You might also like
- Cardiac Rehabilitation: A Workbook for use with Group ProgrammesFrom EverandCardiac Rehabilitation: A Workbook for use with Group ProgrammesNo ratings yet
- Intraoperative Neurophysiological Monitoring in Hemifacial Spasm: A Practical GuideFrom EverandIntraoperative Neurophysiological Monitoring in Hemifacial Spasm: A Practical GuideNo ratings yet
- Truspected Stroke AlgorithmDocument4 pagesTruspected Stroke Algorithmtri wahyunoNo ratings yet
- Acute Coronary SyndromeDocument7 pagesAcute Coronary SyndromePuskesmas Pinang JayaNo ratings yet
- Suspected Stroke Algorithm: NINDS Time GoalsDocument1 pageSuspected Stroke Algorithm: NINDS Time Goalsjohndoe1995No ratings yet
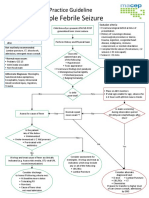
- Comparison of The Effects of Clobazam and Diazepam in Prevention of Recurrent Febrile SeizuresDocument2 pagesComparison of The Effects of Clobazam and Diazepam in Prevention of Recurrent Febrile SeizuresCharina Geofhany DeboraNo ratings yet
- STEMI Algorithm Poster 18x24Document1 pageSTEMI Algorithm Poster 18x24OgizWaraNo ratings yet
- Acute Coronary Syndrome - YMDocument64 pagesAcute Coronary Syndrome - YMNirwanaNo ratings yet
- QR Early Management of Head Injury in AdultsDocument8 pagesQR Early Management of Head Injury in Adultshoong.michelleNo ratings yet
- Stemi NSTEMI or Unstable Angina: Offer AspirinDocument1 pageStemi NSTEMI or Unstable Angina: Offer AspirinVemuri SrinivasNo ratings yet
- Acs With New Stemi GuidelineDocument35 pagesAcs With New Stemi Guidelinematmin07No ratings yet
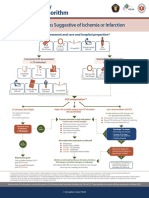
- Syndromes Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PreparationDocument1 pageSyndromes Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PreparationIGOR SHEYNINNo ratings yet
- Response Assessment in Neuro-Oncology (RANO)Document31 pagesResponse Assessment in Neuro-Oncology (RANO)Rini AndrianiNo ratings yet
- Randomized Trial of Atorvastatin For Reduction of Myocardial Damage During Coronary InterventionDocument5 pagesRandomized Trial of Atorvastatin For Reduction of Myocardial Damage During Coronary InterventionHarunNo ratings yet
- EP Club - Basic Holter MonitoringDocument29 pagesEP Club - Basic Holter Monitoringzakiyyatul aflakhaNo ratings yet
- Management of A Case of Ventricular Bigeminy UsingDocument2 pagesManagement of A Case of Ventricular Bigeminy UsingAlfian AlfianNo ratings yet
- ACS Management in Pandemic EraDocument56 pagesACS Management in Pandemic EraFatmawati nersNo ratings yet
- Rangkuman CCS 1Document16 pagesRangkuman CCS 1Tesis Maruli Tua SianiparNo ratings yet
- Stroke Guidelines: Cva Critical Pathway Department of NeurologyDocument5 pagesStroke Guidelines: Cva Critical Pathway Department of NeurologyplethoraldorkNo ratings yet
- How To Stratify The Risk and When To Refer: NsteacsDocument28 pagesHow To Stratify The Risk and When To Refer: NsteacsRatna TambaNo ratings yet
- Cardiology 2023 FinalDocument208 pagesCardiology 2023 FinalBelinda ELISHA100% (1)
- Algorithm 1: Initial Evaluation and Management: Symptoms of Possible ACSDocument6 pagesAlgorithm 1: Initial Evaluation and Management: Symptoms of Possible ACSNenyNo ratings yet
- Dr. WismajiDocument41 pagesDr. WismajislametNo ratings yet
- UNC ED Code Stroke Pathway 9 2016 FINALDocument2 pagesUNC ED Code Stroke Pathway 9 2016 FINALJackNo ratings yet
- Kegawatan Jantung - MeDocument41 pagesKegawatan Jantung - MeNam Min BinNo ratings yet
- Garrett Terhune SBP Ich Grand RoundsDocument31 pagesGarrett Terhune SBP Ich Grand Roundsapi-648757084No ratings yet
- 12-Adult Post Resuscitation Care Algorithm 2021Document1 page12-Adult Post Resuscitation Care Algorithm 2021khaledNo ratings yet
- OrthopeadicsDocument30 pagesOrthopeadicsharshaNo ratings yet
- ACS Algorithm 2016 PDFDocument1 pageACS Algorithm 2016 PDFrabin1994No ratings yet
- TrialsDocument12 pagesTrialsRaaj SharmaNo ratings yet
- Algorithm of Resuscitation CareDocument1 pageAlgorithm of Resuscitation CarejyothiNo ratings yet
- Management of Status Epilepticus 2022Document8 pagesManagement of Status Epilepticus 2022albert siraitNo ratings yet
- Kahpf IhdDocument2 pagesKahpf IhdAnastasia ApriliaNo ratings yet
- AAN2023 PedsNCC Case1 Compositeslides 4.13Document14 pagesAAN2023 PedsNCC Case1 Compositeslides 4.13Evelina ȘabanovNo ratings yet
- Acs CCS 2021 KLDocument52 pagesAcs CCS 2021 KLPitchya WangmeesriNo ratings yet
- 2020 Acls Megacode Testing Scenarios - 2Document13 pages2020 Acls Megacode Testing Scenarios - 2Dr. Saqib RazaNo ratings yet
- Acute Coronary Syndrome Workup Approach Considerations, Electrocardiography, Measurement of CK-MB LevelsDocument1 pageAcute Coronary Syndrome Workup Approach Considerations, Electrocardiography, Measurement of CK-MB LevelsfeaghNo ratings yet
- Syndroms Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PrepartionDocument8 pagesSyndroms Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PrepartionNugroho TeguhNo ratings yet
- Syndroms Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PrepartionDocument1 pageSyndroms Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PrepartionAnonymous CKAborxxwNo ratings yet
- Exercise TestingDocument13 pagesExercise TestingjainilNo ratings yet
- Slide Deck ACS Referral Forum - DR Adhitia MIni Simposium ACSDocument20 pagesSlide Deck ACS Referral Forum - DR Adhitia MIni Simposium ACSsyahrial fazaNo ratings yet
- Neurology Musculoskeletal (MedicalBooksVN - Com)Document4 pagesNeurology Musculoskeletal (MedicalBooksVN - Com)Jonathan AiresNo ratings yet
- ICSI Stroke June2019 v2Document55 pagesICSI Stroke June2019 v2PerwiraNo ratings yet
- Acut Coronary SyndromesDocument1 pageAcut Coronary SyndromesMuhittin Selçuk ÖzkanNo ratings yet
- Algo Acs PDFDocument1 pageAlgo Acs PDFNety Pandung SalembanNo ratings yet
- Algo Acs PDFDocument1 pageAlgo Acs PDFJim Christian EllaserNo ratings yet
- Posters For ClinicDocument80 pagesPosters For ClinicdenzkissaieNo ratings yet
- Adult Post-Cardiac Arrest Care Algorithm: o Co Io o CoDocument1 pageAdult Post-Cardiac Arrest Care Algorithm: o Co Io o CoKavya ShreeNo ratings yet
- BDMS Trauma Algorithm Version 2.0Document32 pagesBDMS Trauma Algorithm Version 2.0Aungkhena Noomnim100% (2)
- ACLS ACS Algorithm NewDocument3 pagesACLS ACS Algorithm Newsambo100% (1)
- Captura de Pantalla 2021-09-28 A La(s) 6.46.21 P. M.Document1 pageCaptura de Pantalla 2021-09-28 A La(s) 6.46.21 P. M.VALENTINA LOPEZ MARINNo ratings yet
- Cyclobenzaprine Hydrochloride Drug StudyDocument4 pagesCyclobenzaprine Hydrochloride Drug StudyJay Ann Joy PerudaNo ratings yet
- ACLS Megacode Testing ScenariosDocument12 pagesACLS Megacode Testing Scenariosealm10100% (2)
- Rehab Tech 1Document11 pagesRehab Tech 1Vipul JainNo ratings yet
- Modalities of Cardiac Stress Test: Tiffany T. Nguyen MD April 2014Document14 pagesModalities of Cardiac Stress Test: Tiffany T. Nguyen MD April 2014Vimal NishadNo ratings yet
- ACLS Healthcare Provider Post-Cardiac Arrest Care Algorithm: o Co Io o CoDocument1 pageACLS Healthcare Provider Post-Cardiac Arrest Care Algorithm: o Co Io o CoAlexis HospitalNo ratings yet
- AlgorithmACLS PCAC 200622Document1 pageAlgorithmACLS PCAC 200622Sandy XNo ratings yet
- Geriatric Anesthesia: A Practical GuideFrom EverandGeriatric Anesthesia: A Practical GuideBharathi GourkantiNo ratings yet
- Blood Management in Post-Partum Haemorrhage, Including Point of Care Coagulation TestsDocument7 pagesBlood Management in Post-Partum Haemorrhage, Including Point of Care Coagulation TestsDobrila SimonovicNo ratings yet
- Hemophilia and Von Willebrand Disease EmergenciesDocument13 pagesHemophilia and Von Willebrand Disease EmergenciesDobrila SimonovicNo ratings yet
- Grlinger ROTEM PPH DSMH Colombo 22-01-2019 ShortDocument86 pagesGrlinger ROTEM PPH DSMH Colombo 22-01-2019 ShortDobrila SimonovicNo ratings yet
- Topical Application of Tranexamic Acid - GREEN VoRDocument73 pagesTopical Application of Tranexamic Acid - GREEN VoRDobrila SimonovicNo ratings yet
- PROGRAM 10th Annual Spring Scientific Symposium in Anaesthesiology and IntesniveCareDocument14 pagesPROGRAM 10th Annual Spring Scientific Symposium in Anaesthesiology and IntesniveCareDobrila SimonovicNo ratings yet
- Saint-Go Bain: Safety Data SheetDocument7 pagesSaint-Go Bain: Safety Data SheeteadriesNo ratings yet
- Tapan Majhi 10.12.21Document6 pagesTapan Majhi 10.12.21Suman MajhiNo ratings yet
- Whatis Art TherapyDocument14 pagesWhatis Art TherapyNoha IbrahimNo ratings yet
- Preterm BirthDocument198 pagesPreterm BirthHoopmen tampubolonNo ratings yet
- Lopez Fernandez 2021 Emerging Health and Education IssueDocument19 pagesLopez Fernandez 2021 Emerging Health and Education IssueAna Paula GomesNo ratings yet
- Report IndexedDocument302 pagesReport Indexeditab45No ratings yet
- Danger Signs in NewbornDocument22 pagesDanger Signs in NewbornAbhirup BoseNo ratings yet
- Principles of Primary Health Care: Presenter: DR Vaishnavi C Guide: DR Priyadarshini CDocument66 pagesPrinciples of Primary Health Care: Presenter: DR Vaishnavi C Guide: DR Priyadarshini CMarwa FoudNo ratings yet
- WeeFIM Clinical ReviewDocument10 pagesWeeFIM Clinical Reviewsss_sarzzzNo ratings yet
- NCM 108 - Bioethics - Chapter 4Document2 pagesNCM 108 - Bioethics - Chapter 4Rohoney LogronioNo ratings yet
- A Rare Case Report: Abdominal Muscle Myoclonic JerksDocument4 pagesA Rare Case Report: Abdominal Muscle Myoclonic JerksasclepiuspdfsNo ratings yet
- TENECTEPLASE (Metalyse®) Protocol: Wentworth Area Health ServiceDocument3 pagesTENECTEPLASE (Metalyse®) Protocol: Wentworth Area Health ServiceillusionilluNo ratings yet
- Level 12 Passage 1-1-3Document3 pagesLevel 12 Passage 1-1-3SalinasPalominoSebastianNo ratings yet
- Plasma Pen - Consultation & Consent FormDocument10 pagesPlasma Pen - Consultation & Consent FormDS Hz Vega100% (1)
- Co-Trimoxazole Drug StudyDocument1 pageCo-Trimoxazole Drug Studyjonelo123100% (1)
- JHA For Crates-Boxes With Potential Hazardous SubstancesDocument4 pagesJHA For Crates-Boxes With Potential Hazardous SubstancesTnarg RagawNo ratings yet
- Hair Care and Oral CareDocument8 pagesHair Care and Oral Care22 - Fernandez, Lyza Mae D.No ratings yet
- Standards of Good Practice For Spinal Interventional ProceduresDocument20 pagesStandards of Good Practice For Spinal Interventional ProceduresMadyline VictoryaNo ratings yet
- Drug Therapy CP A1Document6 pagesDrug Therapy CP A1Faizah KhalidNo ratings yet
- Care Giver Stress IndexDocument2 pagesCare Giver Stress IndexcpradheepNo ratings yet
- MalpresentationDocument16 pagesMalpresentationAnghel CruzNo ratings yet
- Computer Commerce PDFDocument176 pagesComputer Commerce PDFMallu TechNo ratings yet
- Development of A Sports ComplexDocument13 pagesDevelopment of A Sports ComplexJosua Biadno MenisNo ratings yet
- Malt Extract Italia MsdsDocument6 pagesMalt Extract Italia MsdsSorin LazarNo ratings yet
- Hemorrhage Case Studies - in ClassDocument35 pagesHemorrhage Case Studies - in ClassMile100% (2)
- Pagpamaeandong Kaibahan Si Bantay A Phenomenological Study On The Mental and Emotional Influence of Dog OwnershipDocument110 pagesPagpamaeandong Kaibahan Si Bantay A Phenomenological Study On The Mental and Emotional Influence of Dog OwnershipShane UretaNo ratings yet
- Drug Study MisoprostolDocument2 pagesDrug Study Misoprostolrica sebabillones100% (1)
- Drug Card AmbienDocument1 pageDrug Card AmbienAdrianne Bazo100% (1)
- Office: The of The SecretaryDocument3 pagesOffice: The of The SecretaryElaine DabuNo ratings yet
- Afbc 404 F 2 Baf 1 D 1Document29 pagesAfbc 404 F 2 Baf 1 D 1api-584621926No ratings yet