You might also like
- US - ASA Physical Status Classification Chart - V2Document1 pageUS - ASA Physical Status Classification Chart - V2Roberto PvetNo ratings yet
- LosartanDocument2 pagesLosartanVina Jane P Laurel89% (9)
- Goljan Errata SheetDocument11 pagesGoljan Errata SheetVishala MishraNo ratings yet
- Quizlet Compilation (Part 1) : Philippine Nurse Licensure ExaminationDocument49 pagesQuizlet Compilation (Part 1) : Philippine Nurse Licensure Examinationhhello100% (1)
- NCP Knowledge DeficitDocument2 pagesNCP Knowledge DeficitRainier IbarretaNo ratings yet
- CASP Case Control Study Checklist DownloadDocument6 pagesCASP Case Control Study Checklist DownloadbintangNo ratings yet
- Hypertension Questionnaire-Applicant: Policy NumberDocument2 pagesHypertension Questionnaire-Applicant: Policy NumberMariane Tabor VelezNo ratings yet
- Nutrition Lec 10 Diet Surgical Conditions Burns PDFDocument2 pagesNutrition Lec 10 Diet Surgical Conditions Burns PDFbaekho's laughNo ratings yet
- Lapsus Rehab Low Back Pain-1Document10 pagesLapsus Rehab Low Back Pain-1rendyjiwonoNo ratings yet
- Rebamipide, A Gastro-Protective and Anti-Inflammatory Drug, Promotes Gastric Ulcer Healing Following Eradication TherapyDocument4 pagesRebamipide, A Gastro-Protective and Anti-Inflammatory Drug, Promotes Gastric Ulcer Healing Following Eradication TherapySilvester HenryNo ratings yet
- Venous Thrombosis: Complications of Deep Vein Thrombosis. Saint Luke's Health System. (N.D.) - Retrieved OctoberDocument1 pageVenous Thrombosis: Complications of Deep Vein Thrombosis. Saint Luke's Health System. (N.D.) - Retrieved OctoberSureen RegularNo ratings yet
- Diabetes Mellitus: Rasmussen NPR Concept PlanDocument1 pageDiabetes Mellitus: Rasmussen NPR Concept PlanRoshin TejeroNo ratings yet
- JBI Critical Appraisal-Checklist For Quasi - Experimental StudiesDocument6 pagesJBI Critical Appraisal-Checklist For Quasi - Experimental StudiesHendra Kurnia RakhmaNo ratings yet
- Physical Examination CopdDocument3 pagesPhysical Examination CopdOM BAWNENo ratings yet
- Episiotomy PDFDocument54 pagesEpisiotomy PDFputri diana100% (1)
- CASP Case Control Study Checklist 2018 Fillable Form Ceklis FixDocument6 pagesCASP Case Control Study Checklist 2018 Fillable Form Ceklis FixAndi MardiansyahNo ratings yet
- Nursing Assessment IIDocument5 pagesNursing Assessment IImyer pasandalanNo ratings yet
- How Can You Help Your Patients With An Uncomplicated UTI?: Know?Document1 pageHow Can You Help Your Patients With An Uncomplicated UTI?: Know?gegeNo ratings yet
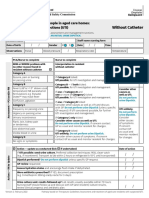
- Form Ams Clinical Pathway Fillable Form Without CatheterDocument1 pageForm Ams Clinical Pathway Fillable Form Without CatheterTeenu JobyNo ratings yet
- Nursing Care 2Document1 pageNursing Care 2Moh. H.AlObaidyNo ratings yet
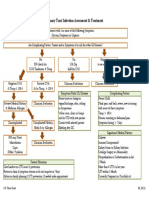
- Treating Your Infection UtiDocument1 pageTreating Your Infection UtiJames 'jps' SimanjuntakNo ratings yet
- CDU Care Plan. UTIDocument7 pagesCDU Care Plan. UTImutiso mutieNo ratings yet
- PearlsDocument2 pagesPearlspatriciaatan1497No ratings yet
- Surgery PearlsDocument2 pagesSurgery Pearlspatriciaatan1497No ratings yet
- Decision Aid For Diagnosis and Management of Suspected Urinary Tract Infection (UTI) in Older PeopleDocument4 pagesDecision Aid For Diagnosis and Management of Suspected Urinary Tract Infection (UTI) in Older PeopleNeisa SukmaNo ratings yet
- Abortion BSN 0PR-2: Case Study of BelleDocument27 pagesAbortion BSN 0PR-2: Case Study of BellekervinNo ratings yet
- PPI DeprescribingDocument1 pagePPI Deprescribinghairos.izhaNo ratings yet
- (GYNE) Dysmenorrhea and Breast Diseases-Dr. Lim (Pingu)Document13 pages(GYNE) Dysmenorrhea and Breast Diseases-Dr. Lim (Pingu)adrian kristopher dela cruzNo ratings yet
- Acute Appendicitis Clinical Case by SlidesgoDocument14 pagesAcute Appendicitis Clinical Case by SlidesgoalisbelecastilloNo ratings yet
- Urological RefferalDocument12 pagesUrological Refferalmichelle octavianiNo ratings yet
- Syndromic Management of STIsDocument1 pageSyndromic Management of STIsJoyNo ratings yet
- Tamoxifen NolvadexDocument1 pageTamoxifen NolvadexAdrianne Bazo100% (1)
- September 5, 2022: Date / Time Cues Nursing Diagnosis Rationale EvaluationDocument2 pagesSeptember 5, 2022: Date / Time Cues Nursing Diagnosis Rationale EvaluationCynelle AguilonNo ratings yet
- Early Medical Abortion Procedure SummaryDocument1 pageEarly Medical Abortion Procedure SummaryNusratNo ratings yet
- Barrientos Case Presentation Urinary Tract InfectionDocument17 pagesBarrientos Case Presentation Urinary Tract InfectionCalingalan Hussin CaluangNo ratings yet
- UTI TreatmentDocument3 pagesUTI TreatmentMaria RezitadinaNo ratings yet
- UrolithiasisDocument9 pagesUrolithiasisJessa MaeNo ratings yet
- DS ParatramDocument1 pageDS ParatramLarr SumalpongNo ratings yet
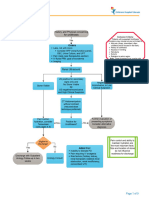
- UTI Treatment Algorithm - Sharp Mesa Vista 2Document3 pagesUTI Treatment Algorithm - Sharp Mesa Vista 2Fitri 1997No ratings yet
- Audit Tool IOLDocument6 pagesAudit Tool IOLRosa ValenteNo ratings yet
- Acute PancreatitisDocument11 pagesAcute PancreatitisJessa MaeNo ratings yet
- Ectopic Pregnancy CasiaDocument16 pagesEctopic Pregnancy CasiaMarie Ashley CasiaNo ratings yet
- Pancreatitis Pathway PDFDocument13 pagesPancreatitis Pathway PDFKhanif MuflikhatunNo ratings yet
- Holy Child School of Davao Nursing Care Plan: E. Jacinto St. Davao CityDocument2 pagesHoly Child School of Davao Nursing Care Plan: E. Jacinto St. Davao CityMaxileo Villareal AbeciaNo ratings yet
- NCP - Imbalanced Nutrition - de Guzman, Gadia, Lacanilao, VergaraDocument4 pagesNCP - Imbalanced Nutrition - de Guzman, Gadia, Lacanilao, VergaraLuis Gatchalian LacanilaoNo ratings yet
- Common Health Problems in AdolescentDocument12 pagesCommon Health Problems in AdolescentANNIE SHINE MAGSACAYNo ratings yet
- Uterine InversionDocument4 pagesUterine Inversionkarl de guzmanNo ratings yet
- Nursing Process Care Plan: Assessment Analysis Planning Implementation EvaluationDocument2 pagesNursing Process Care Plan: Assessment Analysis Planning Implementation EvaluationJamaila DomingoNo ratings yet
- Drug Study: West Visayas State University La Paz, Iloilo CityDocument14 pagesDrug Study: West Visayas State University La Paz, Iloilo CityKhryss Paula BaldonadoNo ratings yet
- JGJBJBDocument1 pageJGJBJBJuwita syafutriNo ratings yet
- Funda Sample ScenarioDocument2 pagesFunda Sample ScenarioGadez JeanpelNo ratings yet
- Does My Patient Need To Be Screened or Treated For A Urinary Tract InfectionDocument4 pagesDoes My Patient Need To Be Screened or Treated For A Urinary Tract Infectiontsiko111No ratings yet
- Assessment and Management Women in PregnantDocument1 pageAssessment and Management Women in Pregnantanisah tri agustiniNo ratings yet
- Nursing Care Management For Patient With Renal ProblemsDocument32 pagesNursing Care Management For Patient With Renal ProblemsMaria Victoria A. PraxidesNo ratings yet
- Common Causes of Low Abdominal (Pelvic) Pain in Women of Reproductive AgeDocument3 pagesCommon Causes of Low Abdominal (Pelvic) Pain in Women of Reproductive AgeZerry Reza SyahrulNo ratings yet
- Recommendations For Oral Surgery During COVID-19 Pandemic: WWW - Rcseng.ac - Uk/dental-Faculties/fds/coronavirusDocument7 pagesRecommendations For Oral Surgery During COVID-19 Pandemic: WWW - Rcseng.ac - Uk/dental-Faculties/fds/coronavirusFaiqotul KumalaNo ratings yet
- bpj20 Stis Pages 24-29Document6 pagesbpj20 Stis Pages 24-29tecnoaaaa2No ratings yet
- Hemophilia and Von Willebrand Disease EmergenciesDocument13 pagesHemophilia and Von Willebrand Disease EmergenciesDobrila SimonovicNo ratings yet
- Grandrounds Protocol ServandoDocument4 pagesGrandrounds Protocol ServandoAllison Eunice ServandoNo ratings yet
- Cburbachcareplan 2Document8 pagesCburbachcareplan 2api-520843051No ratings yet
- Marquez 12d NCP Mod 3Document2 pagesMarquez 12d NCP Mod 3Macy MarquezNo ratings yet
- Blue and White Illustrated Medical Healthcare in The 21st Century Education PresentationDocument32 pagesBlue and White Illustrated Medical Healthcare in The 21st Century Education PresentationMaria Victoria A. PraxidesNo ratings yet
- PomtoplistDocument14 pagesPomtoplistOladimeji Raphael OnibonNo ratings yet
- Medications and Falls in The ElderlyDocument2 pagesMedications and Falls in The ElderlyOladimeji Raphael OnibonNo ratings yet
- BiochemistryDocument1 pageBiochemistryOladimeji Raphael OnibonNo ratings yet
- Moneyinclusive PatternDocument3 pagesMoneyinclusive PatternOladimeji Raphael OnibonNo ratings yet
- Bola CommunityDocument5 pagesBola CommunityOladimeji Raphael OnibonNo ratings yet
- Great Is Thy FaithDocument1 pageGreat Is Thy FaithOladimeji Raphael OnibonNo ratings yet
- Green Light Pre-Reg Study Day Programme Booking Form 2015-16-9Document2 pagesGreen Light Pre-Reg Study Day Programme Booking Form 2015-16-9Oladimeji Raphael OnibonNo ratings yet
- Pas RPSGB Fs Controlled Drugs Community Pharmacy Feb08Document54 pagesPas RPSGB Fs Controlled Drugs Community Pharmacy Feb08sweetmacyNo ratings yet
- Pas RPSGB Fs Controlled Drugs Community Pharmacy Feb08Document54 pagesPas RPSGB Fs Controlled Drugs Community Pharmacy Feb08sweetmacyNo ratings yet
- Therapeutic Handbook 2012 PDFDocument376 pagesTherapeutic Handbook 2012 PDFOladimeji Raphael OnibonNo ratings yet
- Therapeutic Handbook 2012 PDFDocument376 pagesTherapeutic Handbook 2012 PDFOladimeji Raphael OnibonNo ratings yet
- MO Community Pharmacy BriefingDocument4 pagesMO Community Pharmacy BriefingOladimeji Raphael OnibonNo ratings yet
- Severe Disability, MRS 2) : Scottish Intercollegiate Guidelines NetworkDocument2 pagesSevere Disability, MRS 2) : Scottish Intercollegiate Guidelines NetworkOladimeji Raphael OnibonNo ratings yet
- Numeracy Sample Paper 1Document6 pagesNumeracy Sample Paper 1Oladimeji Raphael OnibonNo ratings yet
- Pharmacy CalculationsDocument39 pagesPharmacy CalculationsOladimeji Raphael OnibonNo ratings yet
- Graha Roga'sDocument10 pagesGraha Roga'srohinibrajole123No ratings yet
- Fnac of Thyroid - 102717Document13 pagesFnac of Thyroid - 102717Lal RuattlingaNo ratings yet
- Intestinal ObstructionDocument59 pagesIntestinal ObstructionGeorge GuruNo ratings yet
- G.R. No. L-56259 March 18, 1983 Sylvia F. Panangui and Olivia F. Panangui, Minors, Represented by Albertha FerrerDocument25 pagesG.R. No. L-56259 March 18, 1983 Sylvia F. Panangui and Olivia F. Panangui, Minors, Represented by Albertha Ferrerpoint clickNo ratings yet
- 1 s2.0 S014067362300020X MainDocument14 pages1 s2.0 S014067362300020X MainGERIATRIA 72No ratings yet
- Hypocalcaemia ESSAYDocument2 pagesHypocalcaemia ESSAYPris AtarashiiNo ratings yet
- 5th Year Passmedicine Notes 3Document20 pages5th Year Passmedicine Notes 3quojo041No ratings yet
- TB PosterDocument13 pagesTB Posterthamizhselvi87No ratings yet
- Why Does My Patient Limphadenopathy or Splenomegaly?Document14 pagesWhy Does My Patient Limphadenopathy or Splenomegaly?lacmftcNo ratings yet
- Psychotherapy DAP NoteDocument2 pagesPsychotherapy DAP NoteMistor Williams100% (1)
- Stago Vol 5 Issue 2 2015Document10 pagesStago Vol 5 Issue 2 2015PABLO ZAMUDIONo ratings yet
- Errata of QbankDocument29 pagesErrata of QbankSaba WaheedNo ratings yet
- Zollinger-Ellison SyndromeDocument9 pagesZollinger-Ellison SyndromeGLYDEL CORDERONo ratings yet
- Urnal Vox Sanguinis - 2023 - Pons - Prevalence of Red Blood Cell Alloantibodies Among Blood Donors in The French Military BloodDocument5 pagesUrnal Vox Sanguinis - 2023 - Pons - Prevalence of Red Blood Cell Alloantibodies Among Blood Donors in The French Military BloodFauzan.ANo ratings yet
- Amniotic Fluid and Placenta AbnormalitiesDocument60 pagesAmniotic Fluid and Placenta AbnormalitiesMicah Lou CalambaNo ratings yet
- Untitled Document 22Document5 pagesUntitled Document 22api-609568172No ratings yet
- Patient's Profile I. Biographic DataDocument2 pagesPatient's Profile I. Biographic DataLongyapon Sheena StephanieNo ratings yet
- Clinical Practicum Worksheet: Nursing Care PlanDocument4 pagesClinical Practicum Worksheet: Nursing Care PlanOrlea Francisco-SisioNo ratings yet
- CCL 029 029a Child Medical Record Immunization History Health AssessmentDocument3 pagesCCL 029 029a Child Medical Record Immunization History Health Assessmentapi-311935573No ratings yet
- Inherited Metabolic Disorders Are Genetic Conditions That Result in Metabolism ProblemsDocument10 pagesInherited Metabolic Disorders Are Genetic Conditions That Result in Metabolism ProblemsLance CornistaNo ratings yet
- Problem Nursing Diagnosis Background Knowledge Goal and Objective Nursing Intervention Rationale EvaluationDocument2 pagesProblem Nursing Diagnosis Background Knowledge Goal and Objective Nursing Intervention Rationale Evaluationcherrymae mataNo ratings yet
- Association Between Liver Cirrhosis and Diabetes Mellitus: A Review On Hepatic OutcomesDocument15 pagesAssociation Between Liver Cirrhosis and Diabetes Mellitus: A Review On Hepatic Outcomesdoremi miredoNo ratings yet
- Spinal Cord InjuryDocument52 pagesSpinal Cord Injurynur muizzah afifah hussinNo ratings yet
- Biostat 2020 62 QDocument270 pagesBiostat 2020 62 Q'محمد علي' محمد لافيNo ratings yet
- Food HygieneDocument31 pagesFood Hygienehemihema100% (1)
- Test Yourself: MCQ and Extended MatchingDocument2 pagesTest Yourself: MCQ and Extended MatchingPhil ChanNo ratings yet
- Appendix DuplicationDocument3 pagesAppendix DuplicationMario TrejoNo ratings yet
- ConcorDocument40 pagesConcorviczNo ratings yet