You might also like
- Maersk Doha: Report On The Investigation of The Machinery Breakdown and Subsequent Fire OnboardDocument46 pagesMaersk Doha: Report On The Investigation of The Machinery Breakdown and Subsequent Fire OnboardShyam Kishore100% (1)
- 27-Fatal Boiler ExplosionDocument2 pages27-Fatal Boiler ExplosionLACC50No ratings yet
- 3) EX 5,02. Accident Analysis ExerciseDocument6 pages3) EX 5,02. Accident Analysis ExerciseAndrejSukoraNo ratings yet
- Mars 243Document4 pagesMars 243CostasKNo ratings yet
- Investigarea Unui Incendiu La Bordul NaveiDocument5 pagesInvestigarea Unui Incendiu La Bordul NaveiSilviu NistorNo ratings yet
- Case StudyDocument15 pagesCase Study2178-gme39-jaydeepNo ratings yet
- CompleteDocument35 pagesCompleteJay JayNo ratings yet
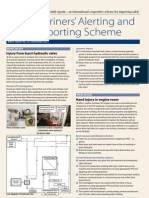
- Mariners' Alerting and Reporting Scheme: Injury From Burst Hydraulic ValveDocument4 pagesMariners' Alerting and Reporting Scheme: Injury From Burst Hydraulic ValveCostasKNo ratings yet
- .CSC Boiler Explosion PDFDocument4 pages.CSC Boiler Explosion PDFadula paulinaNo ratings yet
- Lessons Learned From Marine Casualties (III 6/15, Annex 3)Document15 pagesLessons Learned From Marine Casualties (III 6/15, Annex 3)Prince DhakaNo ratings yet
- Report of Investigation Into The Engine Room Fire On Board The Hong Kong Registered ShipDocument18 pagesReport of Investigation Into The Engine Room Fire On Board The Hong Kong Registered Shipalina_inaNo ratings yet
- Case Study - ER Fire and Failure of FIxed Fire Fighting SystemsDocument2 pagesCase Study - ER Fire and Failure of FIxed Fire Fighting SystemsHarman SandhuNo ratings yet
- Case Study HMS Endurance StudentDocument5 pagesCase Study HMS Endurance StudentPrasanga MallawaarachchiNo ratings yet
- Fire Report FinalDocument5 pagesFire Report FinalQuentin DidierNo ratings yet
- Piper Alpha Background & ShortcomingsDocument4 pagesPiper Alpha Background & Shortcomingsfashwin0% (1)
- HTTP WWW - Maib.gov - Uk Cms Resources - CFM File Yeoman Bontrup SynopsisDocument1 pageHTTP WWW - Maib.gov - Uk Cms Resources - CFM File Yeoman Bontrup SynopsisIoana PetcuNo ratings yet
- MARS 227 September 2011Document4 pagesMARS 227 September 2011captkcNo ratings yet
- ИнгDocument3 pagesИнгАртём АржинтNo ratings yet
- Fire Investigation ReportDocument3 pagesFire Investigation ReportMarius SykaaNo ratings yet
- SF 08 22Document6 pagesSF 08 22Shivkumar JadhavNo ratings yet
- CR British Valour Crankcase ExplosionDocument23 pagesCR British Valour Crankcase ExplosionjameswdanielsNo ratings yet
- Case Study Fire On Board and Sinking of A Restricted Limits Passenger VesselDocument2 pagesCase Study Fire On Board and Sinking of A Restricted Limits Passenger VesselAndreas IoannouNo ratings yet
- Case Study - Fire Incident On MV of SPMDocument4 pagesCase Study - Fire Incident On MV of SPMHedi Ben MohamedNo ratings yet
- Investigation Reportsuncor Altares PDFDocument12 pagesInvestigation Reportsuncor Altares PDFR GunalanNo ratings yet
- A Case Study of The Boiler AccidentDocument11 pagesA Case Study of The Boiler AccidentZekie Lee100% (1)
- NarrativeDocument7 pagesNarrativeSandeep KumarNo ratings yet
- MARS 230 December 2011Document4 pagesMARS 230 December 2011captkcNo ratings yet
- Safety Digest 1 1995Document31 pagesSafety Digest 1 1995Gwyn WilliamsNo ratings yet
- Case Study: Unattended Burning Candles, Inoperable Fire-Detection System Caused $6.78M in DamageDocument17 pagesCase Study: Unattended Burning Candles, Inoperable Fire-Detection System Caused $6.78M in DamageonlieoussamaNo ratings yet
- Unit C Element 2Document10 pagesUnit C Element 2w hiteNo ratings yet
- Unit C Element 2Document9 pagesUnit C Element 2rahularenNo ratings yet
- Boiler ExplosionDocument25 pagesBoiler ExplosionmahaveenNo ratings yet
- Boiler Explosion (Exxon Singapore)Document25 pagesBoiler Explosion (Exxon Singapore)danish873100% (1)
- Fire ReportDocument3 pagesFire ReportGabriela Iftimie100% (1)
- MJV Safety Culture (NL) - Safety Culture and AccidentsDocument8 pagesMJV Safety Culture (NL) - Safety Culture and AccidentsHesham HamyNo ratings yet
- Piper AlphaDocument6 pagesPiper AlphaAhmed Eldeeb100% (1)
- National Transportation Safety Board: Marine Accident BriefDocument5 pagesNational Transportation Safety Board: Marine Accident BriefAnonymous 3aPuAaiNo ratings yet
- Piper Alpha IncidentDocument31 pagesPiper Alpha IncidentKhairul ZakirinNo ratings yet
- SS Norway Boiler ExplosionDocument1 pageSS Norway Boiler Explosiontjtheboater95No ratings yet
- Casualty Circular No. 2 of 2006Document2 pagesCasualty Circular No. 2 of 2006Ajay SinghNo ratings yet
- Texas City Refinery Explosion - WikipediaDocument18 pagesTexas City Refinery Explosion - WikipediaMOHAN RAVICHANDRANNo ratings yet
- Paris MouDocument24 pagesParis MouPrince DhakaNo ratings yet
- MD 518 Suitability SurveyDocument4 pagesMD 518 Suitability SurveylamsoncoegNo ratings yet
- Fire in The Engine Room: MARS 2021Document3 pagesFire in The Engine Room: MARS 2021Praveen AbisakeNo ratings yet
- Epcsm Term PaperDocument13 pagesEpcsm Term PaperFake accNo ratings yet
- Accident ENG 1.1Document6 pagesAccident ENG 1.1Tom MoritzNo ratings yet
- MO-2022-001 Final ReportDocument13 pagesMO-2022-001 Final ReportguigikikoNo ratings yet
- Learning 6Document1 pageLearning 6iomerkoNo ratings yet
- Ex 2.01 Human Error Chain in An AccidentDocument5 pagesEx 2.01 Human Error Chain in An AccidentAndrejSukoraNo ratings yet
- Tmi NotesDocument2 pagesTmi Notesgeorge aarthiNo ratings yet
- Executive Summary WIPP Underground Fire Report 03 12 2014Document12 pagesExecutive Summary WIPP Underground Fire Report 03 12 2014Brian FoxNo ratings yet
- 709 Turbocharger ExplosionDocument2 pages709 Turbocharger ExplosionTimmyJuriNo ratings yet
- Turbocharger Explosion and Engine Room Fire: Marine Technical LibraryDocument2 pagesTurbocharger Explosion and Engine Room Fire: Marine Technical LibraryNoui BouzidNo ratings yet
- Crankcase Explosion Casualty Investigation British ValourDocument23 pagesCrankcase Explosion Casualty Investigation British Valoursevero97100% (1)
- LFI H2S Gas Release Leading To Fatallity From HeightDocument3 pagesLFI H2S Gas Release Leading To Fatallity From HeightRusman PribadiNo ratings yet
- Dry DockDocument80 pagesDry DockSwopon MollahNo ratings yet
- A Guide to Ship Repair Estimates in Man-hoursFrom EverandA Guide to Ship Repair Estimates in Man-hoursRating: 4.5 out of 5 stars4.5/5 (5)
- D155A-6 Power Train System: Dubai Training and Demonstration CenterDocument20 pagesD155A-6 Power Train System: Dubai Training and Demonstration CenterMichael DavidNo ratings yet
- ELT - 213 - 1 Offshore Repair of The IFA 2000 Cross-Channel Link (2004) PDFDocument7 pagesELT - 213 - 1 Offshore Repair of The IFA 2000 Cross-Channel Link (2004) PDFNam Hoai LeNo ratings yet
- DI16Document2 pagesDI16Erln LimaNo ratings yet
- ZukaBaby Baby Gift Registry Favorites 2021Document1 pageZukaBaby Baby Gift Registry Favorites 2021Peter CampolaNo ratings yet
- Saurian StarhostDocument1 pageSaurian StarhostafwsefwefvNo ratings yet
- Imoca 60 RC Work Breakdown StructureDocument1 pageImoca 60 RC Work Breakdown StructureSardar PerdawoodNo ratings yet
- Albany Police Dept Arrest Summary ReportDocument4 pagesAlbany Police Dept Arrest Summary ReportBryan FitzgeraldNo ratings yet
- Lloyd's - Register 2018Document188 pagesLloyd's - Register 2018Pranesh SbNo ratings yet
- Director Production Operations Manufacturing in Columbus OH Resume Todd BejsovecDocument2 pagesDirector Production Operations Manufacturing in Columbus OH Resume Todd BejsovecToddBejsovecNo ratings yet
- Summer Training Report NTPCDocument45 pagesSummer Training Report NTPCChetan MeenaNo ratings yet
- Meritor ABS TrainingDocument108 pagesMeritor ABS Trainingford62b100% (3)
- As Conditions and Safe Navigation Permit, Our Suggested Route Remains ValidDocument2 pagesAs Conditions and Safe Navigation Permit, Our Suggested Route Remains ValidIonut GabrielNo ratings yet
- rc38 Recs For Frost Protection Measures For Sprinklers PDFDocument12 pagesrc38 Recs For Frost Protection Measures For Sprinklers PDFNahado DMNo ratings yet
- Ac 43.9-1e, Instructions For Completion of Faa Form 337 (Omb No (1) - 2120-0020), Major Repair and AlteraDocument5 pagesAc 43.9-1e, Instructions For Completion of Faa Form 337 (Omb No (1) - 2120-0020), Major Repair and Alterabobbyo56No ratings yet
- 480-EIA Manual of Recommended Safety Practices - IndexDocument4 pages480-EIA Manual of Recommended Safety Practices - Indexkirandevi1981No ratings yet
- Second Avenue Subway ReviewDocument8 pagesSecond Avenue Subway ReviewCity Room100% (2)
- 2 Review Sand Detachment Modern Deep Marine Environments Upslope Stratigraphic Traps (01-03)Document3 pages2 Review Sand Detachment Modern Deep Marine Environments Upslope Stratigraphic Traps (01-03)Douglas Ribeiro AntunesNo ratings yet
- Avl PDFDocument52 pagesAvl PDFAhmet HamamcıoğluNo ratings yet
- Terex Peiner SK315 PDFDocument6 pagesTerex Peiner SK315 PDFJhony Espinoza Perez0% (1)
- Aerodrome Traffic Circuit.Document10 pagesAerodrome Traffic Circuit.Vinay SinghNo ratings yet
- Odc GTDocument2 pagesOdc GTDinoNo ratings yet
- Comparative Study of Maruti and HyundaiDocument65 pagesComparative Study of Maruti and HyundaiPitabash Behera52% (23)
- Jsa (Job Safety Analysis)Document2 pagesJsa (Job Safety Analysis)Ruben Mejia100% (1)
- BPW Meeting: Agenda ItemsDocument34 pagesBPW Meeting: Agenda ItemsJeffrey SteinNo ratings yet
- CFR, Cif, Fob, DapDocument18 pagesCFR, Cif, Fob, DapthuyluuNo ratings yet
- Airframe PDFDocument124 pagesAirframe PDFskynorthNo ratings yet
- Fabrication of Structural and Miscellaneous Steel Supplier Drawing & Data Commitment (SDDC) FormDocument7 pagesFabrication of Structural and Miscellaneous Steel Supplier Drawing & Data Commitment (SDDC) FormEl_memitoNo ratings yet
- SCLMDocument45 pagesSCLMkeerthana chandrasekarNo ratings yet
- BNI Feature PresentationDocument18 pagesBNI Feature PresentationK4 TOUR WORLDNo ratings yet
- Chapter 17 Notes (Brinkley)Document6 pagesChapter 17 Notes (Brinkley)Annie LeeNo ratings yet