You might also like
- Knee ExaminationDocument54 pagesKnee ExaminationZed HarrisNo ratings yet
- Knee Examination OSCE GuideDocument23 pagesKnee Examination OSCE GuideAaron Nameer Abrar RahmanNo ratings yet
- Ankle Fractures: Winda Alviranisa/20204010293 Pembimbing: Dr. Muhammad Pandu Nugraha, SP - OTDocument28 pagesAnkle Fractures: Winda Alviranisa/20204010293 Pembimbing: Dr. Muhammad Pandu Nugraha, SP - OTwinda alviraNo ratings yet
- Ankle and Foot PatternsDocument119 pagesAnkle and Foot PatternsshmishivendNo ratings yet
- Deformities of Greater and Lesser ToesDocument20 pagesDeformities of Greater and Lesser ToesSylvia ChongNo ratings yet
- The Soulmate DietDocument24 pagesThe Soulmate DietShana MarieNo ratings yet
- Rheumatology Examination: Physical Examination-N ManoliosDocument7 pagesRheumatology Examination: Physical Examination-N ManoliosRohit SharmaNo ratings yet
- Ankle Instability: Dr. Syarif Hidayatullah, SP - OT, M.KesDocument75 pagesAnkle Instability: Dr. Syarif Hidayatullah, SP - OT, M.Kesahmad zakyNo ratings yet
- Hallux Valgus (Bunion), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHallux Valgus (Bunion), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Regional Anesthesia in OtolaryngologyDocument85 pagesRegional Anesthesia in OtolaryngologyleocitraNo ratings yet
- Special Needs Children CategoriesDocument10 pagesSpecial Needs Children CategoriesJoe Well100% (1)
- Ortho Lec Knee OrthopaedicsDocument45 pagesOrtho Lec Knee OrthopaedicsNadeen GhazalNo ratings yet
- Babita Blood TestDocument11 pagesBabita Blood TestHimanshu tyagiNo ratings yet
- Ankle and FootDocument31 pagesAnkle and FootmetoNo ratings yet
- Tr90 Flyer Eng (4 Pages)Document4 pagesTr90 Flyer Eng (4 Pages)Cherry San Diego0% (1)
- Meningococcal MeningitisDocument22 pagesMeningococcal MeningitisShuvashishSunuwar100% (1)
- Foot and AnkleDocument58 pagesFoot and Anklekyliever100% (1)
- Eye Care Activity For ChildrenDocument12 pagesEye Care Activity For ChildrenAngelina Tan Rong XuanNo ratings yet
- Hallus Valgus and VarusDocument37 pagesHallus Valgus and VarusAyesha ShafiqNo ratings yet
- Hallux VarusDocument12 pagesHallux VarusZam PamateNo ratings yet
- 4 - Ankle and FootDocument65 pages4 - Ankle and Footxj74fr4ddxNo ratings yet
- Knee&Foot Part2Document26 pagesKnee&Foot Part2SarkawtNo ratings yet
- MUSCULOSKELETALDocument27 pagesMUSCULOSKELETALCassandra Mae PerochoNo ratings yet
- Limb Length Discrepancy: Amputation Versus Reconstruction For Fibular HemimeliaDocument5 pagesLimb Length Discrepancy: Amputation Versus Reconstruction For Fibular HemimeliaAlfred JacksonNo ratings yet
- Flatfoot Deformity An OverviewDocument9 pagesFlatfoot Deformity An OverviewpetcudanielNo ratings yet
- Hallux ValgusDocument19 pagesHallux Valgushacker ammerNo ratings yet
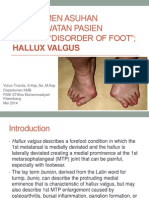
- Manajemen Asuhan Keperawatan Pasien Dengan Disorder of Foot Hammer Toe and Hallux Valgus FREEDocument29 pagesManajemen Asuhan Keperawatan Pasien Dengan Disorder of Foot Hammer Toe and Hallux Valgus FREENovita DamaiyantiNo ratings yet
- Surgical Reconstruction For Fibular HemimeliaDocument27 pagesSurgical Reconstruction For Fibular HemimeliaArditya yudistiraNo ratings yet
- Fibular Hemimelia FAQsDocument11 pagesFibular Hemimelia FAQsLucila LugoNo ratings yet
- Hallux VarusDocument4 pagesHallux VarusmadziiieNo ratings yet
- Hallux Valgus2014Document6 pagesHallux Valgus2014isx hdzNo ratings yet
- Foot Orthotics - FDLDocument19 pagesFoot Orthotics - FDLDiamoniq AyuningtiaNo ratings yet
- Ankle DislocationDocument18 pagesAnkle DislocationKaiwalyaNo ratings yet
- Hallux ValgusDocument16 pagesHallux ValgusucssNo ratings yet
- Deformities: Learning ObjectiveDocument4 pagesDeformities: Learning ObjectiveEimad AtifNo ratings yet
- Deformities of FootDocument10 pagesDeformities of FootShehin SalimNo ratings yet
- Colles FractureDocument3 pagesColles FractureDivya RanasariaNo ratings yet
- 30.ankle & Foot DiseasesDocument46 pages30.ankle & Foot DiseasesDuha HamidNo ratings yet
- Clinical ExaminationDocument6 pagesClinical Examinationarvind appNo ratings yet
- Lec 19 DEFORMITIES OF FOOT UpdatedDocument9 pagesLec 19 DEFORMITIES OF FOOT UpdatedMaheen IrfanNo ratings yet
- Adult-Acquired Flatfoot DeformityDocument8 pagesAdult-Acquired Flatfoot DeformityC Martin TraumatoNo ratings yet
- Ankle ExamDocument6 pagesAnkle ExamHarris TaheryNo ratings yet
- LUMBAR DISC NotesDocument7 pagesLUMBAR DISC NotesPrasadNo ratings yet
- pGALS Examination OSCE GuideDocument18 pagespGALS Examination OSCE GuideFanny PritaningrumNo ratings yet
- Congenital Talipes Equino Varus (Ctev) - Nur HanisahDocument11 pagesCongenital Talipes Equino Varus (Ctev) - Nur HanisahNur HanisahNo ratings yet
- Definition: Is A Condition Resulting in Partial or Complete Separation of A Segment of Normal Hyaline Cartilage From It's Supporting BoneDocument8 pagesDefinition: Is A Condition Resulting in Partial or Complete Separation of A Segment of Normal Hyaline Cartilage From It's Supporting BoneKarla Chariz Fernandez BayagNo ratings yet
- Pes PlanusDocument18 pagesPes Planushacker ammerNo ratings yet
- Painfull Accessory Navicular BoneDocument29 pagesPainfull Accessory Navicular BoneAmmar MahdiNo ratings yet
- Pes Planus - Flat FeetDocument9 pagesPes Planus - Flat Feetumermudassir619No ratings yet
- Ankle&fEET Written Procedure-MagsombolDocument2 pagesAnkle&fEET Written Procedure-Magsombolhazell_aseronNo ratings yet
- Musculoskeletal Abnormal FindingsDocument8 pagesMusculoskeletal Abnormal FindingstmmrsptlnNo ratings yet
- Hallux Varus, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHallux Varus, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Decision Making in The Treatment of Hallux Valgus: Thomas N. Joseph, M.D., and Kenneth J. Mroczek, M.DDocument5 pagesDecision Making in The Treatment of Hallux Valgus: Thomas N. Joseph, M.D., and Kenneth J. Mroczek, M.Ddanieldrev1No ratings yet
- Examination of The Hip Joint: Dr. Pallav AgrawalDocument66 pagesExamination of The Hip Joint: Dr. Pallav AgrawalJohn Agana AyamgaNo ratings yet
- BY Gayathri G.V BPT 2 Year SRM College of PhysiotherapyDocument7 pagesBY Gayathri G.V BPT 2 Year SRM College of PhysiotherapyjothiNo ratings yet
- VSR 511 Veterinary Orthopedics and LamenessDocument311 pagesVSR 511 Veterinary Orthopedics and LamenessChandan PatilNo ratings yet
- Hallux Valgus ReportDocument2 pagesHallux Valgus Reportapi-282474245No ratings yet
- ISMT12 - Day 244 - Ravanno - Spondylolisthesis and SpondylosisDocument25 pagesISMT12 - Day 244 - Ravanno - Spondylolisthesis and SpondylosisRavanno Fanizza HarahapNo ratings yet
- OrthoticsDocument37 pagesOrthoticsergosadia658No ratings yet
- Surgery 1 - 1st ray-MTPJ (1-25-08)Document3 pagesSurgery 1 - 1st ray-MTPJ (1-25-08)Eddie MillsNo ratings yet
- Hallux Valgus SXDocument569 pagesHallux Valgus SXandi100% (2)
- Cubitus Varus, Elbow Joint, Mitali JoshiDocument13 pagesCubitus Varus, Elbow Joint, Mitali JoshiKapil Lakhwara100% (1)
- Different Injuries of The Musculoskeletal System Its Management and CareDocument113 pagesDifferent Injuries of The Musculoskeletal System Its Management and CareMaAn Castor Palcon TuzonNo ratings yet
- 01 Body Conformation of HorseDocument32 pages01 Body Conformation of HorseDrSagar Mahesh Sonwane100% (3)
- Case StudyDocument11 pagesCase StudyAnj TadxNo ratings yet
- Hip ExaminationDocument43 pagesHip ExaminationJayakrishnu tjNo ratings yet
- ClubfootDocument30 pagesClubfootdrusmanjamilhcmdNo ratings yet
- Position Sizing Calculator For StocksDocument2 pagesPosition Sizing Calculator For StocksMuhamad Izwan Bin HanafiNo ratings yet
- 5 Strand Vs 6 StrandDocument7 pages5 Strand Vs 6 StrandMuhamad Izwan Bin HanafiNo ratings yet
- STMKB Ar2020 FinalDocument328 pagesSTMKB Ar2020 FinalMuhamad Izwan Bin HanafiNo ratings yet
- ACL BTB Using EndoBDocument16 pagesACL BTB Using EndoBMuhamad Izwan Bin HanafiNo ratings yet
- Employers Liability Takaful Proposal Form 11102023Document5 pagesEmployers Liability Takaful Proposal Form 11102023Muhamad Izwan Bin HanafiNo ratings yet
- A-Life MediFlex Brochure 14062023 ENG & BMDocument12 pagesA-Life MediFlex Brochure 14062023 ENG & BMMuhamad Izwan Bin HanafiNo ratings yet
- Pathology Last 10 YearsDocument20 pagesPathology Last 10 YearsVastya RishiNo ratings yet
- Landmark Tennison: Pembimbing: Dr. Mantra Nandini, DRG., Mars, SPBM OlehDocument12 pagesLandmark Tennison: Pembimbing: Dr. Mantra Nandini, DRG., Mars, SPBM Olehdrg Riki Indra KusumaNo ratings yet
- Tableau Antidiabetiques Guide Des Produits 2017 enDocument1 pageTableau Antidiabetiques Guide Des Produits 2017 enHayna RoseNo ratings yet
- MRC - Sudan - Company Profile 2022Document6 pagesMRC - Sudan - Company Profile 2022Mohamed Mohamed Abdelrhman FadlNo ratings yet
- The Antecedents of Civilization in The Indus ValleyDocument17 pagesThe Antecedents of Civilization in The Indus ValleyNeha AnandNo ratings yet
- B22546 Sports Physician Concussion Assessment Tool SCAT3Document5 pagesB22546 Sports Physician Concussion Assessment Tool SCAT3Beto Alonso RamírezNo ratings yet
- Drug Discovery and Development: Medicinal ChemistryDocument57 pagesDrug Discovery and Development: Medicinal ChemistryHazel Ruth Yara CastilloNo ratings yet
- Genewin Biotech: Company IntroductionDocument16 pagesGenewin Biotech: Company IntroductionSwapnil DeyNo ratings yet
- Your Guide To Optimizing Vitamin D Youthfully: Optimize Vit D LevelsDocument13 pagesYour Guide To Optimizing Vitamin D Youthfully: Optimize Vit D LevelsJordanNo ratings yet
- Invertebrate Biology: by Jane YaweDocument42 pagesInvertebrate Biology: by Jane YaweANYWAR SIMONNo ratings yet
- Neonatal and Infant CareDocument10 pagesNeonatal and Infant CareCarla JimenezNo ratings yet
- Practical 3: Blood Grouping Test ObjectiveDocument2 pagesPractical 3: Blood Grouping Test ObjectiveTHASVIN OFFICIAL NETWORKNo ratings yet
- Nucleus - Structure and FunctionDocument36 pagesNucleus - Structure and FunctionMUHAMMAD SHAYANNo ratings yet
- Protection Against Stress by Natural Triterpene Esters - AAK PDFDocument4 pagesProtection Against Stress by Natural Triterpene Esters - AAK PDFjaggampudi. rajasekharNo ratings yet
- OBGYN II Important QsDocument10 pagesOBGYN II Important QsDwivith ReddyNo ratings yet
- 91157-Genetic Variation-2015Document12 pages91157-Genetic Variation-2015api-323107386No ratings yet
- CH 12 Word ListDocument3 pagesCH 12 Word ListtigertiaNo ratings yet
- A U D: D C M A - P C: Lcohol SE Isorders Iagnosis and Linical Anagement of Lcohol Related Hysical OmplicationsDocument286 pagesA U D: D C M A - P C: Lcohol SE Isorders Iagnosis and Linical Anagement of Lcohol Related Hysical Omplicationsdia9diaNo ratings yet
- Megan Talbott ResumeDocument3 pagesMegan Talbott Resumeapi-291314145No ratings yet
- NCPDocument4 pagesNCPMark Benedict Ocampo VelardeNo ratings yet
- Blood Bank ManagementDocument12 pagesBlood Bank ManagementSayantan MandalNo ratings yet
- Chapter-2 RRLDocument98 pagesChapter-2 RRLLovlegin DiongNo ratings yet