You might also like
- 1-Good Health Gold Package - PO2257496339-951Document1 page1-Good Health Gold Package - PO2257496339-951Aafaq BhuttoNo ratings yet
- Dneerajalaxmi 20220611120615333Document1 pageDneerajalaxmi 20220611120615333Donthula SripathiNo ratings yet
- Deepika.R:::: Patient Age / Sex 26 Y / Female BranchDocument2 pagesDeepika.R:::: Patient Age / Sex 26 Y / Female BranchkannanNo ratings yet
- Patient ReportDocument7 pagesPatient ReportY2J FilmsNo ratings yet
- R3Document1 pageR3Asif ButtNo ratings yet
- SaritaDocument2 pagesSaritaPushpanjaliNo ratings yet
- FM Report Download PDFDocument1 pageFM Report Download PDFNitish PonneboyinaNo ratings yet
- Patient test results for Mrs. Lakshmi PrasannaDocument4 pagesPatient test results for Mrs. Lakshmi PrasannaSiva JabilliNo ratings yet
- Thyroid Profile (Total T3, Total T4, TSH), Serum: EcliaDocument3 pagesThyroid Profile (Total T3, Total T4, TSH), Serum: EcliaRoopa gowdaNo ratings yet
- Final: L16 - Bhopal 6 - CC Shop No.10, Shakti Nagar Shopping Complex, Shakti Nagar, Bhopal-4 BHOPAL 462024Document1 pageFinal: L16 - Bhopal 6 - CC Shop No.10, Shakti Nagar Shopping Complex, Shakti Nagar, Bhopal-4 BHOPAL 462024Lalita KacherNo ratings yet
- LPL - Paschim Vhr-Iv Dr. Umesh Mittal, House No - 233, Block A-5 DelhiDocument1 pageLPL - Paschim Vhr-Iv Dr. Umesh Mittal, House No - 233, Block A-5 DelhiSupriya SukhejaNo ratings yet
- Jotsna Meshram PDFDocument1 pageJotsna Meshram PDFYashNo ratings yet
- Fever Panel BasicDocument7 pagesFever Panel BasicMadNo ratings yet
- S14 - FPSC Rakesh Marg J-3, Pushpanjali Complex, Nehru Nagar Rakesh Marg, Ghaziabad-Utp, IndDocument2 pagesS14 - FPSC Rakesh Marg J-3, Pushpanjali Complex, Nehru Nagar Rakesh Marg, Ghaziabad-Utp, Indvijay rastogiNo ratings yet
- Diabetes Screening ReportDocument15 pagesDiabetes Screening ReportShivam AroraNo ratings yet
- Clinical Biochemistry: Sumit Omkant Nile ,, MRDocument2 pagesClinical Biochemistry: Sumit Omkant Nile ,, MRShivRaj Omkant NileNo ratings yet
- SHAKTI KHATRI Report PDFDocument3 pagesSHAKTI KHATRI Report PDFShakti KhatriNo ratings yet
- Ssumangarg@gmail - Com 20220825193722Document13 pagesSsumangarg@gmail - Com 20220825193722Suman GargNo ratings yet
- Date 28/mar/2023 10:09AM Unit Bio Ref Interval: Laboratory Investigation ReportDocument12 pagesDate 28/mar/2023 10:09AM Unit Bio Ref Interval: Laboratory Investigation ReportChauhanNo ratings yet
- Reportpdf1 PDFDocument3 pagesReportpdf1 PDFLifetime AbbeyNo ratings yet
- Sample Type: Visit Id: R8539558Document1 pageSample Type: Visit Id: R8539558Ravi KumarNo ratings yet
- Efbu2630Document4 pagesEfbu2630Aniruddh NagaNo ratings yet
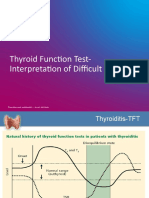
- TFT Interpretation of Difficult CasesDocument51 pagesTFT Interpretation of Difficult CasesAditya GautamNo ratings yet
- Abnormal Thyroid Function in PregnancyDocument54 pagesAbnormal Thyroid Function in Pregnancyasri khazaliNo ratings yet
- Department of Hematology Covid-19 Health Checkup (Post Recovery)Document8 pagesDepartment of Hematology Covid-19 Health Checkup (Post Recovery)Geetika GuptaNo ratings yet
- Dr. Sangeeta Sharma's Thyroid Profile Report for ZainaDocument1 pageDr. Sangeeta Sharma's Thyroid Profile Report for ZainaZaina AkramNo ratings yet
- LPL Bengaluru Reference Lab ReportDocument11 pagesLPL Bengaluru Reference Lab ReportKomal SharmaNo ratings yet
- Vijaya Diagnostic Lab Test ReportDocument1 pageVijaya Diagnostic Lab Test ReportUpender Rao SunkishalaNo ratings yet
- Haematology Complete Blood Count (CBC EXT) : 021808250310 MR - AJAY KUMAR 662326Document7 pagesHaematology Complete Blood Count (CBC EXT) : 021808250310 MR - AJAY KUMAR 662326ANSHU KUMAR RANANo ratings yet
- Department of Hematology Test Name Result Unit Bio. Ref. IntervalDocument3 pagesDepartment of Hematology Test Name Result Unit Bio. Ref. Intervalaf dNo ratings yet
- Diagnostic Report: FinalDocument3 pagesDiagnostic Report: FinalkrishnkantNo ratings yet
- Himani Singhal 56024602023 04 19 10 55 14 598 1 6 452 133264571589922492 PDFDocument16 pagesHimani Singhal 56024602023 04 19 10 55 14 598 1 6 452 133264571589922492 PDFONE SURE LABNo ratings yet
- S14 - FPSC Rajnagar Ext - Ii-Ghaziabad Shop 01, Classic Arcade, Classic Residency Rajanagar Extension GHAZIABAD-201001 GhaziabadDocument2 pagesS14 - FPSC Rajnagar Ext - Ii-Ghaziabad Shop 01, Classic Arcade, Classic Residency Rajanagar Extension GHAZIABAD-201001 GhaziabadSaharsh MittalNo ratings yet
- Biol 460 Case StudyDocument11 pagesBiol 460 Case Studyapi-353888678No ratings yet
- HeaderDocument13 pagesHeaderRoshan Virat PandeyNo ratings yet
- Conference Brochure With Link7Document16 pagesConference Brochure With Link7Shrutik AshiyaniNo ratings yet
- BT01110300041275232 RLS PDFDocument14 pagesBT01110300041275232 RLS PDFnk2k10No ratings yet
- Remotesensing 12 00857 v2Document1 pageRemotesensing 12 00857 v2Rajarshi BhattacharyaNo ratings yet
- Report 831a66a7 PDFDocument23 pagesReport 831a66a7 PDFViral PatelNo ratings yet
- CBC Haemogram Report for Mr. Madhav MaheshwariDocument1 pageCBC Haemogram Report for Mr. Madhav Maheshwarimadhav maheshwariNo ratings yet
- Variations, Errors, and QualityDocument46 pagesVariations, Errors, and QualityJohn Reden RomeroNo ratings yet
- Gds137 Slide HyperthyroidismDocument30 pagesGds137 Slide HyperthyroidismLouie Kem Anthony BabaranNo ratings yet
- eGFR Report for Bhanwar SinghDocument7 pageseGFR Report for Bhanwar SinghDevraj SinghNo ratings yet
- SpectrophotometerDocument13 pagesSpectrophotometerRanjana NailwalNo ratings yet
- LABORATORY and PATHOLOGY Online Report: Patient InformationDocument3 pagesLABORATORY and PATHOLOGY Online Report: Patient InformationRamcoNo ratings yet
- Liver Kidney PanelDocument13 pagesLiver Kidney Panelvishal pundirNo ratings yet
- ReportDocument2 pagesReportSupriya DewanNo ratings yet
- Vijaya Diagnostic Lab Report SummaryDocument3 pagesVijaya Diagnostic Lab Report Summaryrajashekarcse533No ratings yet
- Poonam Thyrocare 7th MarchDocument1 pagePoonam Thyrocare 7th Marchsumit.raj.iiit5613No ratings yet
- 82-Year-Old Male's Comprehensive Blood Test ResultsDocument11 pages82-Year-Old Male's Comprehensive Blood Test ResultsshyamNo ratings yet
- Blood Tests ReportDocument7 pagesBlood Tests ReportLalith GoudNo ratings yet
- Hypothyroid in Pregnancy Andi CakraDocument32 pagesHypothyroid in Pregnancy Andi CakraCakraEkkyNo ratings yet
- 1-Aarogyam 1.2 - PO4080828012-204Document10 pages1-Aarogyam 1.2 - PO4080828012-204jannyyatinNo ratings yet
- Microalbumin Creatinine Ratio - Spot Urine: SR - No Investigation Observed Value Reference Range UnitDocument1 pageMicroalbumin Creatinine Ratio - Spot Urine: SR - No Investigation Observed Value Reference Range Unitdebabrata_dutta678No ratings yet
- Hepatitis "B" Surface Antigen (Hbsag) Parameter Results MethodDocument4 pagesHepatitis "B" Surface Antigen (Hbsag) Parameter Results MethodSachin AgarwalNo ratings yet
- 1-Basic Health Screening (Includes 29 Tests) - PO2403760062-868Document5 pages1-Basic Health Screening (Includes 29 Tests) - PO2403760062-868SMILLING CLOUDNo ratings yet
- Sample ReportDocument8 pagesSample Reportनवीन कुमारNo ratings yet
- Endocrine 160110083024Document65 pagesEndocrine 160110083024Ryan CracknellNo ratings yet
- LabReport-1_editedDocument2 pagesLabReport-1_editedsonunaikratulavathNo ratings yet
- ReportDocument1 pageReportRanjan Mano100% (1)
- Terapia Anabolica y Antiresortiva Secuencial en OsteoporosisDocument11 pagesTerapia Anabolica y Antiresortiva Secuencial en OsteoporosisTony Miguel Saba SabaNo ratings yet
- Early - Detection - and - Management DMT2Document35 pagesEarly - Detection - and - Management DMT2AlfajridrgNo ratings yet
- Polycystic Ovarian Syndrome (PCOS) Diagnosis and TreatmentDocument25 pagesPolycystic Ovarian Syndrome (PCOS) Diagnosis and Treatmenting_claudia100% (3)
- Short Synacthen Test 2Document3 pagesShort Synacthen Test 2sanham100% (2)
- IM-Module B Summarized Notes (IBD)Document69 pagesIM-Module B Summarized Notes (IBD)DeepbluexNo ratings yet
- Acog Practice Bulletin TiroidesDocument10 pagesAcog Practice Bulletin TiroidesMerpi Alvarez Goris100% (1)
- Endocrine ConditionsDocument5 pagesEndocrine ConditionsGlen DizonNo ratings yet
- Thyroiditis Dissertation SignedDocument29 pagesThyroiditis Dissertation SignedRogers256No ratings yet
- Endocrine SystemDocument73 pagesEndocrine SystemIsabel Higgins100% (4)
- Hidden Story of Cancer - Brian Scott PeskinDocument723 pagesHidden Story of Cancer - Brian Scott Peskinawakejoy93% (14)
- Supplement ZadnjaverDocument80 pagesSupplement ZadnjaverikaNo ratings yet
- Health Locus of Control Dan Self-Efficacy Pasien DM: Tipe 2 Dengan Penerapan Modifikasi PsikoedukasiDocument9 pagesHealth Locus of Control Dan Self-Efficacy Pasien DM: Tipe 2 Dengan Penerapan Modifikasi PsikoedukasiahlamNo ratings yet
- Early Insulin TherapyDocument6 pagesEarly Insulin TherapyEKNo ratings yet
- Chennai ThesisDocument22 pagesChennai ThesisShradhanjali PandaNo ratings yet
- Anatomy and Physiology of Adrenal GlandsDocument4 pagesAnatomy and Physiology of Adrenal Glandsxxxcamzxxx100% (3)
- D V Bhaskar - 2019 - 09 - 21Document6 pagesD V Bhaskar - 2019 - 09 - 21asdfNo ratings yet
- Primary and Secondary Anenorrhea 2016-2017Document24 pagesPrimary and Secondary Anenorrhea 2016-2017zianab ali100% (1)
- Endocrinology Teaching CasesDocument47 pagesEndocrinology Teaching CasesBinta BaptisteNo ratings yet
- Gonadal Hormones and Their Pharmacological InhibitorsDocument7 pagesGonadal Hormones and Their Pharmacological InhibitorsHydieNo ratings yet
- Diabetes SobrebasalizaciónDocument7 pagesDiabetes SobrebasalizaciónComisión Académica FCM - UNAHNo ratings yet
- Endocrine Glands: The Master Glands that Control Our HormonesDocument15 pagesEndocrine Glands: The Master Glands that Control Our HormonesJohn Rick PerezNo ratings yet
- Dr. Nalin, AIMSS, New DelhiDocument12 pagesDr. Nalin, AIMSS, New DelhiSyed AhamedNo ratings yet
- Hormon Paratiroid: Dr. Muniroh, SP - PKDocument10 pagesHormon Paratiroid: Dr. Muniroh, SP - PKFuadi FaisalNo ratings yet
- Patient blood test results show abnormal levelsDocument2 pagesPatient blood test results show abnormal levelsHibaBsharatNo ratings yet
- A Case-Based Guide To Clinical Endocrinology (October 23, 2015) - (1493920588) - (Springer)Document434 pagesA Case-Based Guide To Clinical Endocrinology (October 23, 2015) - (1493920588) - (Springer)AbdulraHman KhalEd100% (2)
- Thyroid Disorders TBL Pathology Learning MaterialDocument20 pagesThyroid Disorders TBL Pathology Learning MaterialIrdina SyabilNo ratings yet
- Multiple Endocrine NeoplaciaDocument12 pagesMultiple Endocrine NeoplaciaMalaFatmawatiIbrahimNo ratings yet
- Clinical - Use - and - Practical - Recommendation - DR - DR - Himawan - SanusiDocument20 pagesClinical - Use - and - Practical - Recommendation - DR - DR - Himawan - SanusiFX Fbs NewbieNo ratings yet
- Diabetes Insipidus: Dr.M.Bastanta Tarigan, Sppd-KemdDocument8 pagesDiabetes Insipidus: Dr.M.Bastanta Tarigan, Sppd-KemdAngellina SimanjuntakNo ratings yet