You might also like
- Dysrhythmias: Cardiac Conduction System Rhythm Strip RecognitionDocument5 pagesDysrhythmias: Cardiac Conduction System Rhythm Strip Recognitiontantalizin marieNo ratings yet
- Dysrhythmias 1: Cardiac Conduc1on System Rhythm Strip Recogni1onDocument4 pagesDysrhythmias 1: Cardiac Conduc1on System Rhythm Strip Recogni1ontantalizin marieNo ratings yet
- (NS) Arrhythmia Tutorial Questions DONEDocument12 pages(NS) Arrhythmia Tutorial Questions DONEJoei “Jojo” GohNo ratings yet
- Cardiac Science "Arrhythmia"Document16 pagesCardiac Science "Arrhythmia"jimjose antonyNo ratings yet
- A A T P ECG: 1. ID / Calibration 5. IntervalsDocument1 pageA A T P ECG: 1. ID / Calibration 5. IntervalsVanessa BergollaNo ratings yet
- 5.11 Normal Ecg, Chamber Enlargements, Ischemia, Infarcts: TH THDocument6 pages5.11 Normal Ecg, Chamber Enlargements, Ischemia, Infarcts: TH THRomeo AragonNo ratings yet
- Day 3 - EKGDocument115 pagesDay 3 - EKGchristian murtaniNo ratings yet
- Ecg ReadingDocument6 pagesEcg ReadingMarianette CainongNo ratings yet
- Cardiac Study GuideDocument9 pagesCardiac Study GuideJane DiazNo ratings yet
- 2022 Ch-86115. 3 Nursing Management of Patients With DysrhythmiasDocument78 pages2022 Ch-86115. 3 Nursing Management of Patients With DysrhythmiasIzziddin YassineNo ratings yet
- Ecgs Full For Ad2 2023 Ek Am KGDocument29 pagesEcgs Full For Ad2 2023 Ek Am KGj7g2m8fjqvNo ratings yet
- ElectrocardiographyDocument8 pagesElectrocardiographyRohan PackiarajNo ratings yet
- ECG How To InterpretDocument10 pagesECG How To InterpretMohamad DanialNo ratings yet
- Cardio NotesDocument7 pagesCardio Notesapi-3744683100% (4)
- (NS) Arrhythmia Tutorial QuestionsDocument11 pages(NS) Arrhythmia Tutorial QuestionsJoei “Jojo” GohNo ratings yet
- 07.01 - 12 Lead ECG Interpretation 2019Document141 pages07.01 - 12 Lead ECG Interpretation 2019Lana LocoNo ratings yet
- ECG Interpretation: DR S J Bhosale DM, FPCC (Canada) Associate Professor Tata Memorial CentreDocument90 pagesECG Interpretation: DR S J Bhosale DM, FPCC (Canada) Associate Professor Tata Memorial Centrevaishali TayadeNo ratings yet
- Medicine Revision E6.5 (Medicalstudyzone - Com)Document209 pagesMedicine Revision E6.5 (Medicalstudyzone - Com)Diya B johnNo ratings yet
- Ecg Reading - Your Heart's Rhythm and Electrical Activity. Placement of 12 Load EcgDocument6 pagesEcg Reading - Your Heart's Rhythm and Electrical Activity. Placement of 12 Load EcgMarianette CainongNo ratings yet
- Basic EKG InterpretationDocument48 pagesBasic EKG InterpretationAimee Ann Pauco MacaraegNo ratings yet
- Paul Rushe - Data Interpretation EditDocument132 pagesPaul Rushe - Data Interpretation Editjulian kircherNo ratings yet
- ECG 5th Year TeachingDocument27 pagesECG 5th Year TeachingnamwaNo ratings yet
- Presentasi Ws Ekg SakinahDocument40 pagesPresentasi Ws Ekg SakinahsiskaNo ratings yet
- Shelf IM Video SlidesDocument69 pagesShelf IM Video SlidesRuth SanmooganNo ratings yet
- Electrocardiograma NormalDocument56 pagesElectrocardiograma NormalZory NuñezNo ratings yet
- Medsurg 3 Exam 1Document55 pagesMedsurg 3 Exam 1Melissa Blanco100% (1)
- ELECTROCARDIOGRAMA NORMAL - PPTMDocument56 pagesELECTROCARDIOGRAMA NORMAL - PPTMZory NuñezNo ratings yet
- 12 Lead EKG Interpretation PDFDocument251 pages12 Lead EKG Interpretation PDFRobert So JrNo ratings yet
- Ilovepdf MergedDocument17 pagesIlovepdf MergedAngel HannahNo ratings yet
- ECG Interpretation & Dysrhythmia Identification: by Naaim AliDocument47 pagesECG Interpretation & Dysrhythmia Identification: by Naaim AliMohamed ElkadyNo ratings yet
- Dasar Ekg Iwe - RSPP Seminar RSPPDocument89 pagesDasar Ekg Iwe - RSPP Seminar RSPPMabro CahyoNo ratings yet
- Cardiac Life Support Cme Latest Edited VersionDocument53 pagesCardiac Life Support Cme Latest Edited VersionSyed Shahrul Naz SyedNo ratings yet
- EKG Cheat Sheet - Henry Del RosarioDocument1 pageEKG Cheat Sheet - Henry Del RosarioanwarNo ratings yet
- Cardiac Life Support Cme Latest Edited VersionDocument53 pagesCardiac Life Support Cme Latest Edited VersionSyed Shahrul Naz SyedNo ratings yet
- Dasar Dasar Ekg PDFDocument52 pagesDasar Dasar Ekg PDFBobyNo ratings yet
- Mikosis Endemik-WPS OfficeDocument75 pagesMikosis Endemik-WPS OfficeKurniatiKhasanahQhafisaQurratul'ainNo ratings yet
- Basics of ECG Pre-Workshop: Dr. Nancy Selfridge Chair, Department of Clinical Medicine Semester 4 2019Document43 pagesBasics of ECG Pre-Workshop: Dr. Nancy Selfridge Chair, Department of Clinical Medicine Semester 4 2019Tom TsouNo ratings yet
- Hendra - EKGDocument34 pagesHendra - EKGRINANo ratings yet
- Normal Sinus RhythmDocument48 pagesNormal Sinus RhythmStella mNo ratings yet
- ECG Interpretations DR RPDocument109 pagesECG Interpretations DR RPArnis Putri RosyaniNo ratings yet
- Arrhythmias TEAM441Document18 pagesArrhythmias TEAM441Joseph Brima SambaNo ratings yet
- IV - Cardiovascular SystemDocument3 pagesIV - Cardiovascular SystemGael QuingNo ratings yet
- Nclex RN Review Notes 2018 Triple eDocument30 pagesNclex RN Review Notes 2018 Triple eEndla SriniNo ratings yet
- Electrocardiogram Lecture MikeDocument111 pagesElectrocardiogram Lecture MikeDesiree MejicaNo ratings yet
- ECG Normal - ErwanDocument49 pagesECG Normal - ErwanEvelyne NatalieNo ratings yet
- Modul EKGDocument101 pagesModul EKGAjeng Dwik01No ratings yet
- ECG - DocToonDocument2 pagesECG - DocToondoc.abdulrahman.aymanNo ratings yet
- Basics of ECGDocument32 pagesBasics of ECGNachiket Vijay PotdarNo ratings yet
- ECG and ArrhythmiaDocument44 pagesECG and ArrhythmiaSamdiSutantoNo ratings yet
- Interpretase Ekg Ali HaedarDocument20 pagesInterpretase Ekg Ali HaedarRiska SilviaNo ratings yet
- Basic EcgDocument63 pagesBasic EcgrahmaNo ratings yet
- Adult Health IV Week One ECGsDocument20 pagesAdult Health IV Week One ECGsLea BuenoNo ratings yet
- Basic Ecg Interpretation & Procedure: BY: Ahmad Hafiz Bin Alias Universuty Lecturer UniszaDocument26 pagesBasic Ecg Interpretation & Procedure: BY: Ahmad Hafiz Bin Alias Universuty Lecturer UniszaLogadarshini VeerasamyNo ratings yet
- Case Presentation On Supraventricular TachycardiaDocument64 pagesCase Presentation On Supraventricular TachycardiaHazel AsperaNo ratings yet
- Bio Monitoring 01Document41 pagesBio Monitoring 01jidongjcNo ratings yet
- Sunday Academic MeetDocument22 pagesSunday Academic MeetSrinivasan YashrajNo ratings yet
- Basic Dysrhythmia Recognition: by Cookie LittleDocument25 pagesBasic Dysrhythmia Recognition: by Cookie LittleKariSilaMarieNo ratings yet
- Gaje SinghDocument70 pagesGaje SinghgemergencycareNo ratings yet
- TBPI Information PDFDocument8 pagesTBPI Information PDFxtraqrkyNo ratings yet
- 2022 Non-Cardiac SurgeryDocument105 pages2022 Non-Cardiac Surgeryhosameldin ahmedNo ratings yet
- Coronary ArteriesDocument28 pagesCoronary ArteriesMihaela IonescuNo ratings yet
- CPR Manual 2016 New Officers Final 3 1 PDFDocument48 pagesCPR Manual 2016 New Officers Final 3 1 PDFRj Polvorosa100% (1)
- Digoxin Monitoring and Toxicity ManagementDocument11 pagesDigoxin Monitoring and Toxicity ManagementWinsome Chloe Rara-BuñoNo ratings yet
- (Transes) Human Histology - 13 Lymphoid SystemDocument17 pages(Transes) Human Histology - 13 Lymphoid SystemReina CastronuevoNo ratings yet
- NCLEX Based 1000 MCQs Part-2Document12 pagesNCLEX Based 1000 MCQs Part-2AkashNo ratings yet
- Cardiopulmonary 3 2010 With AnswersDocument14 pagesCardiopulmonary 3 2010 With AnswersWenzy Cruz100% (2)
- Heparin Protocol For DVT PEDocument3 pagesHeparin Protocol For DVT PEhorzhanNo ratings yet
- BCLS Practice MCQ StudentsDocument14 pagesBCLS Practice MCQ StudentsRaniNo ratings yet
- UW - Cardiovascular - Educational ObjectivesDocument52 pagesUW - Cardiovascular - Educational ObjectivesUsama BilalNo ratings yet
- AntihypertensiveDocument163 pagesAntihypertensiveOsama FrancisNo ratings yet
- Mics 1Document7 pagesMics 1Ramya ENo ratings yet
- PMLS 2 ReviewerDocument8 pagesPMLS 2 ReviewerNepoy Beltran Entendez100% (3)
- 2017 Hypertension Webinar PDFDocument81 pages2017 Hypertension Webinar PDFMira Mariana UlfahNo ratings yet
- Medical AbbreviationDocument3 pagesMedical AbbreviationWaode FitriNo ratings yet
- Coronary Artery Bypass Graft Surgery in Patients With Ischemic Heart FailureDocument31 pagesCoronary Artery Bypass Graft Surgery in Patients With Ischemic Heart Failuresree vidhyaNo ratings yet
- Heart BlockDocument26 pagesHeart BlockMihir Patel88% (8)
- Med Surg Cardiovascular Flashcards - QuizletDocument2 pagesMed Surg Cardiovascular Flashcards - QuizletErika BacarroNo ratings yet
- Aneurysmal Subarachnoid Hemorrhage Nursing Self-Paced Case StudyDocument100 pagesAneurysmal Subarachnoid Hemorrhage Nursing Self-Paced Case StudyAndi rahma AnugrahNo ratings yet
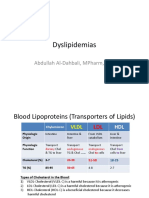
- Dyslipidemias: Abdullah Al-Dahbali, Mpharm, PHDDocument15 pagesDyslipidemias: Abdullah Al-Dahbali, Mpharm, PHDعزالدين الطيارNo ratings yet
- Mechanical Heart Valve vs. Bioprosthetic ValveDocument55 pagesMechanical Heart Valve vs. Bioprosthetic ValvePUSHPITHA PERERANo ratings yet
- 491.prevention of Heart Attacks & Cardiovascular DiseasesDocument80 pages491.prevention of Heart Attacks & Cardiovascular DiseasesAlberto Mora PereaNo ratings yet
- Perbedaan Kadar Kolesterol Sebelum Dan Sesudah Dilakukan Brisk Walking Pada SiswaDocument8 pagesPerbedaan Kadar Kolesterol Sebelum Dan Sesudah Dilakukan Brisk Walking Pada SiswaEva RahmadaniNo ratings yet
- Tetralogy of FallotDocument37 pagesTetralogy of Fallottintinlovessu100% (1)
- 11 Nursing Care Pacemaker Emil 2019Document5 pages11 Nursing Care Pacemaker Emil 2019ameliajamirusNo ratings yet
- Difference Between Dry and Wet GangreneDocument6 pagesDifference Between Dry and Wet GangreneNitamoni Deka0% (1)
- Congestive Heart FailureDocument25 pagesCongestive Heart Failureemman122392No ratings yet
- Stroke and Cerebrovascular DiseaseDocument14 pagesStroke and Cerebrovascular DiseaseMarwan M.No ratings yet
- Satuan Acara Penyuluhan Diabetes Melitus: Mata Kuliah: Keperawatan Komunitas IIDocument10 pagesSatuan Acara Penyuluhan Diabetes Melitus: Mata Kuliah: Keperawatan Komunitas IIJusmanNo ratings yet