You might also like
- Hypothyroidism in PregnancyDocument14 pagesHypothyroidism in PregnancyShajia ZafarNo ratings yet
- Abnormal Thyroid Function in PregnancyDocument54 pagesAbnormal Thyroid Function in Pregnancyasri khazaliNo ratings yet
- Thyroid DX PXLDocument62 pagesThyroid DX PXLabduljebarNo ratings yet
- Thyroid and InfertilityDocument36 pagesThyroid and InfertilitySairindri SahooNo ratings yet
- Levothyroxine in TPO+ euthyroid women before conceptionDocument18 pagesLevothyroxine in TPO+ euthyroid women before conceptionRoxana TudorNo ratings yet
- HipothyroidDocument48 pagesHipothyroidCakraEkkyNo ratings yet
- Hypothyroid in Pregnancy Andi CakraDocument32 pagesHypothyroid in Pregnancy Andi CakraCakraEkkyNo ratings yet
- The Role of Maternal Thyroid Status On Pregnancy Outcome For Motherand NewbornDocument36 pagesThe Role of Maternal Thyroid Status On Pregnancy Outcome For Motherand NewbornRahmayantiYuliaNo ratings yet
- Hyperthyroidsm: EpidemiologyDocument6 pagesHyperthyroidsm: EpidemiologyEllieNo ratings yet
- Gds137 Slide HyperthyroidismDocument30 pagesGds137 Slide HyperthyroidismLouie Kem Anthony BabaranNo ratings yet
- Week 3 Pharmaco Part 2Document34 pagesWeek 3 Pharmaco Part 2Tiko JomidavaNo ratings yet
- Biol 460 Case StudyDocument11 pagesBiol 460 Case Studyapi-353888678No ratings yet
- Let's Talk About Thyroid PDFDocument92 pagesLet's Talk About Thyroid PDFEidi IdhamNo ratings yet
- Thyroid Emergencies-Dr. AM IyagbaDocument13 pagesThyroid Emergencies-Dr. AM IyagbaDr. Amb. Monday ZaccheausNo ratings yet
- Thyroid Panel-1 (T3/T4/TSH) : Investigation Observed Value Unit Biological Reference IntervalDocument2 pagesThyroid Panel-1 (T3/T4/TSH) : Investigation Observed Value Unit Biological Reference IntervalShashikantNo ratings yet
- Endocrine 160110083024Document65 pagesEndocrine 160110083024Ryan CracknellNo ratings yet
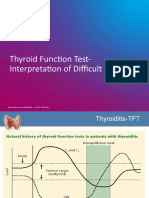
- TFT Interpretation of Difficult CasesDocument51 pagesTFT Interpretation of Difficult CasesAditya GautamNo ratings yet
- CHN1 Health Care Delivery System2Document22 pagesCHN1 Health Care Delivery System2MicaNo ratings yet
- Conference Brochure With Link7Document16 pagesConference Brochure With Link7Shrutik AshiyaniNo ratings yet
- FunctionTests Brochure PDFDocument2 pagesFunctionTests Brochure PDFArslan SaleemNo ratings yet
- Variations, Errors, and QualityDocument46 pagesVariations, Errors, and QualityJohn Reden RomeroNo ratings yet
- Guidelines of The American Thyroid Association PREGNANCY PDFDocument47 pagesGuidelines of The American Thyroid Association PREGNANCY PDFIqra AnugerahNo ratings yet
- AACE and ATA 2012 Clinical Practice Guidelines for HypothyroidismDocument63 pagesAACE and ATA 2012 Clinical Practice Guidelines for HypothyroidismNur Rakhma AkmaliaNo ratings yet
- Critical Aspect Analytical Test Review: Jakarta 14 December 2017 Speaker: Heru Purnomo, STDocument24 pagesCritical Aspect Analytical Test Review: Jakarta 14 December 2017 Speaker: Heru Purnomo, STMohammad Naufal AliefNo ratings yet
- Hyperthyroidism: A Practical Approach To Diagnosis and ManagementDocument70 pagesHyperthyroidism: A Practical Approach To Diagnosis and ManagementMutiara Manuella TambaNo ratings yet
- Interpreting Thyroid Tests: Key FactorsDocument7 pagesInterpreting Thyroid Tests: Key FactorsStrawberry ShortcakeNo ratings yet
- Drug Management of Thyroid DiseaseDocument22 pagesDrug Management of Thyroid DiseaseHassan.shehri100% (6)
- Thyroid Function TestDocument28 pagesThyroid Function TestDhinesh Muthusamy100% (1)
- Thyroid DisordersDocument67 pagesThyroid DisordersMA 09No ratings yet
- Thyroid Emergencies: Abrar AlharbiDocument35 pagesThyroid Emergencies: Abrar AlharbiabrarNo ratings yet
- Therapeutics: Thyroid DisordersDocument24 pagesTherapeutics: Thyroid DisordersSharas FarhadNo ratings yet
- Surgical Pathology For Dentistry Students - Surgical Pathology of Thyroid and Adrenal GlandsDocument38 pagesSurgical Pathology For Dentistry Students - Surgical Pathology of Thyroid and Adrenal Glandssorin niky mocanu100% (1)
- Parathyroid-Hormone Calcium HomeostasisDocument58 pagesParathyroid-Hormone Calcium HomeostasisSudhakar LakavathNo ratings yet
- ThyrotoxicosisDocument105 pagesThyrotoxicosisAli Murtaza Abbas100% (1)
- Thyroiddisease 190216062020Document42 pagesThyroiddisease 190216062020Manikandan Vp100% (1)
- Fertility: Assessment and Treatment For People With Fertility ProblemsDocument4 pagesFertility: Assessment and Treatment For People With Fertility ProblemsPatrick CoghlanNo ratings yet
- Hypothalamic Pitutary Axis and Thyroid Hormone SynthesisDocument5 pagesHypothalamic Pitutary Axis and Thyroid Hormone Synthesis78 shivangi mauryaNo ratings yet
- Thyroid DisordersDocument29 pagesThyroid DisordersEMPINo ratings yet
- 1-Good Health Gold Package - PO2257496339-951Document1 page1-Good Health Gold Package - PO2257496339-951Aafaq BhuttoNo ratings yet
- Endocrine Pathology - UntadDocument158 pagesEndocrine Pathology - UntadfahrulrozyNo ratings yet
- HyperthyroidDocument12 pagesHyperthyroidChristine Joy PepitoNo ratings yet
- HYPOTHYROIDISMDocument30 pagesHYPOTHYROIDISMTopeNo ratings yet
- Laboratory Diagnostics of (Selected) Endocrine DisordersDocument48 pagesLaboratory Diagnostics of (Selected) Endocrine DisordersPaulina PaskeviciuteNo ratings yet
- Lab Report NewDocument2 pagesLab Report Newnsdh5v5v5sNo ratings yet
- Grave'S Disease: Farida Ulfa 1510211057Document11 pagesGrave'S Disease: Farida Ulfa 1510211057farida ulfaNo ratings yet
- Thyroid PathophysiologyDocument7 pagesThyroid PathophysiologyS RiarNo ratings yet
- Thyrotoxicosis: Presenter: Emiacu Kenneth Facilitator: Dr. Freddie KibengoDocument35 pagesThyrotoxicosis: Presenter: Emiacu Kenneth Facilitator: Dr. Freddie KibengoNinaNo ratings yet
- Hypothyroidism in Pregnancy: Causes, Effects and ManagementDocument29 pagesHypothyroidism in Pregnancy: Causes, Effects and ManagementhanaddulNo ratings yet
- Thyroid Care - A Nine Step Program For Busy WomenDocument161 pagesThyroid Care - A Nine Step Program For Busy WomenAnisa A Abeytia100% (3)
- Lecture 29 30 Thyroid TherapeuticsDocument3 pagesLecture 29 30 Thyroid TherapeuticsAhmed MashalyNo ratings yet
- AGE AND DRUG DISPOSITION FACTORSDocument35 pagesAGE AND DRUG DISPOSITION FACTORSMalueth AnguiNo ratings yet
- THYROIDDocument100 pagesTHYROIDFrance PalNo ratings yet
- '3'hyperthyroid and HypothyroidDocument42 pages'3'hyperthyroid and Hypothyroidafriskha bulawanNo ratings yet
- Subclinical Thyroid DiseaseDocument50 pagesSubclinical Thyroid Diseaseกรคุง ภิญโญพจนารถNo ratings yet
- Thyroid Function Test 12-2-09Document69 pagesThyroid Function Test 12-2-09Romaysaamohamed AlyNo ratings yet
- HyperthyroidismDocument18 pagesHyperthyroidismWahyuni FatmonaNo ratings yet
- Thyroid Profile (Total T3, Total T4, TSH), Serum: EcliaDocument3 pagesThyroid Profile (Total T3, Total T4, TSH), Serum: EcliaRoopa gowdaNo ratings yet
- Thyroid Disease in PregnancyDocument36 pagesThyroid Disease in Pregnancypeni_dwiNo ratings yet
- Graves' Disease & PregnancyDocument19 pagesGraves' Disease & Pregnancyrajan kumar100% (1)
- Good Clinical Practice Advice: Thyroid and PregnancyDocument5 pagesGood Clinical Practice Advice: Thyroid and Pregnancyjuan carlos pradaNo ratings yet
- Allergic Rhinitis and Bronchial Asthma: Parthiv MehtaDocument4 pagesAllergic Rhinitis and Bronchial Asthma: Parthiv MehtaAnisa Dinda NurlianaNo ratings yet
- Format LabDocument1 pageFormat LabAnisa DindanurNo ratings yet
- GenogramDocument1 pageGenogramAnisa Dinda NurlianaNo ratings yet
- Daftar PustakaDocument2 pagesDaftar PustakaNur Annisa Laras FikriaNo ratings yet
- Complete Tds CourseDocument32 pagesComplete Tds CourseAMLANNo ratings yet
- MSDS Slideway Oil Iso VG 68 - 031115Document6 pagesMSDS Slideway Oil Iso VG 68 - 031115Rini SiskayantiNo ratings yet
- SECURED TRANSACTION BAR CHECKLISTDocument4 pagesSECURED TRANSACTION BAR CHECKLISTatw4377100% (1)
- Astm D 2783 - 03Document9 pagesAstm D 2783 - 03Sérgio Luiz RodriguesNo ratings yet
- Home BMW F11 530D Xdrive Touring Wiring Diagrams and Functional DescriptionDocument1 pageHome BMW F11 530D Xdrive Touring Wiring Diagrams and Functional DescriptionOliver AlfaroNo ratings yet
- Investigation of Nursing Students Knowledge of and Attitudes About Problem Based LearningDocument4 pagesInvestigation of Nursing Students Knowledge of and Attitudes About Problem Based LearningasdasdasdasNo ratings yet
- A933 Transistor DatasheetDocument5 pagesA933 Transistor Datasheetshorman67134No ratings yet
- Desantis, AlanDocument18 pagesDesantis, AlanOreillerNo ratings yet
- Course Outline TP WindowsDocument6 pagesCourse Outline TP WindowsAnonymous PcPkRpAKD5No ratings yet
- Analgesia SystemDocument7 pagesAnalgesia SystemMudassar Roomi100% (1)
- MathWorks Interview ProcessDocument2 pagesMathWorks Interview ProcessPawan Singh100% (1)
- Weap - ModflowDocument20 pagesWeap - Modflowguive3No ratings yet
- Chemists 12-2023Document7 pagesChemists 12-2023PRC BaguioNo ratings yet
- Analisis Hasil Led Pada Jam Pertama Dan Jam KeduaDocument11 pagesAnalisis Hasil Led Pada Jam Pertama Dan Jam KeduavirafutmainnarNo ratings yet
- HackSpace - June 2021Document116 pagesHackSpace - June 2021Somnath100% (1)
- X-Plane Installer LogDocument3 pagesX-Plane Installer LogMarsala NistoNo ratings yet
- Kristine Jane T. Zipagan Assignment: 1. Parts of InfographicsDocument2 pagesKristine Jane T. Zipagan Assignment: 1. Parts of InfographicsChristyNo ratings yet
- XFARDocument14 pagesXFARRIZA SAMPAGANo ratings yet
- Taxation Management AssignmentDocument11 pagesTaxation Management AssignmentniraliNo ratings yet
- Analog and Digital Communication Systems: The Transmission of Information Is Called CommunicationDocument71 pagesAnalog and Digital Communication Systems: The Transmission of Information Is Called Communication20-403 TejashwiniNo ratings yet
- The 9 Building Blocks of Business ModelsDocument3 pagesThe 9 Building Blocks of Business ModelsTobeFrankNo ratings yet
- Eddy Current Testing Exam Questions Assignment2Document1 pageEddy Current Testing Exam Questions Assignment2Narotam Kumar GupteshwarNo ratings yet
- Folktalesofkeral 00 MenoDocument124 pagesFolktalesofkeral 00 Menoreena sudhirNo ratings yet
- Business Letter WritingDocument13 pagesBusiness Letter WritingAlex Alexandru100% (1)
- Saura, Jasmin E. - DVM - 2B Biochemistry (Activity 2)Document2 pagesSaura, Jasmin E. - DVM - 2B Biochemistry (Activity 2)Jasmin SauraNo ratings yet
- Gujrat Newspaper IndustryDocument14 pagesGujrat Newspaper IndustryAlok MahajanNo ratings yet
- E VTOLDocument12 pagesE VTOLsaikumar raviNo ratings yet
- Uconnect User GuideDocument113 pagesUconnect User GuidetamilarasansrtNo ratings yet
- LinAlg CompleteDocument331 pagesLinAlg Completes0uizNo ratings yet
- Role of Various Avonoids: Hypotheses On Novel Approach To Treat DiabetesDocument6 pagesRole of Various Avonoids: Hypotheses On Novel Approach To Treat DiabetesYuliet SusantoNo ratings yet