You might also like
- 2012 Von Willebrand Disease Pocket GuideDocument4 pages2012 Von Willebrand Disease Pocket GuideAnonymous T1fOfQfqRBNo ratings yet
- Physician or Clinic Coordinating NOAC Treatment Important Patient Instructions What To Do in Certain Occasions Information For Healthcare ProvidersDocument2 pagesPhysician or Clinic Coordinating NOAC Treatment Important Patient Instructions What To Do in Certain Occasions Information For Healthcare ProvidersgabrimarteNo ratings yet
- Case Scenario.... : Caesarian SectionDocument5 pagesCase Scenario.... : Caesarian SectionLyka Joy DavilaNo ratings yet
- PrevacidDocument1 pagePrevacidAdrianne BazoNo ratings yet
- Cburbachcareplan 2Document8 pagesCburbachcareplan 2api-520843051No ratings yet
- WNHS Og AntepartumHaemorrhageDocument17 pagesWNHS Og AntepartumHaemorrhagelydia amaliaNo ratings yet
- PREOPinguinalherniaDocument2 pagesPREOPinguinalherniapatriciaatan1497No ratings yet
- GO Case-StudyDocument3 pagesGO Case-StudybabyboyNo ratings yet
- Tamoxifen NolvadexDocument1 pageTamoxifen NolvadexAdrianne Bazo100% (1)
- Drug StudyDocument2 pagesDrug StudyTrexie ScattNo ratings yet
- Pre Op Guidelines PDFDocument60 pagesPre Op Guidelines PDFAhmed NahrawyNo ratings yet
- Algorithm - June 2019 Pathway IntususepsiDocument1 pageAlgorithm - June 2019 Pathway IntususepsiIndah KumalaNo ratings yet
- Drug Study HemoDocument5 pagesDrug Study HemobarugacristianNo ratings yet
- PearlsDocument2 pagesPearlspatriciaatan1497No ratings yet
- Antepartum HaemorrhageDocument19 pagesAntepartum HaemorrhageKvy OngNo ratings yet
- PRN00936 II Pharmacy First Clinical Pathways v.1.6Document7 pagesPRN00936 II Pharmacy First Clinical Pathways v.1.6Oladimeji Raphael OnibonNo ratings yet
- Acute Appendicitis Clinical Case by SlidesgoDocument14 pagesAcute Appendicitis Clinical Case by SlidesgoalisbelecastilloNo ratings yet
- LovenoxDocument1 pageLovenoxAdrianne BazoNo ratings yet
- Cholecystectomy - James Conrad SalengaDocument14 pagesCholecystectomy - James Conrad SalengaJames Conrad SalengaNo ratings yet
- Aafp Dizziness CPGDocument9 pagesAafp Dizziness CPGIrene ChanNo ratings yet
- AFP Abnormal MensesDocument12 pagesAFP Abnormal Mensespatrick_raj884545No ratings yet
- Interference and ImmunoassaysDocument42 pagesInterference and ImmunoassaysGawri AbeyNo ratings yet
- LovenoxDocument1 pageLovenoxKatie McPeek100% (2)
- Recommendations For Oral Surgery During COVID-19 Pandemic: WWW - Rcseng.ac - Uk/dental-Faculties/fds/coronavirusDocument7 pagesRecommendations For Oral Surgery During COVID-19 Pandemic: WWW - Rcseng.ac - Uk/dental-Faculties/fds/coronavirusFaiqotul KumalaNo ratings yet
- Tranexamic Acid Drug StudyDocument1 pageTranexamic Acid Drug StudyEsmareldah Henry Sirue100% (1)
- LocalDocument5 pagesLocalybqbjpvtmrNo ratings yet
- Drug StudyDocument19 pagesDrug StudyKimberly Subade MandilagNo ratings yet
- Incision and Drainage of Abscess: Manalac, Eunice Jade A. BSN 3-ADocument11 pagesIncision and Drainage of Abscess: Manalac, Eunice Jade A. BSN 3-AEunice MañalacNo ratings yet
- DKA Case of The WeekDocument3 pagesDKA Case of The WeeklqpnoteNo ratings yet
- Hemolytic AnemiaDocument46 pagesHemolytic AnemiaSjerwin Anthony Gianan100% (1)
- Placenta Previa Case Study: Adefuin, Jay Rovillos, Noemie MDocument40 pagesPlacenta Previa Case Study: Adefuin, Jay Rovillos, Noemie MMikes CastroNo ratings yet
- Urinary Tract Infection and Pyelonephritis AIIMS Kalyani 7th SemesterDocument39 pagesUrinary Tract Infection and Pyelonephritis AIIMS Kalyani 7th Semesterrakesh raushanNo ratings yet
- Checked DS-ClopidogrelDocument2 pagesChecked DS-ClopidogrelBev ManaloNo ratings yet
- Urological RefferalDocument12 pagesUrological Refferalmichelle octavianiNo ratings yet
- JFP 1992-05 v34 I5 Complications-Occurring-From-DiagnosticDocument3 pagesJFP 1992-05 v34 I5 Complications-Occurring-From-DiagnosticwenyNo ratings yet
- Drug LovenoxDocument2 pagesDrug LovenoxSrkocherNo ratings yet
- Ceftriaxone SodiumDocument2 pagesCeftriaxone SodiumSTORAGE FILENo ratings yet
- Lovenox (Enoxaparin) 80mgDocument1 pageLovenox (Enoxaparin) 80mgAdrianne BazoNo ratings yet
- PearlsDocument2 pagesPearlspatriciaatan1497No ratings yet
- Nle Tips MS PDFDocument11 pagesNle Tips MS PDFjthsNo ratings yet
- Nursing Care 2Document1 pageNursing Care 2Moh. H.AlObaidyNo ratings yet
- Ectopic Pregnancy Villapando Ivan Concept MapDocument8 pagesEctopic Pregnancy Villapando Ivan Concept MapIvan VillapandoNo ratings yet
- Oxytocin Drug StudyDocument2 pagesOxytocin Drug StudyRem remNo ratings yet
- Assessment and Management Women in PregnantDocument1 pageAssessment and Management Women in Pregnantanisah tri agustiniNo ratings yet
- Waiters PATIENT CARE PLAN 2020 For PPHDocument3 pagesWaiters PATIENT CARE PLAN 2020 For PPHmp1757No ratings yet
- Anal Fissure - ColoproctoDocument3 pagesAnal Fissure - ColoproctoThomas KlebNo ratings yet
- Vets Now Surgical Safety ChecklistDocument1 pageVets Now Surgical Safety ChecklistVeterinarios de ArgentinaNo ratings yet
- Surgery PearlsDocument2 pagesSurgery Pearlspatriciaatan1497No ratings yet
- Hemophilia and Hemostasis: A Case-Based Approach to ManagementFrom EverandHemophilia and Hemostasis: A Case-Based Approach to ManagementAlice D. MaNo ratings yet
- Nursing Care Plan and Drug Study: University of Cebu - Banilad Campus Banilad, Cebu City College of NursingDocument16 pagesNursing Care Plan and Drug Study: University of Cebu - Banilad Campus Banilad, Cebu City College of NursingVinz OñoNo ratings yet
- Febrile Seizures PathwayDocument10 pagesFebrile Seizures PathwayFerry Abu Irsyad AtthaillahNo ratings yet
- Adrenal Hemorrhage A 25-Year Experience at The Mayo Clinic PDFDocument8 pagesAdrenal Hemorrhage A 25-Year Experience at The Mayo Clinic PDFImanuel Far-FarNo ratings yet
- Surgery PearlsDocument2 pagesSurgery Pearlspatriciaatan1497No ratings yet
- Tranexamic Acid Drug StudyDocument1 pageTranexamic Acid Drug StudyCen Janber Cabrillos67% (3)
- Textbook of Urgent Care Management: Chapter 39, Ensuring Patient SafetyFrom EverandTextbook of Urgent Care Management: Chapter 39, Ensuring Patient SafetyNo ratings yet
- USMLE Step 3 Lecture Notes 2021-2022: Pediatrics, Obstetrics/Gynecology, Surgery, Epidemiology/Biostatistics, Patient SafetyFrom EverandUSMLE Step 3 Lecture Notes 2021-2022: Pediatrics, Obstetrics/Gynecology, Surgery, Epidemiology/Biostatistics, Patient SafetyRating: 5 out of 5 stars5/5 (2)
- Comparison of The New Viscoelastic Coagulation AnaDocument9 pagesComparison of The New Viscoelastic Coagulation AnaDobrila SimonovicNo ratings yet
- Blood Management in Post-Partum Haemorrhage, Including Point of Care Coagulation TestsDocument7 pagesBlood Management in Post-Partum Haemorrhage, Including Point of Care Coagulation TestsDobrila SimonovicNo ratings yet
- BASIC PHYSIOLOGY For ANESTHETISTSDocument468 pagesBASIC PHYSIOLOGY For ANESTHETISTSAris ResurreccionNo ratings yet
- Grlinger ROTEM PPH DSMH Colombo 22-01-2019 ShortDocument86 pagesGrlinger ROTEM PPH DSMH Colombo 22-01-2019 ShortDobrila SimonovicNo ratings yet
- Topical Application of Tranexamic Acid - GREEN VoRDocument73 pagesTopical Application of Tranexamic Acid - GREEN VoRDobrila SimonovicNo ratings yet
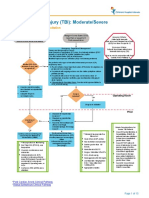
- Traumatic Brain Injury Moderate Severe Clinical PathwayDocument15 pagesTraumatic Brain Injury Moderate Severe Clinical PathwayDobrila SimonovicNo ratings yet
- PROGRAM 10th Annual Spring Scientific Symposium in Anaesthesiology and IntesniveCareDocument14 pagesPROGRAM 10th Annual Spring Scientific Symposium in Anaesthesiology and IntesniveCareDobrila SimonovicNo ratings yet
- Drill Bit Classifier 2004 PDFDocument15 pagesDrill Bit Classifier 2004 PDFgustavoemir0% (2)
- STS Reviewer FinalsDocument33 pagesSTS Reviewer FinalsLeiNo ratings yet
- EHR StandardsIndia - August 2013-32630521Document54 pagesEHR StandardsIndia - August 2013-32630521kartiksinhNo ratings yet
- L&T Motor CatalogDocument24 pagesL&T Motor CatalogSanjeev DhariwalNo ratings yet
- COSO DefinEDDocument21 pagesCOSO DefinEDRefdy AnugrahNo ratings yet
- Glossary of Terms 2nd PartDocument2 pagesGlossary of Terms 2nd Part2DJoyce D.N CapacieteNo ratings yet
- CA-idms Ads Alive User Guide 15.0Document142 pagesCA-idms Ads Alive User Guide 15.0svdonthaNo ratings yet
- Management Glossary - Musa KamawiDocument50 pagesManagement Glossary - Musa KamawiKazi Nazrul IslamNo ratings yet
- Moinho Disco PKM PDFDocument6 pagesMoinho Disco PKM PDFPaulo WilkerNo ratings yet
- THE Ketofeed Diet Book v2Document43 pagesTHE Ketofeed Diet Book v2jacosta12100% (1)
- General Arrangement, Isometric Views and B.O.M. A Midget Steam Car Using A Double Acting Oscillating EngineDocument3 pagesGeneral Arrangement, Isometric Views and B.O.M. A Midget Steam Car Using A Double Acting Oscillating EngineRobson Carlos0% (1)
- The Incidence of COVID-19 Along The ThaiCambodian Border Using Geographic Information System (GIS), Sa Kaeo Province, Thailand PDFDocument5 pagesThe Incidence of COVID-19 Along The ThaiCambodian Border Using Geographic Information System (GIS), Sa Kaeo Province, Thailand PDFInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Fbla Scavenger Hunt 1Document3 pagesFbla Scavenger Hunt 1api-472648158No ratings yet
- Assignment Group OSHADocument10 pagesAssignment Group OSHAariffikriismailNo ratings yet
- Faculty Vitae 1. Name: C.TamilselviDocument2 pagesFaculty Vitae 1. Name: C.Tamilselvisadeeskumar.dNo ratings yet
- Perfect Picture SummaryDocument3 pagesPerfect Picture SummaryReiaNo ratings yet
- NCP81205Document1 pageNCP81205Tom TomNo ratings yet
- (IGC 2024) 2nd Circular - 0630Document43 pages(IGC 2024) 2nd Circular - 0630VictoriaNo ratings yet
- Police Cranston School Committee Member Stole PTO FundsDocument1 pagePolice Cranston School Committee Member Stole PTO FundsashaydelineNo ratings yet
- KirbyDocument3 pagesKirbyNorhassanah UtosabuayanNo ratings yet
- Micro Fibra Sintetica at 06-MapeiDocument2 pagesMicro Fibra Sintetica at 06-MapeiSergio GonzalezNo ratings yet
- Keira Knightley: Jump To Navigation Jump To SearchDocument12 pagesKeira Knightley: Jump To Navigation Jump To SearchCrina LupuNo ratings yet
- EPA NCP Technical Notebook PDFDocument191 pagesEPA NCP Technical Notebook PDFlavrikNo ratings yet
- Augmentation of Labour: Nabhan A, Boulvain MDocument8 pagesAugmentation of Labour: Nabhan A, Boulvain MMade SuryaNo ratings yet
- CS1 Entity Level Controls SolutionsDocument16 pagesCS1 Entity Level Controls SolutionsPakistan Breaking News100% (6)
- Syllabus - Building Rehabilitation Anfd Forensic en - 220825 - 181244Document3 pagesSyllabus - Building Rehabilitation Anfd Forensic en - 220825 - 181244M O H A N A V E LNo ratings yet
- Simple Love Spells That WorkDocument14 pagesSimple Love Spells That Workagg24ankitNo ratings yet
- Grammar Review A2-B1Document5 pagesGrammar Review A2-B1Lena Silva SouzaNo ratings yet
- VDRL - Press. GaugesDocument9 pagesVDRL - Press. GaugesSourav RayNo ratings yet
- DocumentationDocument44 pagesDocumentation19-512 Ratnala AshwiniNo ratings yet