You might also like
- Hyperthyroidsm: EpidemiologyDocument6 pagesHyperthyroidsm: EpidemiologyEllieNo ratings yet
- Gds137 Slide HyperthyroidismDocument30 pagesGds137 Slide HyperthyroidismLouie Kem Anthony BabaranNo ratings yet
- Let's Talk About Thyroid PDFDocument92 pagesLet's Talk About Thyroid PDFEidi IdhamNo ratings yet
- Hypothyroid in Pregnancy Andi CakraDocument32 pagesHypothyroid in Pregnancy Andi CakraCakraEkkyNo ratings yet
- Abnormal Thyroid Function in PregnancyDocument54 pagesAbnormal Thyroid Function in Pregnancyasri khazaliNo ratings yet
- Thyroid Emergencies-Dr. AM IyagbaDocument13 pagesThyroid Emergencies-Dr. AM IyagbaDr. Amb. Monday ZaccheausNo ratings yet
- Hypothyroidism in PregnancyDocument14 pagesHypothyroidism in PregnancyShajia ZafarNo ratings yet
- Biol 460 Case StudyDocument11 pagesBiol 460 Case Studyapi-353888678No ratings yet
- Thyroid and InfertilityDocument36 pagesThyroid and InfertilitySairindri SahooNo ratings yet
- Week 3 Pharmaco Part 2Document34 pagesWeek 3 Pharmaco Part 2Tiko JomidavaNo ratings yet
- Graves' Hyperthyroidism in Pregnancy: A Clinical ReviewDocument22 pagesGraves' Hyperthyroidism in Pregnancy: A Clinical ReviewAnisa Dinda NurlianaNo ratings yet
- Thyroid DX PXLDocument62 pagesThyroid DX PXLabduljebarNo ratings yet
- Thyroid Panel-1 (T3/T4/TSH) : Investigation Observed Value Unit Biological Reference IntervalDocument2 pagesThyroid Panel-1 (T3/T4/TSH) : Investigation Observed Value Unit Biological Reference IntervalShashikantNo ratings yet
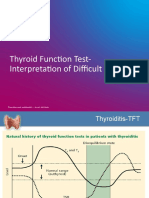
- TFT Interpretation of Difficult CasesDocument51 pagesTFT Interpretation of Difficult CasesAditya GautamNo ratings yet
- The Role of Maternal Thyroid Status On Pregnancy Outcome For Motherand NewbornDocument36 pagesThe Role of Maternal Thyroid Status On Pregnancy Outcome For Motherand NewbornRahmayantiYuliaNo ratings yet
- Levothyroxine in TPO+ euthyroid women before conceptionDocument18 pagesLevothyroxine in TPO+ euthyroid women before conceptionRoxana TudorNo ratings yet
- FunctionTests Brochure PDFDocument2 pagesFunctionTests Brochure PDFArslan SaleemNo ratings yet
- CHN1 Health Care Delivery System2Document22 pagesCHN1 Health Care Delivery System2MicaNo ratings yet
- Variations, Errors, and QualityDocument46 pagesVariations, Errors, and QualityJohn Reden RomeroNo ratings yet
- Conference Brochure With Link7Document16 pagesConference Brochure With Link7Shrutik AshiyaniNo ratings yet
- AACE and ATA 2012 Clinical Practice Guidelines for HypothyroidismDocument63 pagesAACE and ATA 2012 Clinical Practice Guidelines for HypothyroidismNur Rakhma AkmaliaNo ratings yet
- Critical Aspect Analytical Test Review: Jakarta 14 December 2017 Speaker: Heru Purnomo, STDocument24 pagesCritical Aspect Analytical Test Review: Jakarta 14 December 2017 Speaker: Heru Purnomo, STMohammad Naufal AliefNo ratings yet
- Guidelines of The American Thyroid Association PREGNANCY PDFDocument47 pagesGuidelines of The American Thyroid Association PREGNANCY PDFIqra AnugerahNo ratings yet
- Thyroid Function TestDocument28 pagesThyroid Function TestDhinesh Muthusamy100% (1)
- Hyperthyroidism: A Practical Approach To Diagnosis and ManagementDocument70 pagesHyperthyroidism: A Practical Approach To Diagnosis and ManagementMutiara Manuella TambaNo ratings yet
- Drug Management of Thyroid DiseaseDocument22 pagesDrug Management of Thyroid DiseaseHassan.shehri100% (6)
- Therapeutics: Thyroid DisordersDocument24 pagesTherapeutics: Thyroid DisordersSharas FarhadNo ratings yet
- Thyroid DisordersDocument67 pagesThyroid DisordersMA 09No ratings yet
- Parathyroid-Hormone Calcium HomeostasisDocument58 pagesParathyroid-Hormone Calcium HomeostasisSudhakar LakavathNo ratings yet
- Interpreting Thyroid Tests: Key FactorsDocument7 pagesInterpreting Thyroid Tests: Key FactorsStrawberry ShortcakeNo ratings yet
- Thyroiddisease 190216062020Document42 pagesThyroiddisease 190216062020Manikandan Vp100% (1)
- Surgical Pathology For Dentistry Students - Surgical Pathology of Thyroid and Adrenal GlandsDocument38 pagesSurgical Pathology For Dentistry Students - Surgical Pathology of Thyroid and Adrenal Glandssorin niky mocanu100% (1)
- Thyroid Emergencies: Abrar AlharbiDocument35 pagesThyroid Emergencies: Abrar AlharbiabrarNo ratings yet
- HyperthyroidDocument12 pagesHyperthyroidChristine Joy PepitoNo ratings yet
- Thyrotoxicosis: Presenter: Emiacu Kenneth Facilitator: Dr. Freddie KibengoDocument35 pagesThyrotoxicosis: Presenter: Emiacu Kenneth Facilitator: Dr. Freddie KibengoNinaNo ratings yet
- Endocrine Pathology - UntadDocument158 pagesEndocrine Pathology - UntadfahrulrozyNo ratings yet
- ThyrotoxicosisDocument105 pagesThyrotoxicosisAli Murtaza Abbas100% (1)
- Thyroid Care - A Nine Step Program For Busy WomenDocument161 pagesThyroid Care - A Nine Step Program For Busy WomenAnisa A Abeytia100% (3)
- Lecture 29 30 Thyroid TherapeuticsDocument3 pagesLecture 29 30 Thyroid TherapeuticsAhmed MashalyNo ratings yet
- HYPOTHYROIDISMDocument30 pagesHYPOTHYROIDISMTopeNo ratings yet
- THYROIDDocument100 pagesTHYROIDFrance PalNo ratings yet
- Laboratory Diagnostics of (Selected) Endocrine DisordersDocument48 pagesLaboratory Diagnostics of (Selected) Endocrine DisordersPaulina PaskeviciuteNo ratings yet
- Thyroid PathophysiologyDocument7 pagesThyroid PathophysiologyS RiarNo ratings yet
- Thyroid DisordersDocument29 pagesThyroid DisordersEMPINo ratings yet
- Grave'S Disease: Farida Ulfa 1510211057Document11 pagesGrave'S Disease: Farida Ulfa 1510211057farida ulfaNo ratings yet
- 1-Good Health Gold Package - PO2257496339-951Document1 page1-Good Health Gold Package - PO2257496339-951Aafaq BhuttoNo ratings yet
- Lab Report NewDocument2 pagesLab Report Newnsdh5v5v5sNo ratings yet
- HipothyroidDocument48 pagesHipothyroidCakraEkkyNo ratings yet
- Hypothalamic Pitutary Axis and Thyroid Hormone SynthesisDocument5 pagesHypothalamic Pitutary Axis and Thyroid Hormone Synthesis78 shivangi mauryaNo ratings yet
- '3'hyperthyroid and HypothyroidDocument42 pages'3'hyperthyroid and Hypothyroidafriskha bulawanNo ratings yet
- Thyroid Disease: Presentation By: Pimundu Vicent Audo Ritah Tutor: Dr. Fualal JaneDocument41 pagesThyroid Disease: Presentation By: Pimundu Vicent Audo Ritah Tutor: Dr. Fualal JaneEsther AumaNo ratings yet
- Hypothyroidism in Pregnancy: Causes, Effects and ManagementDocument29 pagesHypothyroidism in Pregnancy: Causes, Effects and ManagementhanaddulNo ratings yet
- Thyroid Function Test 12-2-09Document69 pagesThyroid Function Test 12-2-09Romaysaamohamed AlyNo ratings yet
- Triglycerides and VLDL: (Increased Ra Tio of Triglyceride To Apob)Document20 pagesTriglycerides and VLDL: (Increased Ra Tio of Triglyceride To Apob)Indah Pujiati DtNo ratings yet
- Thyroid Function Tests: Understanding the Hidden Health ProblemDocument34 pagesThyroid Function Tests: Understanding the Hidden Health Problemvjanand07100% (1)
- HyperthyroidismDocument18 pagesHyperthyroidismWahyuni FatmonaNo ratings yet
- Pathophysiology of Endocrine SystemDocument64 pagesPathophysiology of Endocrine SystemTess MohamedNo ratings yet
- Thyroid GlandDocument30 pagesThyroid GlandahmedkomranNo ratings yet
- Autoverification ImplementationDocument53 pagesAutoverification ImplementationEi JamNo ratings yet
- Summary of Medical EmergenciesDocument24 pagesSummary of Medical Emergenciesbasharswork99No ratings yet
- ANP RAM Sepsis ModuleDocument56 pagesANP RAM Sepsis ModuleRyan CracknellNo ratings yet
- Aortic Dissection PaperDocument10 pagesAortic Dissection PaperRyan CracknellNo ratings yet
- Abdullah OxygenDocument2 pagesAbdullah OxygenRyan CracknellNo ratings yet
- Age Adjusted D-Dimer Edit 27-06-22Document9 pagesAge Adjusted D-Dimer Edit 27-06-22Ryan CracknellNo ratings yet
- J Jacc 2023 02 011Document3 pagesJ Jacc 2023 02 011Evania BeatriceNo ratings yet
- Life - Course Model NFBCDocument8 pagesLife - Course Model NFBCShayekh M ArifNo ratings yet
- Chromosomal AnomaliesDocument30 pagesChromosomal AnomaliesJohn MccartneyNo ratings yet
- Dating ViolenceDocument3 pagesDating Violenceapi-490237409No ratings yet
- Hepatic PackingDocument4 pagesHepatic PackingRESIDENTES CIRUGIA IMSSNo ratings yet
- Still Pallet Stacker Sd20 1613 Operating Manual deDocument23 pagesStill Pallet Stacker Sd20 1613 Operating Manual dejanetbenton090185xqb100% (117)
- A Prospective, Longitudinal, Study of Men With Borderline Personality Disorder With and Without Comorbid Antisocial Personality DisorderDocument13 pagesA Prospective, Longitudinal, Study of Men With Borderline Personality Disorder With and Without Comorbid Antisocial Personality DisorderJuan BacelarNo ratings yet
- AMH Talk MH Workplace FINAL Oct 2014Document38 pagesAMH Talk MH Workplace FINAL Oct 2014Princess RanyNo ratings yet
- Test Bank For Pathophysiology 6th Edition Jacquelyn L BanasikDocument3 pagesTest Bank For Pathophysiology 6th Edition Jacquelyn L BanasikKenneth Maestas100% (27)
- Tachipirina Orosolubile: 500 MG Granules, Strawberry-Vanilla FlavorDocument3 pagesTachipirina Orosolubile: 500 MG Granules, Strawberry-Vanilla Flavordenis troshaniNo ratings yet
- Bronchiectasis - A Clinical ReviewDocument13 pagesBronchiectasis - A Clinical Reviewrudy sanabriaNo ratings yet
- Marcil 2001Document4 pagesMarcil 2001Mariana JuravleNo ratings yet
- Infectious Disease Management: Student GuideDocument54 pagesInfectious Disease Management: Student GuideNisa AzzaleaNo ratings yet
- Assessment of Effectiveness of Structured Teaching Programme On Knowledge Regarding Dengue FeverDocument5 pagesAssessment of Effectiveness of Structured Teaching Programme On Knowledge Regarding Dengue FeverEditor IJTSRDNo ratings yet
- Heat Illness Prevention ProgramDocument7 pagesHeat Illness Prevention ProgramSPIQCNo ratings yet
- MDCG 2020-10-2 - Saf Rep Clin Inv MDDocument715 pagesMDCG 2020-10-2 - Saf Rep Clin Inv MDLorenaNo ratings yet
- Neuro Year 3 MedEd Rehaan Khokar 2Document91 pagesNeuro Year 3 MedEd Rehaan Khokar 2Sugoi SagaNo ratings yet
- Capstone PPDocument20 pagesCapstone PPapi-569838480No ratings yet
- Elimination Disorder - A Psychiatric Paediatric DisorderDocument22 pagesElimination Disorder - A Psychiatric Paediatric DisorderMeghana PatilNo ratings yet
- Influenza B SymptomsDocument5 pagesInfluenza B SymptomsHoonchyi KohNo ratings yet
- Social Studies SbaDocument26 pagesSocial Studies SbaKeasha Jones100% (1)
- Soc Sci 112 Module 4 StudentDocument7 pagesSoc Sci 112 Module 4 StudentLeah Lorenzana MalabananNo ratings yet
- MahamTahir PDFDocument6 pagesMahamTahir PDFAdeel AizadNo ratings yet
- A Clinical Study To Evaluate The Efficacy of Shudha Bala Taila Matra Basti in The Management of Kampavata With Special Reference To Parkinson's DiseaseDocument5 pagesA Clinical Study To Evaluate The Efficacy of Shudha Bala Taila Matra Basti in The Management of Kampavata With Special Reference To Parkinson's DiseaseEditor IJTSRDNo ratings yet
- (Equine Veterinary Journal 2010-Jan 05 Vol. 37 Iss. 2) W. W. MUIR - Pain Therapy in Horses (2010) (10.2746 - 0425164054223831) - Libgen - LiDocument3 pages(Equine Veterinary Journal 2010-Jan 05 Vol. 37 Iss. 2) W. W. MUIR - Pain Therapy in Horses (2010) (10.2746 - 0425164054223831) - Libgen - LiAcupuntura de EquinosNo ratings yet
- Commentary "Incidence of Total Thyroidectomy and Lobectomy"Document2 pagesCommentary "Incidence of Total Thyroidectomy and Lobectomy"Cristina RamirezNo ratings yet
- Belly Gud For Health - Department of Health WebsiteDocument2 pagesBelly Gud For Health - Department of Health WebsiteJL Calvin100% (1)
- Sports InjuryDocument31 pagesSports InjuryANTONETTE DUMALENo ratings yet
- Sections of Lab - EssayDocument3 pagesSections of Lab - EssayhalamanNo ratings yet
- PAR Q FORM (Pre Activity Readiness Questionnaire) With COVID-19 (FINAL)Document2 pagesPAR Q FORM (Pre Activity Readiness Questionnaire) With COVID-19 (FINAL)Jhona Marie FuellasNo ratings yet