as
June 2011 Volume 91 Number 6 Physical Therapy f 915
Physical Therapist Practice in the Acute Care Setting
they do in the acute care setting. In a transpired to maintain the patient’s of excellence. Participants noted
study of factors affecting physical safety while working toward improv- their obligation to uphold profes-
therapists’ decision making in the ing function and independence and sional standards by consistently
long-term-care setting, participants securing the most appropriate dis- using current knowledge and theory
reported consistent interactions charge setting. in their care of patients and by cre-
with nurses and other rehabilitation ating written, evidence-based stan-
colleagues, but other health care Professional responsibility. The dards of care for physical therapy
professionals were not mentioned in theme of professional responsibility staff to reference. Excellence also
this context.16 Our participants suggested the framework in which was demonstrated by participants
expressed an overall feeling of the physical therapists applied core noting the need for ongoing profes-
acceptance by physicians and elements of clinical reasoning and sional development. Finally, the
respect for their opinions and rec- engaged in continual dynamic assess- theme of professional responsibility
Downloaded from https://academic.oup.com/ptj/article/91/6/906/2735037 by guest on 12 March 2023
ommendations. This result may rep- ment. This theme reflected the pro- reflected the core value of profes-
resent an evolving and improving fession’s core values of accountabil- sional duty. Participants were com-
role for physical therapists in acute ity, excellence, and professional mitted to their ultimate role of advo-
care settings, because at least one duty.21 Accountability was mani- cating for the best interests of
earlier study indicated difficult inter- fested in participants accepting their patients and providing effective
actions with physicians and the need diverse roles in the acute care set- physical therapy services.
for physical therapists to develop ting, including educating other
better communication skills.19 health care team members about Professional responsibility in acute
their role, determining whether care physical therapy was docu-
Continual dynamic assessment. patients require their care, and work- mented by Lopopolo in 1999.18 Par-
Continual dynamic assessment ing with nurses to enhance their ticipants in her study described the
reflected the highly changeable safety. It appears that in the acute role of physical therapists in acute
nature of the physiological status of care setting, the role of physical ther- care settings as including highly inte-
the patient in the acute care setting. apy can be misunderstood. Partici- grated clinical reasoning and high
The type of clinical reasoning occur- pants described having to explain levels of communication and collab-
ring during continual dynamic their scope of practice to other pro- oration with other health care team
assessment was largely diagnostic viders and having to be proactive in members, converging on the needs
reasoning.13 That is, during sessions gaining access to patients whom of patients. Additionally, although
physical therapists observed and ana- they believed would benefit from the majority of the participants in
lyzed patients’ subjective reports of their services. We also found that our study had less than 10 years of
how they were feeling and the func- physical therapists believed that it experience, on the whole their prac-
tion of nearly every body system on a was their responsibility to add to the tice seemed to reflect a feature of
rapid and constant basis, all within quality improvement process of the expert physical therapists reported
the context of the data collected institution to ensure that patients by Jensen et al,17 that is, patient
from patients’ charts and the other were receiving what they needed advocacy accomplished through
providers on the team. Alternatives during their stays. Fulfilling this constant communications with oth-
or adjustments to interventions and responsibility took the form of edu- ers involved in patient care.
their potential consequences were cating new residents and nurses
considered, implemented, or aban- about when and why to consult a Complex environment. The
doned even as a treatment session physical therapist and educating complex environment created the
progressed. Continual dynamic nursing staff on how to carry out a overall context within which physi-
assessment mirrored the process of patient’s mobility plan while main- cal therapists practiced in acute care
reflection in action as described by taining their own safety. settings. This theme represents the
Schön.20 Similarly, Smith et al6 varied, fast-paced nature of the acute
reported that cardiorespiratory phys- Accountability was demonstrated care setting, in which a physically
ical therapists revised decisions through participants ensuring that complicated environment is made
throughout all aspect of the episode skilled care was necessary rather more difficult by the amount of inter-
of care and incorporated information than, as noted by one participant, fering or distracting activity occur-
about changes in patients’ condi- allowing physical therapists to func- ring near the physical therapist-
tions into decisions about interven- tion as a “walking service.” The patient interaction. The acute care
tions. The constant and repeated theme of professional responsibility setting also is an intellectually com-
assessment of the “whole patient” also had elements of the core value plex environment, requiring physi-
916 f Physical Therapy Volume 91 Number 6 June 2011
Physical Therapist Practice in the Acute Care Setting
cal therapists to monitor and analyze approaches (selecting and interpret- tion of medical information and the
several different sources of data at ing examinations and interventions) integration of that information with
once in an often crowded and noisy and communicative approaches specialized physical therapy knowl-
environment while keeping patient (addressing the unique perspective edge; continual dynamic assessment
safety paramount. The complexity is of patients, such as fears and expec- resulting in rapid decision making; a
compounded by the number of daily tations).13 Decisions relied on par- focus on the whole patient and the
interactions with other health care ticipants’ medical and specialized impact of all physiological systems
providers. Although not explicitly knowledge as well as information on the patient’s physical function;
describing the environment, Smith about a patient’s personal goals and constant communication with many
et al6 reported some of the same fea- social-emotional status. Participants different people; the application of
tures in decision making in the acute reported that with a typically short knowledge of characteristics of vari-
care setting as our participants, length of stay for their patients, ous discharge settings; and a
Downloaded from https://academic.oup.com/ptj/article/91/6/906/2735037 by guest on 12 March 2023
including criticalness, the changing macro-level decision making related crowded, complex, fast-paced envi-
and evolving status of the patient, to discharge began at the first ronment. However, the major con-
urgency, the number of variables, moment they followed up on a refer- cerns of physical therapists in the
the relevance of all of the available ral. Their initial impressions were acute care setting, like physical ther-
data, and the perceived risks associ- subject to change, but the anticipa- apists in other settings, are patient
ated with a decision. These features tion of a rapid discharge constantly safety and functional mobility. We
are unlikely to dominate other inpa- influenced the decision-making pro- believe that this information may be
tient or outpatient rehabilitation set- cesses. Previous studies also cited helpful to those who educate profes-
tings and have not been reported in the important role of physical thera- sional (entry-level) physical therapist
studies of physical therapists in out- pists in discharge planning and dis- students in preparing them for prac-
patient and home health care charge recommendations in the tice in the acute care environment.
settings.14,15 acute care setting.4,5,18
Limitations
Decision making for patient care. Implications for Practice in the The results of our study are not
In our model, decision making for Acute Care Setting broadly generalizable. We used a
patient care was the result of reiter- Recent research supports the propo- convenience sample of participants
ative clinical reasoning and took sition that physical therapists’ deci- from 1 geographic area and only 3
place within the context of physical sion making in the acute care setting different medical centers. Although
therapists’ professional responsibili- has long-term positive effects on we found commonalities across the
ties in a complex environment. On patients.5 The results of our study 3 medical centers, the views of our
the micro level, the decision-making support the important role of phys- participants and their practice meth-
process used in the acute care set- ical therapists in the acute care ods may not be representative of
ting could be likened to knowing-in- setting. Their knowledge, clinical those in other medical centers or
action, as described by Schön.20 That reasoning skills, decision-making geographic areas. We also did not
is, participants demonstrated flexi- capabilities, and professional respon- observe participants in their prac-
bility in their decision making; deci- sibilities indicate that physical thera- tices, relying solely on their per-
sions were based on tacit knowledge pists in the acute care setting pro- ceptions of the content and con-
and intuition and resulted in instan- vide skilled care that others do not. text of their practices. In addition,
taneous actions. In turn, patients’ Our study attempts to articulate the researcher bias may have influenced
responses to those actions influ- clinical reasoning processes that the development of our themes and
enced subsequent decisions. Smith appear to be simple and second model. When we asked our partici-
et al6 reported similar features of nature to physical therapists in the pants to review our findings, how-
decision making by physical thera- acute care setting. Foundationally, ever, they largely confirmed them.
pists in the acute care setting. these processes appear to be similar
to those reported in the literature for Future Research
Macro-level decision making com- other physical therapy practice set- Our model needs to be validated
prised consideration of the whole tings.6,13–15,17 Clinical reasoning in with different groups of physical
patient in designing and implement- the acute care setting, however, therapists in the acute care setting
ing an optimal plan of care for the appears to have features that are because models of practice and roles
episode of care and recommending a somewhat different from those of physical therapists may vary in dif-
discharge setting. Patient care at the found in other settings. These fea- ferent parts of the United States and
macro level included instrumental tures include the constant applica- around the world. Additional areas of
June 2011 Volume 91 Number 6 Physical Therapy f 917
Physical Therapist Practice in the Acute Care Setting
research that could be explored for each patient. The findings sup- 9 Glaser BG. Basics of Grounded Theory
Analysis. Mill Valley, CA: Sociology Press;
include a comparison of clinical rea- port an important and specialized 1992.
soning processes and decision mak- role for physical therapists in the 10 Munhall PL. Revisioning Phenomenology:
ing across physical therapy settings. acute care setting. Nursing and Health Sciences Research.
New York, NY: National League for Nurs-
Future research could also include ing Press; 1994.
an investigation of why physical 11 Boeije H. A purposeful approach to the
All authors provided writing and data anal-
therapists choose different settings ysis. Dr Jette provided concept/idea/research
constant comparative method in the anal-
ysis of qualitative interviews. Qual Quant.
in which to practice, illuminating design and institutional liaisons. Dr Masley, 2002;36:391– 409.
key skills and personality traits that Dr Havrilko, Dr Mahnensmith, and Dr Aubert 12 Miles MB, Huberman AM. Qualitative
may be more suited to one type of provided data collection. Data Analysis. Thousand Oaks, CA: Sage
Publications Ltd; 1994.
practice environment than another This article was submitted September 2, 2010,
13 Edwards I, Jones MA. Clinical reasoning
and helping students and novices and was accepted February 18, 2011. and expert practice. In: Jensen GM, Gwyer
Downloaded from https://academic.oup.com/ptj/article/91/6/906/2735037 by guest on 12 March 2023
evaluate their career options. DOI: 10.2522/ptj.20100296
J, Hack LM, Shepard KF, eds. Expertise in
Physical Therapy Practice. 2nd ed. St
Louis, MO: Saunders Elsevier; 2007:209.
Conclusion 14 Edwards I, Jones M, Carr J, et al. Clinical
Here we described the role of phys- References reasoning strategies in physical therapy.
1 American Physical Therapy Association. Phys Ther. 2004;84:312–330.
ical therapists, the clinical reasoning Rothstein Debate weighs PTs in acute care.
15 May S, Greasley A, Reeve S, Withers S.
processes used by physical thera- PT 2007: Highlights. http://www.apta.org/
Expert therapists use specific clinical rea-
PTinMotion/2007/9/PT2007/. Accessed
pists, and the context for providing March 29, 2011. soning processes in the assessment and
management of patients with shoulder
physical therapy services in the 2 Holt P, Winograd CH. Prospective pay- pain: a qualitative study. Aust J Phys-
acute care setting. The results ment and the utilization of physical ther- iother. 2008;54:261–266.
apy service in the hospitalized elderly.
revealed that physical therapists Am J Public Health. 1990;80:1491–1494. 16 Wainwright SF, McGinnis PQ. Factors that
influence the clinical decision-making of
used sophisticated clinical reasoning 3 Jette DU, Grover L, Keck CP. A qualitative rehabilitation professionals in long-term
processes that required the ability to study of clinical decision making in recom- care settings. J Allied Health. 2009;38:
mending discharge placement from the 143–151.
integrate medical information with acute care setting. Phys Ther. 2003;83:
17 Jensen GM, Gwyer J, Shepard KF, Hack
specialized knowledge about mobil- 224 –236.
LM. Expert practice in physical therapy.
ity and to engage in rapid and con- 4 Jette DU, Brown R, Collette N, et al. Phys- Phys Ther. 2000;80:28 – 43.
ical therapists’ management of patients in
tinual assessment of patients and the acute care setting: an observational 18 Lopopolo RB. Hospital restructuring and
the changing nature of the physical thera-
their responses to movement. The study. Phys Ther. 2009;89:1–24.
pist’s role. Phys Ther. 1999;79:171–185.
practice environment was highly 5 Smith BA, Fields CJ, Fernandez N. Physical
19 Curtis KA, Martin T. Perceptions of acute
therapists make accurate and appropriate
complex, involving patients who discharge recommendations for patients care physical therapy practice: issues for
were medically unstable and were who are acutely ill. Phys Ther. 2010;90: physical therapist preparation. Phys Ther.
693–703. 1993;73:581–594.
undergoing technological monitor- 20 Schön D. Educating the Reflective Practi-
6 Smith M, Higgs J, Ellis E. Characteristics
ing as well as diverse and frequent and processes of physiotherapy clinical tioner. San Francisco, CA: Jossey-Bass;
interactions with many health care decision making: a study of acute care car- 1987.
diorespiratory physiotherapy. Physiother 21 American Physical Therapy Association.
providers. The results demonstrated Res Int. 2008;13:209 –222. Professionalism in physical therapy: core
that physical therapists in the acute 7 Chenitz WC, Swanson JM. From Practice values. Available at: http://www.apta.
care setting aspired to provide the to Grounded Theory. Menlo Park, CA: org/uploadedFiles/APTAorg/About_Us/
Addison-Wesley Publishing Co Inc; 1986. Policies/BOD/Judicial/Professionalismin
best care for individual patients PT.pdf. Accessed March 29, 2011.
8 Hutchinson SA, Wilson HS. Grounded the-
while assuming some accountability ory: the method. In: Munhall PL, Oiler
for the overall quality of the environ- Boyd C, eds. Nursing Research: A Quali-
tative Perspective. 2nd ed. New York, NY:
ment in which they worked. A con- National League for Nursing Press; 1993:
tribution was the recommendation 209 –243.
of the appropriate discharge setting
918 f Physical Therapy Volume 91 Number 6 June 2011
Physical Therapist Practice in the Acute Care Setting
Appendix.
Potential Interview Questions
What are the criteria used by physicians or nurses when they decide to refer patients for physical therapy? Are they
implicit or explicit? How do the criteria vary by the type of service or unit the patient is on?
When a patient is referred for physical therapy, what are the criteria you use to decide whether the patient receives
physical therapy services?
How do you decide whether or not a patient receives ongoing intervention?
What are the decisions you have to make before, during, and after patient treatment sessions?
Talk about the kinds of information and thoughts that go through your head as you care for patients.
Downloaded from https://academic.oup.com/ptj/article/91/6/906/2735037 by guest on 12 March 2023
What factors influence your decision to . . .?
How critical do you think your decision is to the [progress, safety, motivation, etc.] of the patient?
How often do you have to make decisions about . . .?
How is the decision to . . . influenced by input from other health care professionals?
How are the types of decisions you make different from those physical therapists make in other areas of practice?
How would patients’ care differ if physical therapists were not there?
What is the perception of physical therapists in acute care settings?
Invited Commentary Cynthia Coffin-Zadai
Masley and colleagues are to be This study has described the acute As a result, questions have been
applauded for pursuing this impor- care practice environment as fast raised regarding the relevance of
tant qualitative line of practice anal- paced, time sensitive, complex, and physical therapist intervention and
ysis that identifies and begins to interactive. That setting-specific management, commonly associated
answer the question of what physi- description helps identify the envi- with the more lengthy rehabilitation
cal therapists specifically contribute ronmental changes that have phase of care, being delivered in
to the management of patients in the occurred as the length of stay has such a fast-paced setting.3 The
acute hospital environment.1 One shortened in response to dwindling responses of the physical therapists
essential value derived from probing reimbursement. According to the interviewed in the study by Masley
the content and outcome of the Centers for Disease Control and Pre- and colleagues suggest something
physical therapist’s contribution is vention’s National Center for Health else is occurring.1 The themes of this
the creation of a detailed description Statistics, the number of hospital article and previous studies regard-
of acute care practice that can lead days of care for patients of all ages ing the role of the physical therapist
to valid quantitative study. Specifi- was 226 million in 1970 compared seem to demonstrate that physical
cally determining which patients with only 166 million in 2006.2 Sim- therapists have evolved to becoming
benefit most from physical therapist ilarly, the average length of stay was valued professional consultants who
management allows us to eliminate 7.8 days in 1970 and 4.8 days in provide a unique, essential perspec-
unnecessary care and deliver tar- 2006. Today’s hospital environment tive, rendering them integral contrib-
geted care more efficiently. An addi- is one where patients are admitted utors to the acute care team.4 – 6
tional and equally important out- for procedures, invasive medical Today’s physical therapists special-
come will be our ability to better management, and surgical interven- ize in evaluating and managing the
define the professional skill set phys- tions while longer-term healing, patient’s functional mobility needs
ical therapists require to provide the recovery, and rehabilitation occur and, within that scope, serve as both
identified services. elsewhere. consultants and effective transitional
care providers.
June 2011 Volume 91 Number 6 Physical Therapy f 919
You might also like
- Improving Functional Outcomes in Physical RehabilitationDocument342 pagesImproving Functional Outcomes in Physical Rehabilitationhis.thunder12287% (23)
- Clinical Desision in Therapeutik ExerciseDocument335 pagesClinical Desision in Therapeutik ExerciseBrina BeBe Ifakristina100% (3)
- Evidence-Based Practice in Pediatric Physical Therapy by BarryDocument14 pagesEvidence-Based Practice in Pediatric Physical Therapy by BarryFe TusNo ratings yet
- Cognitive-Behavioral Therapy: Instructor's ManualDocument68 pagesCognitive-Behavioral Therapy: Instructor's ManualzingpalmsNo ratings yet
- Transference Interpretation in The Psychotherapy of Borderline Patients: A High-Risk, High-Gain PhenomenonDocument12 pagesTransference Interpretation in The Psychotherapy of Borderline Patients: A High-Risk, High-Gain PhenomenonPaz LanchoNo ratings yet
- IFU Stimulate - LFT01 Rev.02Document9 pagesIFU Stimulate - LFT01 Rev.02Ana ČolovićNo ratings yet
- Natural Alternative Medicine 2013Document2 pagesNatural Alternative Medicine 2013kitianahelloNo ratings yet
- Solution-Focused Brief FamilyDocument17 pagesSolution-Focused Brief Familydido dagNo ratings yet
- Upload 5Document9 pagesUpload 5umair muqriNo ratings yet
- Manual Therapy: Neil Langridge, Lisa Roberts, Catherine PopeDocument6 pagesManual Therapy: Neil Langridge, Lisa Roberts, Catherine PopeVizaNo ratings yet
- Upload 1Document10 pagesUpload 1umair muqriNo ratings yet
- Pincus 2006Document9 pagesPincus 2006Claudio Andrés Olmos de AguileraNo ratings yet
- Awareness and Knowledge of Physical Therapy Among Medical Interns A Pilot StudyDocument7 pagesAwareness and Knowledge of Physical Therapy Among Medical Interns A Pilot StudyInternational Journal of PhysiotherapyNo ratings yet
- Updated Integrated FrameworkDocument17 pagesUpdated Integrated FrameworkE. Jimmy Jimenez TordoyaNo ratings yet
- Managing Low Pain: Attitudes and Treatment Preferences Physical TherapistsDocument8 pagesManaging Low Pain: Attitudes and Treatment Preferences Physical TherapistsSachin0808No ratings yet
- Articulo FisioterapiaDocument10 pagesArticulo FisioterapiaMonica LopezNo ratings yet
- Usual Care Physiotherapy During Acute Hospitalization in Subjects Admitted To The ICU: An Observational Cohort StudyDocument10 pagesUsual Care Physiotherapy During Acute Hospitalization in Subjects Admitted To The ICU: An Observational Cohort StudyJhon F. GonzalezNo ratings yet
- Updated Integrated Framework For Making Clinical Decisions Across The Lifespan and Health ConditionsDocument13 pagesUpdated Integrated Framework For Making Clinical Decisions Across The Lifespan and Health ConditionsmaryelurdesNo ratings yet
- Am I Doing The Right Thing Provider Perspectives On Improving Palliative Care in The Emergency Department 2009 Annals of Emergency MedicineDocument9 pagesAm I Doing The Right Thing Provider Perspectives On Improving Palliative Care in The Emergency Department 2009 Annals of Emergency MedicineTUTIK SISWATINo ratings yet
- Physical Therapy Research in Professional Clinical PracticeDocument5 pagesPhysical Therapy Research in Professional Clinical PracticeProductivity 100No ratings yet
- Pta 2750 Term Research ProjectDocument11 pagesPta 2750 Term Research Projectapi-240265376No ratings yet
- Original Research: Patterns of Clinical Reasoning in Physical Therapist StudentsDocument13 pagesOriginal Research: Patterns of Clinical Reasoning in Physical Therapist StudentsNishtha singhalNo ratings yet
- Patient Centerdness in Physiotherapy WhaDocument2 pagesPatient Centerdness in Physiotherapy Whapedroperestrelo96No ratings yet
- Occupational Therapy in Australian Acute Hospitals: A Modified PracticeDocument9 pagesOccupational Therapy in Australian Acute Hospitals: A Modified Practicesarawu9911No ratings yet
- Clinical Reasoning in Manual TherapyDocument11 pagesClinical Reasoning in Manual TherapyKhushboo PakhraniNo ratings yet
- C P G: C C L B P: Riginal RticleDocument22 pagesC P G: C C L B P: Riginal RticleRajender BishtNo ratings yet
- Clinical Reasoning Strategies in PTDocument19 pagesClinical Reasoning Strategies in PTamitesh_mpthNo ratings yet
- Designing A Polarity Therapy ProtocolDocument12 pagesDesigning A Polarity Therapy ProtocolTariq J FaridiNo ratings yet
- 5-2016 42 Ijmah GoniometeryDocument7 pages5-2016 42 Ijmah GoniometeryNatalie AcostaNo ratings yet
- Orthopedic Manual Therapy 2nd Edition 2nd EditionDocument61 pagesOrthopedic Manual Therapy 2nd Edition 2nd Editionkevin.smart540100% (38)
- Carr e ShepaherdpdfDocument4 pagesCarr e ShepaherdpdfPedro FonsecaNo ratings yet
- 2010 - Calidad Movimiento en Fisioterapia PDFDocument15 pages2010 - Calidad Movimiento en Fisioterapia PDFMargarita CorreaNo ratings yet
- Psychoeducational InterventionDocument12 pagesPsychoeducational InterventionAlicia BrevaNo ratings yet
- Knowledge Attitudes and Barriers Towards Evidence Ba - 2017 - Hong Kong PhysioDocument9 pagesKnowledge Attitudes and Barriers Towards Evidence Ba - 2017 - Hong Kong PhysioAnuj ShandilyaNo ratings yet
- Physiotherapy For Functional Motor Disorders: A Consensus RecommendationDocument7 pagesPhysiotherapy For Functional Motor Disorders: A Consensus RecommendationHesti hasanNo ratings yet
- Manual Therapy: Critical Assessment Profession of Physical Therapy Role TheDocument10 pagesManual Therapy: Critical Assessment Profession of Physical Therapy Role TheManuel Silva HérnandezNo ratings yet
- PublishedEBParticle JournalofAlliedHealth CardinDocument11 pagesPublishedEBParticle JournalofAlliedHealth Cardinag wahyudiNo ratings yet
- Functional Outcome Measures in Physiotherapybridging Evidence Based Practice Function and Our Future 2165 7025.1000e106Document2 pagesFunctional Outcome Measures in Physiotherapybridging Evidence Based Practice Function and Our Future 2165 7025.1000e106Tirumala RaoNo ratings yet
- 1 s2.0 S0965229921000534 MainDocument6 pages1 s2.0 S0965229921000534 MainperawatnanggroeNo ratings yet
- Articles: Massage in HospitalsDocument4 pagesArticles: Massage in HospitalsMenk Leslie Bughao-NavarroNo ratings yet
- CvaDocument10 pagesCvaapi-201999002No ratings yet
- Awareness of Various Aspects of Physiotherapy Among Medical ResidentsDocument6 pagesAwareness of Various Aspects of Physiotherapy Among Medical ResidentsValentina Dela Fuente GarroneNo ratings yet
- Facilitating Case Studies in Massage Therapy CliniDocument5 pagesFacilitating Case Studies in Massage Therapy ClinijorgenovachrolloNo ratings yet
- FT. en EspasticidadDocument6 pagesFT. en Espasticidadrocioag87No ratings yet
- Subgrouping Patients With Low Back PainDocument13 pagesSubgrouping Patients With Low Back PainVladislav KotovNo ratings yet
- Early Intensive Care Unit Mobility Therapy in The Treatment of Acute Respiratory FailureDocument6 pagesEarly Intensive Care Unit Mobility Therapy in The Treatment of Acute Respiratory FailureTakashi NakamuraNo ratings yet
- Manual Therapy: Jenny Setchell, Bernadette Watson, Liz Jones, Michael GardDocument7 pagesManual Therapy: Jenny Setchell, Bernadette Watson, Liz Jones, Michael GardKARENNo ratings yet
- Phys Ther 1992 Farrell 843 52Document12 pagesPhys Ther 1992 Farrell 843 52ubiktrash1492No ratings yet
- Effectiveness of An Extension-OrientedDocument11 pagesEffectiveness of An Extension-OrientedAna Carolina SouzaNo ratings yet
- Ijspt 14 564Document18 pagesIjspt 14 564WaterfloNo ratings yet
- Artigo Numero 3Document13 pagesArtigo Numero 3Bruna AraujoNo ratings yet
- Patient and Family Member Factors Influencing Outcomes of Poststroke Inpatient RehabilitationDocument9 pagesPatient and Family Member Factors Influencing Outcomes of Poststroke Inpatient RehabilitationAdelya YuzyNo ratings yet
- The Impact of Physical Therapy Following Cervical Spine Surgery For Degenerative Spine Disorders: A Systematic ReviewDocument17 pagesThe Impact of Physical Therapy Following Cervical Spine Surgery For Degenerative Spine Disorders: A Systematic ReviewKyle RobinNo ratings yet
- Topic 1Document10 pagesTopic 1Aditi UpadhyayNo ratings yet
- 30.exercise Promotion in Physiotherapy A Qualitative Study Providing Insights Into German Physiotherapists' Practices and ExperiencesDocument7 pages30.exercise Promotion in Physiotherapy A Qualitative Study Providing Insights Into German Physiotherapists' Practices and Experiencesanggie mosqueraNo ratings yet
- Complementary Therapies in MedicineDocument8 pagesComplementary Therapies in Medicinekhadesakshi55No ratings yet
- Manual Therapy One (Updated), March 12Document3 pagesManual Therapy One (Updated), March 12frank andersonNo ratings yet
- Manual Therapy: Jenny Setchell, Bernadette Watson, Liz Jones, Michael GardDocument7 pagesManual Therapy: Jenny Setchell, Bernadette Watson, Liz Jones, Michael Gardanggie mosqueraNo ratings yet
- Clinical Reasoning: Linking Theory To Practice and Practice To TheoryDocument14 pagesClinical Reasoning: Linking Theory To Practice and Practice To Theorylumac1087831No ratings yet
- 09 The Proprioceptive Neuromuscular Facilitationconcept The State of The Evidence A Narrative Review PDFDocument16 pages09 The Proprioceptive Neuromuscular Facilitationconcept The State of The Evidence A Narrative Review PDFdeyana novaNo ratings yet
- 09 The Proprioceptive Neuromuscular Facilitationconcept The State of The Evidence A Narrative ReviewDocument16 pages09 The Proprioceptive Neuromuscular Facilitationconcept The State of The Evidence A Narrative Reviewdeyana novaNo ratings yet
- Physiotherapy Interventions For Shoulder Pain: Cochrane Review AbstractsDocument2 pagesPhysiotherapy Interventions For Shoulder Pain: Cochrane Review Abstractsgemichan26No ratings yet
- AAMT Research Report 10 Oct 11Document51 pagesAAMT Research Report 10 Oct 11S. MihajlovicNo ratings yet
- Essential Physical Therapy Terminology: Navigating Physical Therapy LanguageFrom EverandEssential Physical Therapy Terminology: Navigating Physical Therapy LanguageNo ratings yet
- A Case for Looking: Bridging the Technical and the SpiritualFrom EverandA Case for Looking: Bridging the Technical and the SpiritualNo ratings yet
- 4 - Walking Movement Analysis WorksheetDocument4 pages4 - Walking Movement Analysis WorksheetSM199021No ratings yet
- 2 - Sit To Stand Movement Analysis WorksheetDocument3 pages2 - Sit To Stand Movement Analysis WorksheetSM199021No ratings yet
- 2021 - QoL in MSisdominated by Fatigue - Disability - Sefl-EfficacyDocument7 pages2021 - QoL in MSisdominated by Fatigue - Disability - Sefl-EfficacySM199021No ratings yet
- ARTG - 2020 - Intensive Care Admission and Early Neuro-Rehabilitation. Lessons For COVID-19Document10 pagesARTG - 2020 - Intensive Care Admission and Early Neuro-Rehabilitation. Lessons For COVID-19SM199021No ratings yet
- Telerehabilitation For People With Physical Disabilities and Movement Impairment Development and Evaluation of An Online Toolkit For PractitionersDocument9 pagesTelerehabilitation For People With Physical Disabilities and Movement Impairment Development and Evaluation of An Online Toolkit For PractitionersSM199021No ratings yet
- 2013 - Patients - Carers - Providers Experiences To Support in Self-Management MSDocument11 pages2013 - Patients - Carers - Providers Experiences To Support in Self-Management MSSM199021No ratings yet
- Truijen2022 Article EffectOfHome-basedVirtualRealiDocument12 pagesTruijen2022 Article EffectOfHome-basedVirtualRealiSM199021No ratings yet
- My - Lectures.Updated - II 2015Document137 pagesMy - Lectures.Updated - II 2015prasadmvk100% (1)
- UQRCS Research Proposal TemplateDocument4 pagesUQRCS Research Proposal TemplateNasser QassemNo ratings yet
- Ffiffl: Office of The Controller of ExaminationsDocument4 pagesFfiffl: Office of The Controller of Examinationssunny rahmanNo ratings yet
- Hygeia HMO Senior Plans Proposal - 2023 - UpdatedDocument2 pagesHygeia HMO Senior Plans Proposal - 2023 - UpdatedTaiwo ShotuboNo ratings yet
- Mh25 Borderline Personality GuidelineDocument182 pagesMh25 Borderline Personality GuidelineAbdul Hakim Abdul KadirNo ratings yet
- Dosis Obat PediatriDocument10 pagesDosis Obat PediatriKris AdiNo ratings yet
- NCM 106 PHARMACOLOGY 1st SEMESTER MIDTERM REVIEWERDocument11 pagesNCM 106 PHARMACOLOGY 1st SEMESTER MIDTERM REVIEWEREzra MaeNo ratings yet
- Messer & Wampold - 2002 - Nonspecific Factors of ChangeDocument5 pagesMesser & Wampold - 2002 - Nonspecific Factors of ChangeAnton ShcherbakovNo ratings yet
- Data Master OkDocument128 pagesData Master OkGudang farmasi Rs TandunNo ratings yet
- Cea Hipertensi 8Document7 pagesCea Hipertensi 8ani rahayuNo ratings yet
- Dialogue Group III CP Spatic Quadriplegia GMFCS IV-1Document3 pagesDialogue Group III CP Spatic Quadriplegia GMFCS IV-1Maulida ZahroNo ratings yet
- Principles of Chinese Medicine - A Modern Interpretation PDFDocument258 pagesPrinciples of Chinese Medicine - A Modern Interpretation PDFAndrija100% (1)
- Group CounselingDocument5 pagesGroup CounselingAlam ZebNo ratings yet
- Book Review of The Study of Music Therapy: Current Issues and Concepts by Kenneth AigenDocument3 pagesBook Review of The Study of Music Therapy: Current Issues and Concepts by Kenneth AigenRenato Cardoso SilvaNo ratings yet
- Managing Difficult Patient Encounters (AAFP 2023)Document7 pagesManaging Difficult Patient Encounters (AAFP 2023)Breno Resende Rodrigues CunhaNo ratings yet
- Rekapitulasi Februari 2023Document13 pagesRekapitulasi Februari 2023hanafiNo ratings yet
- MR (Medical Representative) - 28Document2 pagesMR (Medical Representative) - 28rakesharain123No ratings yet
- The Family Journal: Family Art Therapy: The Joint Family Holiday DrawingDocument4 pagesThe Family Journal: Family Art Therapy: The Joint Family Holiday DrawingGuadalupe PérezNo ratings yet
- Psychotherapy and Counselling in Practice A Digby Annas ArchiveDocument335 pagesPsychotherapy and Counselling in Practice A Digby Annas ArchiveAlina MolesagNo ratings yet
- Opioid Conversion Ratios - Guide To Practice 2010: Released December 2010Document12 pagesOpioid Conversion Ratios - Guide To Practice 2010: Released December 2010Ronald WaiNo ratings yet
- Drug Abuse & Prevention Word DockDocument9 pagesDrug Abuse & Prevention Word DockBasmah AnsariNo ratings yet
- Acupressure: By: Tabor, Jonelle, Tan Giomarie & Patricia ValentinDocument13 pagesAcupressure: By: Tabor, Jonelle, Tan Giomarie & Patricia ValentinRoseanne Legaspi CasayuranNo ratings yet
- Unit 1, Herbal Drug Technology, B Pharmacy 6th Sem, Carewell PharmaDocument37 pagesUnit 1, Herbal Drug Technology, B Pharmacy 6th Sem, Carewell Pharmawritters2023No ratings yet
- MTinMedicine DileoDocument10 pagesMTinMedicine DileoFernando OliveiraNo ratings yet
- Alternative Therapies - Monika MakwanaDocument6 pagesAlternative Therapies - Monika Makwanamonika makwanaNo ratings yet