You might also like
- Living Beyond Lyme: Reclaim Your Life From Lyme Disease and Chronic IllnessFrom EverandLiving Beyond Lyme: Reclaim Your Life From Lyme Disease and Chronic IllnessNo ratings yet
- Work Makes Me Nervous: Overcome Anxiety and Build the Confidence to SucceedFrom EverandWork Makes Me Nervous: Overcome Anxiety and Build the Confidence to SucceedNo ratings yet
- Offshore Pre Asses FormDocument8 pagesOffshore Pre Asses Formwendyphan09No ratings yet
- Rosepark 2Document3 pagesRosepark 2schroderanzelNo ratings yet
- Health Surveillance QuestionaireDocument5 pagesHealth Surveillance QuestionaireTrinidad InspectionNo ratings yet
- 5f46c432d9030864565565a15bd2c OriginalDocument7 pages5f46c432d9030864565565a15bd2c OriginalFawwaaz DamareeNo ratings yet
- Do You Have Any of The Following DiseasesDocument6 pagesDo You Have Any of The Following DiseasesYasmin SawyerNo ratings yet
- Multitable New Patient FormDocument8 pagesMultitable New Patient Forme-MedTools100% (9)
- IPL Client History v1 - 7Document8 pagesIPL Client History v1 - 7Karen Dodd100% (1)
- Preliminary Underwriting ApplicationDocument7 pagesPreliminary Underwriting ApplicationProvada Insurance ServicesNo ratings yet
- Adult New Patient FormsDocument10 pagesAdult New Patient FormsCrossNCloud8346No ratings yet
- Health History Form: Dental InformationDocument2 pagesHealth History Form: Dental Informationdarren phamNo ratings yet
- Flu Vaccine Form: Screening QuestionnaireDocument1 pageFlu Vaccine Form: Screening Questionnairesteve bestNo ratings yet
- Application FormDocument2 pagesApplication FormBrookeNo ratings yet
- Employment Application Form 2022Document3 pagesEmployment Application Form 2022paulinemahlangu88No ratings yet
- New-Patient-Forms-All-2020 GoodDocument8 pagesNew-Patient-Forms-All-2020 GoodCheryl WanNo ratings yet
- PacificcareDocument12 pagesPacificcareCourage MlamboNo ratings yet
- Occupational Health Pre-Employment Health Assessment Form March 08Document4 pagesOccupational Health Pre-Employment Health Assessment Form March 08queenmombi100% (2)
- Reon Energy Solution Health Status Questionnare (HSQ)Document2 pagesReon Energy Solution Health Status Questionnare (HSQ)arbab201No ratings yet
- ESP-Accepting Patient in Radiology Department-D3 RadiologiDocument13 pagesESP-Accepting Patient in Radiology Department-D3 RadiologiTest Music CopyrightNo ratings yet
- Kaiser International: Healthgroup, Inc. ®Document5 pagesKaiser International: Healthgroup, Inc. ®Metina MontecilloNo ratings yet
- Client Intake Form For Energy HealingDocument3 pagesClient Intake Form For Energy HealingLasha KvaraNo ratings yet
- Station 5Document2 pagesStation 5Mohammad Neyazur RahamanNo ratings yet
- Facial Consent Form 04Document2 pagesFacial Consent Form 04Miki LeeNo ratings yet
- Company Health Insurance Application: Important InformationDocument8 pagesCompany Health Insurance Application: Important InformationMayar RagabNo ratings yet
- Workplace Health Questionnaire (New Starter)Document4 pagesWorkplace Health Questionnaire (New Starter)zaied abdulhadiNo ratings yet
- Pre-Placement Health Assessment FormDocument5 pagesPre-Placement Health Assessment FormRGanjvarNo ratings yet
- Job Application Form HM 2021 WordDocument7 pagesJob Application Form HM 2021 WordKhan GeNo ratings yet
- Medical Certificate 2Document2 pagesMedical Certificate 2Aditeya Shukla100% (1)
- Sari FormsDocument3 pagesSari FormsJohnasse Sebastian NavalNo ratings yet
- 2013 MedicalsDocument5 pages2013 MedicalsSebastia Felipe SolisNo ratings yet
- Employee Health Evaluation & Enrollment Form: Corporate Solutions IncorporatedDocument2 pagesEmployee Health Evaluation & Enrollment Form: Corporate Solutions IncorporatedMitchell BigleyNo ratings yet
- Health Questionnaire TemplateDocument2 pagesHealth Questionnaire TemplateBaxwal AxmedNo ratings yet
- Pre Employment Health AssessmentDocument7 pagesPre Employment Health AssessmentMP13No ratings yet
- MenHealth Questionnaire A4 4PRINT 1Q2017Document2 pagesMenHealth Questionnaire A4 4PRINT 1Q2017khaiberNo ratings yet
- UAHSF STD Claim Form - APSDocument6 pagesUAHSF STD Claim Form - APSBenjamin AlexanderNo ratings yet
- New Employee Medical QuestionnaireDocument2 pagesNew Employee Medical QuestionnaireRichard R M ThodéNo ratings yet
- Patient Application Tech WritingDocument2 pagesPatient Application Tech Writingapi-272574963No ratings yet
- Medical Application Form: Insured Name: Inception DateDocument3 pagesMedical Application Form: Insured Name: Inception DateDidier G PeñuelaNo ratings yet
- Health History Form 03Document2 pagesHealth History Form 03IñakiNo ratings yet
- Medical CertificateDocument2 pagesMedical CertificatelekacaNo ratings yet
- Meeting 1-General Assessment (Repaired)Document3 pagesMeeting 1-General Assessment (Repaired)Indah Yulinda PramestyNo ratings yet
- Libro ComplementarioDocument155 pagesLibro ComplementarioKowe xDNo ratings yet
- Client Intake Form: Date Patient Last: First Initial Address City Zip Date of Birth Phone CellDocument6 pagesClient Intake Form: Date Patient Last: First Initial Address City Zip Date of Birth Phone Celljayson_tamayo2No ratings yet
- Pre-Employment Physical FormDocument1 pagePre-Employment Physical FormKarthik SNo ratings yet
- Pre Employment Medical Declaration Form - 2022Document2 pagesPre Employment Medical Declaration Form - 2022Neel GhoshNo ratings yet
- Hello!: New Patient Questionnaire Name: DobDocument11 pagesHello!: New Patient Questionnaire Name: DobDavid LawrenceNo ratings yet
- Medical History QuestionnaireDocument3 pagesMedical History QuestionnaireIrene IonescuNo ratings yet
- Consent For Eyebrow Drawing Using Microblading TechniqueDocument4 pagesConsent For Eyebrow Drawing Using Microblading TechniquekeziamachadoNo ratings yet
- Companion Screening FormDocument1 pageCompanion Screening FormjajameimeiNo ratings yet
- Prin. L.N.Welingkar Institute of Management Development and ResearchDocument4 pagesPrin. L.N.Welingkar Institute of Management Development and ResearchKavish JainNo ratings yet
- New Patient FormDocument7 pagesNew Patient Forme-MedTools100% (4)
- English For The Professional Nurse: Part 1: Collecting Demographic Data ElementsDocument5 pagesEnglish For The Professional Nurse: Part 1: Collecting Demographic Data ElementsLestari RahayuNo ratings yet
- Final Life Insurance QuestionnaireDocument6 pagesFinal Life Insurance QuestionnaireVishal GuptaNo ratings yet
- Maternity Unit Antenatal Assessment Referral FormDocument2 pagesMaternity Unit Antenatal Assessment Referral FormJyoti Prem UttamNo ratings yet
- Narayana Health - Consumer QuestionnaireDocument3 pagesNarayana Health - Consumer QuestionnairedivijnathNo ratings yet
- Medical History FormDocument4 pagesMedical History FormHeide Basing-aNo ratings yet
- Envelope - Medical Application Form - New - V3 - Mednet - 1Document3 pagesEnvelope - Medical Application Form - New - V3 - Mednet - 1muhdm7771No ratings yet
- High BPDocument2 pagesHigh BPROYNo ratings yet
- CBT Intake AssessmentDocument4 pagesCBT Intake AssessmentTijana StojkovicNo ratings yet
- Tumor Markers: Universiti Kuala Lumpur (Unikl) - Where Knowledge Is Applied and Dreams RealizedDocument29 pagesTumor Markers: Universiti Kuala Lumpur (Unikl) - Where Knowledge Is Applied and Dreams RealizedNida RidzuanNo ratings yet
- Unclear Outcomes of Heart Rate Variability Following A Concussion: A Systematic ReviewDocument15 pagesUnclear Outcomes of Heart Rate Variability Following A Concussion: A Systematic ReviewMahdi HosseiniNo ratings yet
- ICD 10 CM 2023 Changes and Updates AssessmentDocument7 pagesICD 10 CM 2023 Changes and Updates AssessmentAzra MuzafarNo ratings yet
- Radiographic Pathology For Technologists 7th Edition Kowalczyk Test BankDocument26 pagesRadiographic Pathology For Technologists 7th Edition Kowalczyk Test BankJamesGonzalezwbpg100% (42)
- Concept Map - Colon CancerDocument2 pagesConcept Map - Colon Cancerbea pegadNo ratings yet
- Day 1. Mohd Sami 1Document67 pagesDay 1. Mohd Sami 1Baebee LouNo ratings yet
- Revised Antibiotic Microbial ChecklistDocument1 pageRevised Antibiotic Microbial ChecklistNur Farihan OthmanNo ratings yet
- TNM Staging For Breast Cancer - Cancer Research UKDocument8 pagesTNM Staging For Breast Cancer - Cancer Research UKSanket TelangNo ratings yet
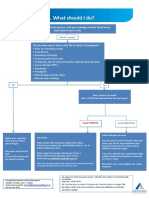
- What To Do If Youre Sick FlowchartDocument1 pageWhat To Do If Youre Sick FlowchartfuckyouNo ratings yet
- Standard Operating Procedure (SOP) For On-Call Emergency Out of Hours Haemodialysis For Renal PatientsDocument23 pagesStandard Operating Procedure (SOP) For On-Call Emergency Out of Hours Haemodialysis For Renal PatientsShahriar MohammodNo ratings yet
- Bacteria Viruses Lesson PlanDocument7 pagesBacteria Viruses Lesson Planapi-665322772No ratings yet
- Folfiri+cetu Gi Col PDocument12 pagesFolfiri+cetu Gi Col PJayelle2No ratings yet
- Vertigo Maneuvers Epley, Semont, Foster, and Brandt-DaroffDocument5 pagesVertigo Maneuvers Epley, Semont, Foster, and Brandt-DaroffIdoNo ratings yet
- Trastornos de Alimentacion CIE 11Document19 pagesTrastornos de Alimentacion CIE 11Elene MezaNo ratings yet
- 11 FNSDDocument16 pages11 FNSDVamsi VasishtNo ratings yet
- Neurosis VS PsychosisDocument1 pageNeurosis VS Psychosissisiner09 DascăluNo ratings yet
- NCMB317 Lec MidtermDocument55 pagesNCMB317 Lec Midterm2 - GUEVARRA, KYLE JOSHUA M.No ratings yet
- Viral Infections of The Gastrointestinal Tract and Viral Infections of The Genitourinary SystemDocument14 pagesViral Infections of The Gastrointestinal Tract and Viral Infections of The Genitourinary SystemDARLENE CLAIRE ANDEZANo ratings yet
- Cerebralamyloid Angiopathy: Laszlo Szidonya,, Joshua P. NickersonDocument12 pagesCerebralamyloid Angiopathy: Laszlo Szidonya,, Joshua P. NickersonJuan Carlos LazoNo ratings yet
- OsteoporosisDocument22 pagesOsteoporosisPrachi DSaNo ratings yet
- Shazia Kazi UpdatedDocument4 pagesShazia Kazi Updatedshazia kazi100% (1)
- OSPE (Hematology)Document19 pagesOSPE (Hematology)Taha100% (1)
- Symptoms Board Game EslDocument4 pagesSymptoms Board Game EslNguyễn LinhNo ratings yet
- OHSS Case Presentation Discussion - Jindal IVF CHDDocument41 pagesOHSS Case Presentation Discussion - Jindal IVF CHDJindal IVF ChandigarhNo ratings yet
- Domestic Violence PresentationDocument9 pagesDomestic Violence PresentationShahanaj Akther TamannaNo ratings yet
- FlagellatesDocument64 pagesFlagellatesRandy BerryNo ratings yet
- Nursing Care of Child With Thalassemia and LeukemiaDocument60 pagesNursing Care of Child With Thalassemia and LeukemiaJanicex FongNo ratings yet
- Seizures/Epilepsy: Case PersentationDocument14 pagesSeizures/Epilepsy: Case PersentationAbdulmalik AliNo ratings yet
- APA Eating Disorder Clinical Practice Guideline Training SlidesDocument66 pagesAPA Eating Disorder Clinical Practice Guideline Training SlidesayyuuafufaaNo ratings yet
- PRULady PDS 2024 1704762736Document6 pagesPRULady PDS 2024 1704762736shirley lee wenNo ratings yet