You might also like
- Book Preparing For Weight Loss Surgery Workbook PDFDocument140 pagesBook Preparing For Weight Loss Surgery Workbook PDFArran KennedyNo ratings yet
- Kiminori Sato (Auth.) - Functional Histoanatomy of The Human Larynx-Springer Singapore (2018) PDFDocument334 pagesKiminori Sato (Auth.) - Functional Histoanatomy of The Human Larynx-Springer Singapore (2018) PDFMdacNo ratings yet
- Head and Neck Cancer and Its Treatment: Historical ReviewDocument12 pagesHead and Neck Cancer and Its Treatment: Historical ReviewMdacNo ratings yet
- First Aid and Water Safety Course PlanDocument2 pagesFirst Aid and Water Safety Course PlanTea AnnNo ratings yet
- Bactomin Product MonographDocument43 pagesBactomin Product MonographVivek AlaiNo ratings yet
- Palpable Nodules After Autologous Fat Grafting in Breast Cancer Patients: Incidence and Impact On Follow-UpDocument9 pagesPalpable Nodules After Autologous Fat Grafting in Breast Cancer Patients: Incidence and Impact On Follow-UpMarcos LouroNo ratings yet
- Breast Cancer SurgeryDocument6 pagesBreast Cancer SurgeryΔρ Βαιος ΑγγελοπουλοςNo ratings yet
- JBC 15 350Document6 pagesJBC 15 350Andres VasquezNo ratings yet
- Residual Breast Tissue After Mastectomy, How Often and Where It Is LocatedDocument11 pagesResidual Breast Tissue After Mastectomy, How Often and Where It Is LocatedBunga Tri AmandaNo ratings yet
- Clinical Study: Extreme Oncoplastic Surgery For Multifocal/Multicentric and Locally Advanced Breast CancerDocument9 pagesClinical Study: Extreme Oncoplastic Surgery For Multifocal/Multicentric and Locally Advanced Breast CancerAsti DwiningsihNo ratings yet
- ASCO 2014 CrossDocument6 pagesASCO 2014 Crossdrrajeshb77No ratings yet
- Procedural Difficulty Differences According To TumDocument11 pagesProcedural Difficulty Differences According To TumDaniel Gonzales LinoNo ratings yet
- The Accuracy of Magnetic Resonance Imaging For Preoperative Deep Myometrium Assessment in Endometrial CancerDocument5 pagesThe Accuracy of Magnetic Resonance Imaging For Preoperative Deep Myometrium Assessment in Endometrial CancerDeviat Ast AmierNo ratings yet
- Zigras 2017Document11 pagesZigras 2017tika apriliaNo ratings yet
- Pi Is 0748798320304078Document7 pagesPi Is 0748798320304078Florina PopaNo ratings yet
- Journal of Surgical Oncology - 2013 - Fortunato - When Mastectomy Is Needed Is The Nipple Sparing Procedure A New StandardDocument6 pagesJournal of Surgical Oncology - 2013 - Fortunato - When Mastectomy Is Needed Is The Nipple Sparing Procedure A New StandardJethro ConcepcionNo ratings yet
- IJHEGY-Volume 1-Issue 3 - Page 84-95Document12 pagesIJHEGY-Volume 1-Issue 3 - Page 84-95Abo-ahmed ElmasryNo ratings yet
- 816-Article Text-5949-1-10-20230609Document6 pages816-Article Text-5949-1-10-20230609NikadekPramesti Dewi Puspita SariNo ratings yet
- Postoperative Outcomes of Breast Reconstruction AfDocument6 pagesPostoperative Outcomes of Breast Reconstruction AfDiana AlexandraNo ratings yet
- Kopkash 2018Document6 pagesKopkash 2018Yefry Onil Santana MarteNo ratings yet
- Surgery For Cervical Cancer Consensus & ControversiesDocument9 pagesSurgery For Cervical Cancer Consensus & ControversiesmilenahugueninNo ratings yet
- Evaluation of Axillary Lymphadenopathy With Carcinoma BreastDocument42 pagesEvaluation of Axillary Lymphadenopathy With Carcinoma BreastMashrufNo ratings yet
- EJHM - Volume 89 جامعه الزقازيقDocument9 pagesEJHM - Volume 89 جامعه الزقازيقفاطمة الزهراء أسامةNo ratings yet
- Clough K Oncoplasty BJSDocument7 pagesClough K Oncoplasty BJSkomlanihou_890233161No ratings yet
- Quilting after mastectomy reduces seromaDocument5 pagesQuilting after mastectomy reduces seromabeepboop20No ratings yet
- Long-Term Cosmesis Following A Novel Schedule ofDocument7 pagesLong-Term Cosmesis Following A Novel Schedule ofEmin PehlivanogluNo ratings yet
- Prot SAP 000 PDFDocument11 pagesProt SAP 000 PDFdrrajeshb77No ratings yet
- Regional Nodal Irradiation in Early-Stage Breast CancerDocument10 pagesRegional Nodal Irradiation in Early-Stage Breast Canceryingming zhuNo ratings yet
- 1 s2.0 S174868151730181X MainDocument9 pages1 s2.0 S174868151730181X MainChiara BoccalettoNo ratings yet
- Hidetaka Nomura Et Al. (2015)Document4 pagesHidetaka Nomura Et Al. (2015)Janardana GedeNo ratings yet
- Nottingham Approach to Therapeutic Mammoplasty Improves Cosmetic OutcomesDocument13 pagesNottingham Approach to Therapeutic Mammoplasty Improves Cosmetic OutcomesimtinanNo ratings yet
- Abstracts 991: ST STDocument1 pageAbstracts 991: ST STAli Sibra MulluziNo ratings yet
- Detecting Early Breast Cancer with ImagingDocument38 pagesDetecting Early Breast Cancer with ImagingAria Alysis100% (1)
- SMJ 60 247Document6 pagesSMJ 60 247Chee Yung NgNo ratings yet
- Abdominoplasty With Customized Transverse Musculoaponeurotic PlicationsDocument9 pagesAbdominoplasty With Customized Transverse Musculoaponeurotic PlicationsМаратNo ratings yet
- Outcomes of Total Skin-sparing Mastectomy and Immediate ReconstructionDocument8 pagesOutcomes of Total Skin-sparing Mastectomy and Immediate ReconstructionAndreea PopescuNo ratings yet
- Laparoscopic FAGOTTY SCOREDocument12 pagesLaparoscopic FAGOTTY SCOREApriliza RalasatiNo ratings yet
- December 2017 1512132618 151Document3 pagesDecember 2017 1512132618 151D Tariq HNo ratings yet
- Asian GynecomastiaDocument5 pagesAsian GynecomastiaAngga Putra Kusuma KusumaNo ratings yet
- The Breast: SciencedirectDocument11 pagesThe Breast: SciencedirectYefry Onil Santana MarteNo ratings yet
- Review: Benjamin O Anderson, Riccardo Masetti, Melvin J SilversteinDocument13 pagesReview: Benjamin O Anderson, Riccardo Masetti, Melvin J SilversteinsanineseinNo ratings yet
- BreastReconstruction Review 2016Document9 pagesBreastReconstruction Review 2016Mohammed FaragNo ratings yet
- Breast Reconstruction: Rekonstrukcija DojkeDocument7 pagesBreast Reconstruction: Rekonstrukcija DojkeJuwita Dewi PratiwiNo ratings yet
- Treatment of Symptomatic Macromastia in A Breast Unit: Research Open AccessDocument6 pagesTreatment of Symptomatic Macromastia in A Breast Unit: Research Open AccessRamiro Castro ApoloNo ratings yet
- Oncoplastic Breast SurgeryDocument27 pagesOncoplastic Breast SurgeryReem Amr El-DafrawiNo ratings yet
- Brown 2014Document8 pagesBrown 2014nelly alconzNo ratings yet
- Annals of Medicine and Surgery: M. Riis TDocument13 pagesAnnals of Medicine and Surgery: M. Riis TJacob AlajyNo ratings yet
- Long-Term Complications and Patient-Reported Outcomes After Alloplastic Breast ReconstructionDocument7 pagesLong-Term Complications and Patient-Reported Outcomes After Alloplastic Breast Reconstruction郭竹瑩No ratings yet
- DOC-20230504-WA0039.Document4 pagesDOC-20230504-WA0039.Debraj SahaNo ratings yet
- Comparison of Ultrasound and Mammography For Early DiagnosisDocument8 pagesComparison of Ultrasound and Mammography For Early Diagnosishdh1224No ratings yet
- Consensus Guideline On Breast Cancer Lumpectomy MarginsDocument6 pagesConsensus Guideline On Breast Cancer Lumpectomy MarginsSubhamSarthakNo ratings yet
- INCISION PATTERNS IN BREAST ONCOPLASTIC SURGERYDocument26 pagesINCISION PATTERNS IN BREAST ONCOPLASTIC SURGERYccmcshh surgeryNo ratings yet
- 2014 179 0 Successful Treatment of Cervical Incompetence Using A Modified Laparoscopic Cervical Cerclage Technique A Cohort StudyDocument5 pages2014 179 0 Successful Treatment of Cervical Incompetence Using A Modified Laparoscopic Cervical Cerclage Technique A Cohort Studyalifiah nabillaNo ratings yet
- Oncologic Safety of Conservative Mastectomy in The Therapeutic SettingDocument10 pagesOncologic Safety of Conservative Mastectomy in The Therapeutic SettingIdaamsiyatiNo ratings yet
- 3D Mammometric Changes in The Treatment of Idiopathic Joban 2019Document9 pages3D Mammometric Changes in The Treatment of Idiopathic Joban 2019Wildan Satrio WemindraNo ratings yet
- New Trends in Breast Cancer Surgery: A Therapeutic Approach Increasingly Efficacy and Respectful of The PatientDocument8 pagesNew Trends in Breast Cancer Surgery: A Therapeutic Approach Increasingly Efficacy and Respectful of The PatientleonardoNo ratings yet
- Nipple Discharge 3Document3 pagesNipple Discharge 3Dima PathNo ratings yet
- Study of Fine Needle Aspiration Cytology of Breast Lump: Correlation of Cytologically Malignant Cases With Their Histological FindingsDocument5 pagesStudy of Fine Needle Aspiration Cytology of Breast Lump: Correlation of Cytologically Malignant Cases With Their Histological FindingsArvind Vashi AroraNo ratings yet
- Tiwari 2017Document3 pagesTiwari 2017Dewa OkaNo ratings yet
- Accuracy of Mammography and Ultrasound for Detecting Breast CancerDocument3 pagesAccuracy of Mammography and Ultrasound for Detecting Breast CancerBayuHernawanRahmatMuhariaNo ratings yet
- 1 s2.0 S2405632423000197 MainDocument11 pages1 s2.0 S2405632423000197 Mainsaros22568No ratings yet
- Will Surgery Be A Part of Breast Cancer Treatment in The FutureDocument5 pagesWill Surgery Be A Part of Breast Cancer Treatment in The FutureValentina MihaelaNo ratings yet
- Evaluation of Breast Masses Using Mammography and Sonography As First Line InvestigationsDocument3 pagesEvaluation of Breast Masses Using Mammography and Sonography As First Line InvestigationsNata SanjayaNo ratings yet
- Oncoplastic Breast Surgery Techniques for the General SurgeonFrom EverandOncoplastic Breast Surgery Techniques for the General SurgeonNo ratings yet
- Diverticular Disease Symptoms and Treatment AMBOSSDocument17 pagesDiverticular Disease Symptoms and Treatment AMBOSSMdacNo ratings yet
- Chronic Pancreatitis Symptoms, Causes & TreatmentDocument13 pagesChronic Pancreatitis Symptoms, Causes & TreatmentMdacNo ratings yet
- Intestinal Ischemia Guide - Causes, Symptoms & TreatmentDocument13 pagesIntestinal Ischemia Guide - Causes, Symptoms & TreatmentMdacNo ratings yet
- Gooi 2016Document6 pagesGooi 2016MdacNo ratings yet
- Acute Appendicitis - AMBOSSDocument28 pagesAcute Appendicitis - AMBOSSMdacNo ratings yet
- Practiceguidelines: Received: 4 May 2017 Accepted: 22 May 2017 DOI: 10.1002/hed.24866Document7 pagesPracticeguidelines: Received: 4 May 2017 Accepted: 22 May 2017 DOI: 10.1002/hed.24866MdacNo ratings yet
- Acute Cholangitis - AMBOSSDocument14 pagesAcute Cholangitis - AMBOSSMdacNo ratings yet
- Finding What Works in Health Care Standards For Systematic Reviews IOM 2011 PDFDocument341 pagesFinding What Works in Health Care Standards For Systematic Reviews IOM 2011 PDFVenance BasilNo ratings yet
- AHNS Series - Do You Know Your Guidelines? Lip CancerDocument5 pagesAHNS Series - Do You Know Your Guidelines? Lip CancerMdacNo ratings yet
- Bray Et al-2018-CA A Cancer Journal For Clinicians PDFDocument31 pagesBray Et al-2018-CA A Cancer Journal For Clinicians PDFSindhy DewiNo ratings yet
- Class. of Maxillectomy DefectsDocument10 pagesClass. of Maxillectomy DefectsJASPREETKAUR0410No ratings yet
- 2012 European Thyroid Association Guidelines For Metastatic Medullary Thyroid CancerDocument10 pages2012 European Thyroid Association Guidelines For Metastatic Medullary Thyroid CancerMdacNo ratings yet
- ASCO Guidelines Head and NeckDocument24 pagesASCO Guidelines Head and NeckMdacNo ratings yet
- Salvage Laryngectomy Following Organ-Preservation TherapyDocument8 pagesSalvage Laryngectomy Following Organ-Preservation TherapyMdacNo ratings yet
- Laryngectomee GuideDocument90 pagesLaryngectomee GuideMdacNo ratings yet
- Masa CervicalDocument9 pagesMasa CervicalMdacNo ratings yet
- Brown Et Al-2000-Head & NeckDocument10 pagesBrown Et Al-2000-Head & NeckMdacNo ratings yet
- (Cocos Nucifera) The Tree of Life: Coconut in Modern MedicineDocument6 pages(Cocos Nucifera) The Tree of Life: Coconut in Modern MedicineAdharsh ShankaranNo ratings yet
- Rare blistering skin condition linked to gluten intoleranceDocument2 pagesRare blistering skin condition linked to gluten intoleranceCharticha PatrisindryNo ratings yet
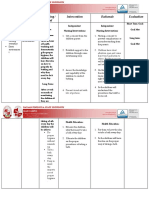
- NCP BathingDocument3 pagesNCP BathingNICOLE TOLENTINONo ratings yet
- My Courses: Home UGRD-PHYED6101-2113T Week 2: Health-Related Fitness Components Prelim Quiz 1Document4 pagesMy Courses: Home UGRD-PHYED6101-2113T Week 2: Health-Related Fitness Components Prelim Quiz 1Miguel Angelo GarciaNo ratings yet
- F o L K M e D I FinalDocument19 pagesF o L K M e D I FinalCk LamaNo ratings yet
- CG298 2016-05 Common Ground MagazineDocument32 pagesCG298 2016-05 Common Ground MagazineCommonGroundBCNo ratings yet
- Nutrition QuestionnaireDocument4 pagesNutrition QuestionnaireNitya Krishna100% (1)
- Eir - December2017 (1) Starup ListDocument2,738 pagesEir - December2017 (1) Starup ListNithin N Nayak0% (1)
- Mere WaliDocument7 pagesMere WaliMaliCk TaimoorNo ratings yet
- Knowledge and Practices of Mothers On Nigeria PDFDocument11 pagesKnowledge and Practices of Mothers On Nigeria PDFalfinNo ratings yet
- PSYCH 7 Course OutlineDocument4 pagesPSYCH 7 Course OutlineJM FranciscoNo ratings yet
- CV Template2Document3 pagesCV Template2rosemaryNo ratings yet
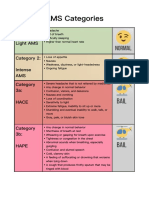
- AMS Symptoms and CategoriesDocument1 pageAMS Symptoms and CategoriesyyggvcNo ratings yet
- Fibroids (Uterine Myomas) - ClinicalKeyDocument25 pagesFibroids (Uterine Myomas) - ClinicalKeyfebri febiNo ratings yet
- Hsg245 - Investigating Accident & IncidentsDocument89 pagesHsg245 - Investigating Accident & IncidentsJohn MaynardNo ratings yet
- NCP-Deficient Fluid VolumeDocument1 pageNCP-Deficient Fluid Volumejanmichael8No ratings yet
- MukokelDocument3 pagesMukokeljulietNo ratings yet
- Guide To Competency Assessment Exam 2018Document14 pagesGuide To Competency Assessment Exam 2018Thenmolle RamanathanNo ratings yet
- CA 125II: Assay SummaryDocument14 pagesCA 125II: Assay SummaryThế TuyềnNo ratings yet
- Mefenamic Acid Drug StudyDocument1 pageMefenamic Acid Drug StudyAj GoNo ratings yet
- Intimidation: A Tool of Learning? Do We Learn Better Under The Gun?Document39 pagesIntimidation: A Tool of Learning? Do We Learn Better Under The Gun?Budi Iman SantosoNo ratings yet
- Managing Stress in GroupsDocument22 pagesManaging Stress in GroupsNguyen Vu Thuc Uyen (K17 QN)No ratings yet
- STUDENT KAP ON HIV/AIDSDocument22 pagesSTUDENT KAP ON HIV/AIDSbegosewNo ratings yet
- NBME Form 1 Step 2 ReviewDocument77 pagesNBME Form 1 Step 2 Reviewalex karevNo ratings yet
- Immunization Monitoring FormDocument4 pagesImmunization Monitoring FormDiler Singh100% (2)
- UW Water Resources and Innovation Conference 2015Document61 pagesUW Water Resources and Innovation Conference 2015LungisaniNo ratings yet
- Measuring Hospital Information System Readiness for E-Health Implementation Using HOT Fit MethodDocument5 pagesMeasuring Hospital Information System Readiness for E-Health Implementation Using HOT Fit Methodrm donorojoNo ratings yet