Professional Documents
Culture Documents
Rhodes Et Al 2023 Preexposure Prophylaxis Uptake Among Spanish Speaking Transgender Women A Randomized Controlled Trial
Uploaded by
Jessie BrionesOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Rhodes Et Al 2023 Preexposure Prophylaxis Uptake Among Spanish Speaking Transgender Women A Randomized Controlled Trial
Uploaded by
Jessie BrionesCopyright:
Available Formats
RESEARCH & ANALYSIS
Preexposure Prophylaxis Uptake
Among Spanish-Speaking Transgender
Women: A Randomized Controlled
Trial in North and South Carolina,
2019–2022
Scott D. Rhodes, PhD, MPH, Jorge Alonzo, JD, Lilli Mann-Jackson, MPH, Lucero Refugio Aviles, Amanda E. Tanner, PhD, MPH,
Carla A. Galindo, MPH, Patricia A. Bessler, MPH, Cari Courtenay-Quirk, PhD, Manuel Garcia, Ana D. Sucaldito, PhD, MPH,
Benjamin D. Smart, MD, MS, Tamar Goldenberg, PhD, MPH, and Beth A. Reboussin, PhD
Objectives. To evaluate Chicas Creando Acceso a la Salud (Girls Creating Access to Health; ChiCAS), a
Spanish-language, small-group intervention designed to increase preexposure prophylaxis (PrEP) use,
January 2024, Vol. 114, No. 1
consistent condom use, and medically supervised gender-affirming hormone therapy use among
Spanish-speaking transgender Latinas who have sex with men.
Methods. Participants were 144 HIV-negative Spanish-speaking transgender Latinas, aged 18 to
59 years, living in North and South Carolina. From July 2019 to July 2021, we screened, recruited, and
randomized them to the 2-session ChiCAS intervention or the delayed-intervention waitlist control.
Participants completed assessments at baseline and 6-month follow-up. Follow-up retention was 94.4%.
AJPH
Results. At follow-up, relative to control participants, ChiCAS participants reported increased PrEP use
(adjusted odds ratio [AOR] 5 4.64; 95% confidence interval [CI] 5 1.57, 13.7; P < .006). However, ChiCAS
participants did not report increased use of condoms or medically supervised gender-affirming
hormone therapy. ChiCAS participants reported increases in knowledge of HIV (P < .001), sexually
transmitted infections (P < .001), and gender-affirming hormone therapy (P 5 .01); PrEP awareness
(P < .001), knowledge (P < .001), and readiness (P < .001); condom use skills (P < .001); and community
attachment (P < .001).
Conclusions. The ChiCAS intervention was efficacious in increasing PrEP use among Spanish-speaking,
transgender Latinas in this trial. (Am J Public Health. 2024;114(1):68–78. https://doi.org/10.2105/
AJPH.2023.307444)
T
ransgender women are dispropor- Evidence-based strategies are needed name Descovy) as safe and effective
tionately affected by HIV. Current to prevent HIV transmission through in reducing the risk of HIV infection in
estimates indicate that about 14% of the use of preexposure prophylaxis adults and adolescents; injectable intra-
transgender women in the United (PrEP), a critical biomedical strategy to muscular extended-release cabotegra-
1 4,5
States are living with HIV, fewer than prevent new HIV infections. PrEP vir as PrEP is also now an option.6
2
half of whom know their status. Cer- clinical practice guidelines recommend However, awareness, knowledge, and
tain subpopulations of transgender daily oral combination tenofovir and use of PrEP are low among transgender
women are particularly affected by HIV, emtricitabine (brand name Truvada) women, particularly transgender
1,3
including transgender Latinas. or tenofovir and alafenamide (brand Latinas.5,7–11
68 Research Peer Reviewed Rhodes et al.
RESEARCH & ANALYSIS
Transgender Latinas also report little The US Centers for Disease Control service organizations, public health
use of medically supervised gender- and Prevention (CDC) has reiterated departments, and other community
12–14
affirming hormone therapy. Many calls for scaled-up HIV prevention strat- organizations; federal partners; and
report little access to formal health egies for transgender women, especial- academic researchers from multiple
care and thus may obtain hormones ly Latinas, given a recent finding that universities, and it developed, imple-
from nonmedical sources (e.g., Latine 35% of transgender Latinas tested pos- mented, and evaluated ChiCAS.11 The
[“Latine” uses a gender-neutral “e,” itive for HIV in a study in 7 major US partnership worked collaboratively with
which replaces the gendered endings cities.3 a 6-member community steering com-
“a” and “o” in “Latina” and “Latino” and is Our objective in this intervention trial mittee of transgender Latinas that met
similar to “Latinx.” This term is increas- was to test whether participants ran- monthly for the first year of the trial
ingly used within Latine LGBTQ1 (lesbi- domized to Chicas Creando Acceso a la and quarterly thereafter. The steering
an, gay, bisexual, transgender/-sexual, Salud (Girls Creating Access to Health; committee provided guidance to the
queer or questioning, and all subsects) ChiCAS) increased their use of PrEP, partnership on all aspects of the trial,
communities] grocers, the Internet, and condoms, and medically supervised including trial design (e.g., intervention
countries of origin) and take hormones gender-affirming hormone therapy and delayed-intervention wait list con-
without medical supervision; instead, compared with participants random- trol); recruitment and retention strate-
they may rely on one another for guid- ized to a delayed-intervention wait gies; inclusion of medically supervised
ance about dosage, administration, tim- list control. gender-affirming hormone therapy as
ing, and side effects.12,13 The use of an intervention focus; development of
AJPH
medically supervised gender-affirming METHODS the intervention logic model and inter-
hormone therapy is associated with vention activities, scripts, and materials,
January 2024, Vol. 114, No. 1
positive mental health outcomes and We used community-based participato- including video segments that role
behaviors (e.g., lower rates of suicidal ry research (CBPR) throughout all modeled seeking care; measurement;
ideation and drug and alcohol use), phases of this trial. CBPR is an effective and dissemination. They also helped
which also shape risk behaviors.13 approach to improving health and well- address emergent challenges, such as
Transgender Latinas using gender- being, aiding in disease prevention, and how to adapt the trial and intervention
affirming hormone therapy often priori- promoting health equity and reduce to the COVID-19 pandemic.9
tize the use of hormones over PrEP for disparities. CBPR blends the perspec-
HIV prevention because of fears that tives of community members, organiza- Intervention Development
taking PrEP will interfere with hormone tion representatives, and academic and Enhancement
use.15 Furthermore, medically super- partners to yield studies that have com-
vised gender-affirming hormone thera- munity buy-in and are authentic to how After obtaining CDC funding in 2016,
py can be costly and difficult to access community members engage, convene, our CBPR partnership and the trial
17,18
with no or insufficient health insurance; and interact. Compared with steering committee enhanced the local-
some transgender Latinas may obtain approaches that do not blend this array ly developed ChiCAS intervention, as
gender-affirming hormone therapy of perspectives, CBPR ensures higher described elsewhere,9,11 by developing
from less reliable sources or engage in recruitment and retention rates, more a logic model (Table A, available as a
sex work to pay for gender-affirming precise measurement, and more ac- supplement to the online version of
hormone therapy.13,16 ceptable data collection strategies. this article at http://www.ajph.org) and
Despite the disproportionate burden Moreover, data analysis and interpreta- an intervention logo; incorporating
of HIV among transgender Latinas, tion of findings may be more accurate. updated data on HIV burden and con-
no efficacious evidence-based or CBPR also contributes to the develop- text among transgender Latinas; pro-
evidence-informed intervention for ment of interventions that are more ducing a video segment outlining how
17,19
Spanish-speaking transgender Latinas likely to be efficacious. to access PrEP using transgender Lati-
is listed in the Compendium of Evidence- Our long-standing CBPR partnership na role models deciding to obtain PrEP
Based Interventions and Best Practices for is composed of local Latine community and then seeking care in a local clinic;
HIV Prevention (https://bit.ly/3SoQwjz). members; representatives from HIV refining intervention activities and
Research Peer Reviewed Rhodes et al. 69
RESEARCH & ANALYSIS
materials; outlining ways to access study (e.g., posters and flyers) at bars Because of the onset of the COVID-19
PrEP, including in the context of lacking and clubs, community colleges, Latine- pandemic, we adapted the trial as previ-
health insurance and being undocu- owned businesses, and community ously described.9 We gave participants
mented; and carefully scripting inter- events (e.g., LGBTQ1 pride events and cash as a token of appreciation for com-
vention delivery. We also reduced the Latine cultural festivals); through the pleting the baseline assessment ($30),
intervention from 4 to 2 sessions. use of social media and networking the 2 intervention sessions (before
20
Based on social cognitive theory Web sites, including apps for social and COVID: $40 per session), and the
and empowerment education,21 Chi- sexual networking used by or designed 6-month follow-up assessment ($40).
CAS is designed to increase PrEP use, for members of the LGBTQ1 communi- Before the pandemic, sessions were in
consistent condom use, and use of ty (e.g., Facebook and Grindr); and by person and dinner was served at each
medically supervised gender-affirming word of mouth whereby study partici- session. After the onset of the pandemic,
hormone therapy.11 The intervention pants invited friends to participate. we implemented ChiCAS virtually via
addresses critical behavioral determi- Study participants were eligible if videoconferencing and dinner was not
nants, which have been found to be as- they self-identified as a transgender served. Each participant also received a
sociated with HIV prevention behaviors woman or reported having been assigned T-shirt and a bag with the project logo.
among transgender Latinas.11,13,22,23 male sex at birth and self-identifying as We provided a graduation ceremony for
These determinants include knowledge female, self-identified as Hispanic/Latina, participants after they completed all Chi-
of HIV and sexually transmitted infec- were aged 18 years or older, reported CAS sessions, and participants received
tions (STIs) and their modes of trans- sex with at least 1 man in the past 6 framed certificates of completion.
January 2024, Vol. 114, No. 1
mission and prevention strategies, months, were HIV-negative (based on Three interventionists delivered the
knowledge of PrEP and medically su- self-report and verified by HIV testing ChiCAS intervention: a native Spanish-
pervised gender-affirming hormone during the consent process), spoke flu- speaking transgender Latina woman,
therapy and of eligibility for accessing ent Spanish, and provided informed con- a native Spanish-speaking cisgender
various services and resources, per- sent. Persons who had participated in Latino gay man, and a fluent Spanish-
ceived access to available health care any other HIV prevention intervention in speaking cisgender White woman.
services and self-efficacy to overcome the past 12 months were ineligible. The These interventionists were experi-
AJPH
access barriers, communication skills study team referred and linked potential enced in implementing HIV prevention
with providers and sexual partners, participants who tested positive for HIV and PrEP promotion interventions in
sociocultural context (e.g., internalized during screening to HIV care. Linkage in- LGBTQ1 communities and were trained
transphobia), and relationships and cluded helping these individuals make in ChiCAS implementation. Before the
sense of community among transgen- appointments for confirmatory HIV tests COVID-19 pandemic, the interventionists
der Latinas. We did not provide PrEP in and subsequent HIV care and accompa- delivered ChiCAS in person to partici-
this intervention; rather, we built the nying them to initial appointments if pants during 2 sessions lasting 4 hours
skills among participants to seek and desired. each on consecutive Sunday evenings in
successfully obtain PrEP in the commu- We recruited and enrolled 144 trans- safe and conveniently located communi-
nity. Building community capacity to re- gender Latinas to the study in 10 waves ty settings. After the onset of the pan-
duce health inequities is an important of approximately 14 participants per demic, we adapted the 2 sessions to last
strategy in our CBPR partnership. wave. Participants completed written 2 hours each via Zoom, given the chal-
informed consent and a baseline as- lenges of maintaining attention via video-
Study Design sessment, and a block randomization conferencing. Additional adaptations
scheme generated with SAS version 9.3 made to the ChiCAS intervention and
We used a 2-group, randomized, inter- (SAS Institute, Cary, NC) assigned them study delivery are described elsewhere.9
vention wait list control design with a to ChiCAS (n 5 72) or the delayed- Raters provided quality assurance
1 to 1 allocation ratio to evaluate the ef- intervention wait list control (n 5 72; during intervention delivery; they
ficacy of ChiCAS. From July 2019 to July Figure 1). Half of the sample was attended each session and documen-
2021, we recruited participants recruited and participated in the interven- ted whether activities were implemen-
by distributing information about the tion before the onset of the pandemic. ted with fidelity.
70 Research Peer Reviewed Rhodes et al.
RESEARCH & ANALYSIS
Community-Based Participatory Research Partnership
Community Scientific
research research
partners Study team
partners
Intervention
enhancement
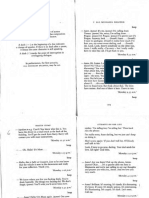
Screen Ineligible:
(n = 162) Did not meet inclusion criteria (n = 1)
Baseline assessment
(n = 161)
Not randomized:
Randomization Wave not implemented because of NC
(n = 144) COVID-19 stay-at-home order (n = 5)
Not available/schedule conflict (n = 11)
AJPH
ChiCAS Intervention Delayed-Intervention
January 2024, Vol. 114, No. 1
(n = 72; Control
in-person = 35, virtual = 37) (n = 72)
6-month follow-up 6-month follow-up
(n = 68; 94.4% retention) (n = 68; 94.4% retention)
FIGURE 1— Schematic of the Research Design to Test the ChiCAS Intervention for HIV-Negative Spanish-Speaking
Transgender Latinas: North and South Carolina, 2019–2022
Note. ChiCAS 5 Chicas Creando Acceso a la Salud (Girls Creating Access to Health).
Outcome Measures therapy. We defined consistent con- knowledge with true–false items. A
dom use as using condoms during sample gender-affirming hormone
We collected all outcome measures at every instance of insertive anal or re- therapy knowledge item included “Only
baseline upon enrollment and then ceptive anal or vaginal sex with men a medical doctor or nurse can deter-
again at a follow-up. We collected out- and insertive vaginal or anal sex with mine the appropriate hormone therapy
comes via assessments that a trained women in the 30 days before the base- and dose.”
interviewer administered in Spanish. line and 6-month follow-up assessments. We assessed awareness and knowl-
PrEP use was a primary outcome be- We measured the use of medically super- edge of PrEP and readiness to take
cause of its demonstrated effectiveness vised gender-affirming hormone therapy PrEP. We assessed PrEP awareness us-
at reducing the risk of sexual HIV trans- by asking whether participants were cur- ing the scale item “On a scale from 0 to
mission. We assessed current PrEP use rently using it and, if so, where they 10, with 0 being knowing nothing at all
by asking participants whether they obtained the gender-affirming hormones. and 10 being knowing a lot, how much
were currently using PrEP. We assessed We also measured changes in deter- would you say you know about PrEP?”
2 additional outcomes: consistent con- minants that ChiCAS was designed to Sample PrEP knowledge items included
dom use and current use of medically influence. We measured HIV,24 STI,25 “PrEP can reduce the chances of getting
supervised gender-affirming hormone and gender-affirming hormone therapy HIV among those without HIV” and
Research Peer Reviewed Rhodes et al. 71
RESEARCH & ANALYSIS
“PrEP interacts with gender-affirming concerns I have even when he or she intervention group may exhibit more
hormones that some transgender per- does not ask.”32 similar patterns of PrEP use, condom
sons take or plan to take.” We assessed We also measured barriers to health use, and use of gender-affirming hor-
PrEP readiness using the item “How like- care.33 Sample barriers to which partici- mone therapy at 6-month follow-up
ly is it that you’d use PrEP?” Response pants were asked to respond included, compared with participants in other
options ranged from “not at all likely” (1) “You didn’t have transportation” and study waves. We adjusted models for
to “extremely likely” (5). “You felt like you would be treated age, education, employment, country of
We used an adapted version of the poorly.” We measured barriers using origin, and whether participants partici-
Condom-Use Skills Checklist to assess yes–no responses and yes responses pated in in-person or virtual implemen-
knowledge about correct condom added together. tation to obtain adjusted odds ratios
25 25,26
use and condom use intentions. We completed reverse coding as (AORs) and computed the 95% confi-
We used the 26-item Internalized warranted, and higher scores for each dence intervals (CIs) and corresponding
27
Transphobia Scale to measure inter- determinant indicated higher levels of P values. We fit models using PROC
nalized transphobia, the 12-item Multi- that determinant. GLIMMIX in SAS.
28
group Ethnic Identity Measure to In our secondary analysis, we used the
measure ethnic group pride, and an Statistical Analyses t test to assess changes in determinants
adapted 18-item version of the Index of that the ChiCAS intervention addressed.
Sojourner Social Support Scale29 to We used an intention-to-treat protocol We included the same sociodemo-
measure social support. We measured to analyze participants’ outcomes rela- graphic factors in these analyses that we
January 2024, Vol. 114, No. 1
community attachment using an tive to their assigned intervention included in the final outcome models.
adapted 3-item scale30 consisting of group, irrespective of the number of For each scale, we replaced missing
“Please indicate how much you feel a sessions they attended.34 At baseline, scale items with the person-mean im-
part of or connected to . . .” “. . . the we calculated descriptive statistics to puted value for each specific scale if
transgender community,” “. . . the summarize sociodemographic charac- 20% or less of scale items responses
Hispanic/Latino community,” and “. . . teristics of intervention and delayed- were missing. If more than 20% was
the Hispanic/Latino transgender com- intervention wait list control participants. missing, we considered that scale miss-
AJPH
munity.” Response options ranged from We assessed differences between the ing and did not use it in our analyses.
“not at all” (0) to “to a great extent” (5). groups at baseline using the Student For each model, we calculated adjusted
We measured medical mistrust using t test for continuous variables and x2 means and SEs and differences of ad-
a scale that we have successfully used for categorical variables. justed means and their corresponding
previously with Spanish-speaking popu- Our primary data analyses to evalu- P values. We estimated all models in the
lations.31 Participants ranked on a scale ate ChiCAS efficacy compared propor- context of multivariable random effects
from strongly disagree (1) to strongly tions of PrEP use, consistent condom linear regression modeling using PROC
agree (4) how much they agree with use, and use of medically supervised MIXED in SAS. We performed all analyses
5 statements, including “Sometimes gender-affirming hormone therapy by using SAS/STAT version 9.3.
doctors care more about what is conve- intervention and delayed-intervention
nient for them than about their patients’ wait list control participants at the RESULTS
medical needs.” We also measured pa- 6-month postintervention follow-up
tient activation (i.e., provider communi- while adjusting for baseline rates. The average age of the 144 study parti-
cation skills and health management Statistical analysis used multivariable cipants was 33.1 years (SD 5 9.4), nearly
efficacy) using an adapted version of the random effects logistic regression 50% had less than a high school educa-
short form of the Patient Activation Mea- modeling that adjusted for potential tion or general equivalency diploma
sure. Participants indicated on a scale clustering in intervention groups by equivalent, 65% were employed year
from strongly disagree (1) to strongly including a random effect for the inter- round, and 80.1% reported earning
agree (4) how much they agreed with vention group.35 This adjustment less than $2000 per month. The majori-
13 statements, including “I am confi- accounted for the possibility that parti- ty of participants were foreign born
dent I can tell my health care provider cipants in the same study wave and (88%). Seventy percent of the
72 Research Peer Reviewed Rhodes et al.
RESEARCH & ANALYSIS
participants reported speaking only or Most participants (69.4%) assigned to Intervention Effects
mostly Spanish. Foreign-born partici- the ChiCAS intervention completed
pants had been living in the United both of their assigned intervention ses- At 6-month follow-up, ChiCAS partici-
States for a mean of 16.4 years. Partici- sions; however, attendance rates varied pants’ reports of current PrEP use sig-
pants self-identified as female (98%) or by mode of intervention delivery. Virtual nificantly increased, from 10.6% at
transgender (2%). Sexual orientation was implementation had a higher rate of re- baseline to 31.8% (P 5 .002). PrEP use
reported as heterosexual (81%), bisexual tention, with 73.0% (27 of 37) attending among delayed-intervention wait list
(10%), gay (6%), and “something else” both sessions; in-person implementation control participants did not significantly
(3%). Three percent of participants had a retention rate of 65.7% (23 of 35) change (7.5% at baseline vs 13.4% at
reported sex with women in addition to attending both sessions. 6-month follow-up; P 5 .23). Adjusting
men within the past 6 months. There Overall retention for 6-month follow- for age, education, employment, coun-
were no significant differences between up assessments across intervention and try of origin, and mode of intervention
sociodemographic characteristics of delayed-intervention wait list control par- delivery (i.e., in person or virtual) at
intervention and control participants ticipants was 94.4%. We delivered the in- 6-month follow-up, ChiCAS participants
(Table 1). tervention with a high degree of fidelity. were 4.64 (95% CI 5 1.57, 13.7) times as
TABLE 1— Characteristics of Participants in the ChiCAS Intervention Trial by Intervention Group at
Baseline: North and South Carolina, 2019–2022
AJPH
Delayed-
January 2024, Vol. 114, No. 1
Intervention
Intervention Wait List Group,
Group, No. (%) or No. (%)
Characteristica Mean 6SD or Mean 6SD) Pb
Age, y (n 5 143) 33.0 69.4 33.2 69.4 .93
Years living in US among foreign born (n 5 122) 15.9 68.5 17.0 68.9 .54
Country of origin (n 5 142) .48
Mexico 44 (62.0) 49 (69.0)
United States 8 (11.3) 9 (12.7)
Other 19 (26.8) 13 (18.3)
Education (n 5 143) .09
Less than high school education or general equivalency diploma equivalent 32 (45.1) 39 (54.2)
High school or general equivalency diploma 20 (28.2) 18 (25.0)
Some college 16 (22.5) 7 (9.7)
College 3 (4.2) 8 (11.1)
Employment (n 5 143) .37
Employed year-round 49 (69.0) 44 (61.1)
Seasonal 9 (12.7) 7 (9.7)
Unemployed 10 (14.1) 13 (18.1)
Disabled/not working 3 (4.2) 8 (11.1)
Monthly income, $ (n 5 141)
None 12 (16.9) 18 (25.7) .43
< 1000 16 (22.5) 10 (14.3)
1000–1999 28 (39.4) 29 (41.4)
≥ 2000 15 (21.1) 13 (18.6)
Note. ChiCAS 5 Chicas Creando Acceso a la Salud (Girls Creating Access to Health).
a
Number for each characteristic may not equal 144 because of missing data.
b
P value from t-test statistics for means and x2 statistics for %.
Research Peer Reviewed Rhodes et al. 73
RESEARCH & ANALYSIS
TABLE 2— Reported Use of Preexposure Prophylaxis (PrEP), Condoms, and Medically Supervised
Hormone Therapy Among ChiCAS Participants at Baseline and Follow-up by Intervention Group: North
and South Carolina, 2019–2022
Intervention Intervention
Effect Effect
Intervention Delayed Intervention Unadjusted Adjusteda
Baseline, Follow-Up, Unadjusted Baseline, Follow-Up, Unadjusted
Variable No. (%) No. (%) Pb No. (%) No. (%) P valueb OR (95% CI) AOR (95% CI)
Current PrEP usec 7 (10.6) 21 (31.8) .002 5 (7.5) 9 (13.4) .23 3.29 (1.24, 8.75) 4.64 (1.57, 13.7)
Past 30-d consistent 20 (40.8) 24 (48.9) .13 17 (38.6) 23 (52.3) .1 0.81 (0.32, 2.04) 0.76 (0.28, 2.09)
condom use
among those
reporting sexd
Current use of 25 (36.8) 28 (41.2) .67 25 (39.1) 27 (42.2) .48 1.04 (0.40, 2.74) 1.29 (0.46, 3.61)
medically
supervised
gender-affirming
hormone
therapye
Note. AOR 5 adjusted odds ratio; ChiCAS 5 Chicas Creando Acceso a la Salud (Girls Creating Access to Health); CI 5 confidence interval; OR 5 odds ratio;
PrEP 5 preexposure prophylaxis. Study sample size was n 5 144.
a
Adjusted for baseline, age, education, employment, country of birth, and mode of delivery (in person vs virtual).
January 2024, Vol. 114, No. 1
b
Test of within-group differences between baseline and follow-up.
c
Intervention n 5 66; delayed-intervention n 5 67 (owing to missing data).
d
Participants reporting sex in past 30 d, intervention (n 5 49) and delayed-intervention(n 5 44).
e
Intervention n 5 68; delayed-intervention n 5 64 (owing to missing data).
likely as delayed-intervention wait list and community attachment (P < .001). We found that ChiCAS participants
control participants to report PrEP use There were no statistically significant were more than 4 times as likely as
(P 5 .006). Adjusting for age, education, differences between ChiCAS and delayed-intervention wait list control
AJPH
employment, country of origin, and delayed-intervention wait list control participants to report current PrEP use
mode of intervention delivery, ChiCAS participants in reported internalized at 6-month follow-up. We did not iden-
participants’ reports of past 30-day con- transphobia, ethnic group pride, social tify significant changes in the 2 other
dom use and current use of medically support, medical mistrust, patient acti- study outcomes that the intervention
supervised gender-affirming hormone vation, or barriers to health care. was designed to affect: consistent con-
therapy were not significantly different dom use and medically supervised
at 6-month follow-up (AOR 5 0.76; 95% gender-affirming hormone therapy.
CI 5 0.28, 2.09 and AOR 5 1.3; 95% DISCUSSION There are a number of potential expla-
CI 5 0.46, 3.61, respectively; Table 2). nations for this. First, the ChiCAS trial
We observed marked differences in Transgender Latinas in the United States was powered on PrEP uptake.11 Fur-
8 behavioral determinants that the are particularly vulnerable to HIV infec- thermore, the onset of the COVID-19
intervention targeted (Table 3). Com- tion, and their PrEP and condom use pandemic about halfway through the
pared with delayed-intervention wait remain low. However, there are no effi- trial required us to abbreviate the inter-
list control participants at 6-month cacious HIV prevention interventions for vention for virtual implementation to
follow-up, ChiCAS participants reported transgender Latinas currently listed in continue the trial safely, as previously
increases in knowledge of HIV (P < .001), the CDC Compendium of Evidence-Based described.9 These abbreviations and
STI (P < .001), and medically supervised Interventions and Best Practices for HIV Pre- the absence of in-person interactions
gender-affirming hormone therapy vention (https://bit.ly/45SSNqp), and the during some activities, such as the sex-
(P < .01); PrEP awareness (P < .001), CDC has called for an increased focus ual partner condom use negotiation ac-
knowledge (P < .001), and readiness on HIV prevention among transgender tivities, may have affected intervention
(P < .001); condom use skills (P < .001); women, especially Latinas. efficacy, and the complexities
74 Research Peer Reviewed Rhodes et al.
RESEARCH & ANALYSIS
TABLE 3— Adjusted Means and SE of Behavioral Determinants Among ChiCAS Participants at 6-Month
Follow-Up by Intervention Group: North and South Carolina, 2019–2022
Adjusted Means and SEs at 6-Mo Follow-Upa
Difference of
Adjusted Adjusted Degree of
Determinant Mean 6SE Mean 6SE Freedom t value P
HIV knowledge 3.7 60.48 114 7.67 < .001
Intervention group 16.7 60.46
Control group 13.0 60.46
STI knowledge 2.3 60.41 114 5.61 < .001
Intervention group 12.8 60.47
Control Group 10.5 60.47
Gender-affirming hormone therapy knowledge 0.82 60.31 114 2.62 .01
Intervention group 8.3 60.31
Control group 7.4 60.31
PrEP awareness 2.2 60.37 113 5.81 < .001
Intervention group 7.8 60.42
Control group 5.6 60.42
PrEP knowledge 3.0 60.42 114 6.98 < .001
AJPH
Intervention group 10.7 60.40
Control group 7.7 60.40
January 2024, Vol. 114, No. 1
PrEP use readiness 1.0 60.27 114 3.71 < .001
Intervention group 4.2 60.26
Control group 3.1 60.26
Condom use skills 0.76 60.16 114 4.58 < .001
Intervention group 16.1 60.18
Control group 15.4 60.18
Condom use intentions 0.18 60.17 111 1.05 .29
Intervention group 4.2 60.18
Control group 4.0 60.18
Internalized transphobia 1.5 62.74 113 0.54 .59
Intervention group 62.2 62.56
Control group 60.7 62.52
Multiethnic identity measure/ethnic group pride 0.88 60.92 114 0.95 .34
Intervention group 37.0 60.92
Control group 36.1 60.94
Social support 4.2 62.41 114 1.76 .08
Intervention group 34.8 63.12
Control group 30.6 63.13
Community attachment 0.82 60.21 110 3.86 < .001
Intervention group 3.8 60.20
Control group 3.0 60.20
Medical mistrust 20.53 60.44 113 21.21 .23
Intervention group 16.3 60.44
Control group 16.9 60.44
Patient activation 20.98 61.12 113 20.88 .38
Intervention group 43.1 61.05
Continued
Research Peer Reviewed Rhodes et al. 75
RESEARCH & ANALYSIS
TABLE 3— Continued
Adjusted Means and SEs at 6-Mo Follow-Upa
Difference of
Adjusted Adjusted Degree of
Determinant Mean 6SE Mean 6SE Freedom t value P
Control group 44.1 61.06
Barriers to health care 20.33 60.38 113 20.86 .39
Intervention group 0.7 60.55
Control group 1.1 60.6
Note. ChiCAS 5 Chicas Creando Acceso a la Salud (Girls Creating Access to Health); PrEP 5 preexposure prophylaxis; STI 5 sexually transmitted infection.
a
Adjusted means and SEs were based on multivariable random effect linear mixed models with covariates of age, education attainment, employment,
model of delivery, and country of origin with corresponding baseline measure.
associated with condom use negotia- participants and obtained their con- gender-affirming hormone therapy at
tion and initiation may require addition- sent, implemented the intervention, baseline and follow-up were able to pro-
al skills-building support. Furthermore, delivered intervention materials, and vide authenticating details, including the
not all transgender Latinas want to use contacted participants for follow-up provider and clinic where they obtained
gender-affirming hormones. assessments reflected the study popu- their prescriptions and the pharmacy
It is noteworthy that we observed fa- where they filled their prescription.
January 2024, Vol. 114, No. 1
lation (transgender Latinas) or closely
vorable changes in 8 critical behavioral aligned with the population (LGBTQ1 The lack of significant between-group
determinants that the ChiCAS interven- community), native Spanish speakers, differences in some of the determi-
tion was designed to affect; specifically, and were skilled in trust and rapport nants that we designed the ChiCAS in-
ChiCAS participants had increased building. tervention to affect and that have been
knowledge of HIV, STIs, and medically associated with HIV prevention beha-
supervised gender-affirming hormone Limitations viors suggests a need to reexamine
AJPH
therapy; PrEP awareness and knowl- how the intervention addresses these
edge; readiness to use PrEP; condom Although we had planned to verify use determinants. Finally, although we did
use skills; and community attachment. of PrEP and medically supervised control for mode of delivery in our pri-
Furthermore, our study had a very high gender-affirming hormone therapy mary outcome analyses, we were un-
retention rate: 94.4% of all participants through review of medical records, the able to test the intervention by mode of
completed 6-month follow-up assess- onset of the COVID-19 pandemic made delivery (i.e., in person vs virtual) given
ments. This may be attributable to the this task untenable given that many the small sample size.
substantial engagement of transgender clinics were understaffed because of
Latinas at all stages of developing inter- the pandemic. Members of our part- Conclusions
vention content. ChiCAS was developed nership, some of whom represented
to reflect the real-world experiences health departments and clinics, advised Important gaps exist in the current in-
and priorities of transgender Latinas. us not to place additional burdens on tervention arsenal for reducing HIV risk
Each intervention module and activity already stressed facilities by conducting among sexual and gender minority
was designed to meet Spanish- medical record reviews. Therefore, we populations, and nowhere is there a
speaking transgender Latinas’ relied on self-reported use of PrEP and greater need than among transgender
expressed needs and was presented in medically supervised gender-affirming Latinas. Thus, ChiCAS offers an urgently
a manner that was highly engaging and hormone therapy; however, self-report needed resource to prevent HIV among
interactive, during both in-person and has been found to be reliable if con- Spanish-speaking transgender Latinas
virtual implementation delivery. Fur- ducted carefully.36 In post hoc analyses, who have sex with men. The intervention
thermore, many members of the study 100% of participants who reported was efficacious, significantly increasing
team who screened and recruited use of PrEP and medically supervised PrEP use in this trial. It also may serve as
76 Research Peer Reviewed Rhodes et al.
RESEARCH & ANALYSIS
a foundation for interventions designed participant recruitment and retention and data guidelines-2021.pdf. Accessed November 1,
collection. A. E. Tanner assisted in study implemen- 2023.
to increase PrEP use among other trans- tation and data analysis. C. A. Galindo, P. A. Bessler, 7. Holder CL, Perez-Gilbe HR, Fajardo FJ, Garcia S,
gender populations. and C. Courtenay-Quirk oversaw the study. B. A. Cyrus E. Disparities of HIV risk and PrEP use
Reboussin participated in study development and among transgender women of color in South
oversaw data analyses. All authors participated in Florida. J Natl Med Assoc. 2019;111(6):625–632.
ABOUT THE AUTHORS https://doi.org/10.1016/j.jnma.2019.08.001
article preparation.
Scott D. Rhodes, Jorge Alonzo, Lilli Mann-Jackson, 8. Collier KL, Colarossi LG, Hazel DS, Watson K,
and Manuel Garcia are with the Department of Wyatt GE. Healing our women for transgender
Social Sciences and Health Policy, Wake Forest
ACKNOWLEDGMENTS women: adaptation, acceptability, and pilot test-
University School of Medicine, Winston-Salem, Funding for the ChiCAS trial was provided by the ing. AIDS Educ Prev. 2015;27(5):418–431. https://
doi.org/10.1521/aeap.2015.27.5.418
NC. At trial initiation, Lucero Refugio Aviles was US Centers for Disease Control and Prevention
with the Triad Health Project, Greensboro, NC; (CDC; cooperative agreement U01PS005137). 9. Rhodes SD, Tanner AE, Mann-Jackson L, et al.
Note. The findings and conclusions in this arti- Adapting a group-level PrEP promotion interven-
she completed the study while at the Department
tion trial for transgender Latinas during the
of Social Sciences and Health Policy, Wake Forest cle are those of the authors and do not necessar-
COVID-19 pandemic. AIDS Educ Prev. 2022;34(6):
University School of Medicine. Amanda E. Tanner ily represent the official position of the CDC. 481–495. https://doi.org/10.1521/aeap.2022.34.
and Tamar Goldenberg are with the Department 6.481
of Public Health Education, University of North
CONFLICTS OF INTEREST 10. Poteat T, Wirtz A, Malik M, et al. A gap between
Carolina, Greensboro. Carla A. Galindo, Patricia A. willingness and uptake: findings from mixed
Bessler, and Cari Courtenay-Quirk are with the The authors have no conflicts of interest to methods research on HIV prevention among
US Centers for Disease Control and Prevention, declare. Black and Latina transgender women. J Acquir
Atlanta, GA. Ana D. Sucaldito is with the Clinical Immune Defic Syndr. 2019;82(2):131–140. https://
and Translational Science Institute, Wake Forest doi.org/10.1097/QAI.0000000000002112
HUMAN PARTICIPANT
University School of Medicine. Benjamin D. Smart 11. Rhodes SD, Kuhns LM, Alexander J, et al. Evaluat-
is with the Karolinska Institutet, Stockholm,
PROTECTION ing homegrown interventions to promote PrEP
Sweden. Beth A. Reboussin is with the Depart- Human participant oversight was provided by the among racially/ethnically diverse transgender
ment of Biostatistics and Data Sciences, Wake institutional review board of Wake Forest Univer- women in the United States: a unique CDC initia-
tive. AIDS Educ Prev. 2021;33(4):345–360. https://
Forest University School of Medicine. sity School of Medicine. Written informed consent
AJPH
doi.org/10.1521/aeap.2021.33.4.345
was obtained from each participant.
12. Rhodes SD, Alonzo J, Mann L, et al. Using photo-
CORRESPONDENCE voice, Latina transgender women identify priori-
January 2024, Vol. 114, No. 1
Correspondence should be sent to Scott D. ties in a new immigrant-destination state. Int J
REFERENCES Transgend. 2015;16(2):80–96. https://doi.org/10.
Rhodes, Department of Social Sciences and
Health Policy, Wake Forest School of Medicine, 1. Becasen JS, Denard CL, Mullins MM, Higa DH, 1080/15532739.2015.1075928
Division of Public Health Sciences, Medical Center Sipe TA. Estimating the prevalence of HIV and 13. Smart BD, Mann-Jackson L, Alonzo J, et al. Trans-
sexual behaviors among the US transgender gender women of color in the US South: a quali-
Blvd, Winston-Salem, NC 27157-1063 (e-mail:
population: a systematic review and meta-analysis, tative study of social determinants of health and
srhodes@wakehealth.edu). Reprints can be
2006–2017. Am J Public Health. 2019;109(1):e1–e8. healthcare perspectives. Int J Transgend.
ordered at http://www.ajph.org by clicking the https://doi.org/10.2105/AJPH.2018.304727 2020;23(1–2):164–177. https://doi.org/10.1080/
“Reprints” link. 26895269.2020.1848691
2. Habarta N, Wang G, Mulatu MS, Larish N. HIV
testing by transgender status at Centers for Dis- 14. Rivera AV, Lopez JM, Braunstein SL. Exploring the
PUBLICATION INFORMATION ease Control and Prevention–funded sites in the association between gender affirmation and
Full Citation: Rhodes SD, Alonzo J, Mann-Jackson L, United States, Puerto Rico, and US Virgin Islands, PrEP use among transgender women in New
2009–2011. Am J Public Health. 2015;105(9): York City. AIDS Behav. 2023;27(5):1523–1530.
et al. Preexposure prophylaxis uptake among
1917–1925. https://doi.org/10.2105/AJPH.2015. https://doi.org/10.1007/s10461-022-03944-7
Spanish-speaking transgender women: a random-
302659 15. Sevelius JM, Patouhas E, Keatley JG, Johnson MO.
ized controlled trial in North and South Carolina,
3. Centers for Disease Control and Prevention. HIV Barriers and facilitators to engagement and re-
2019–2022. Am J Public Health. 2024;114(1):68–78.
infection, risk, prevention, and testing behaviors tention in care among transgender women living
Acceptance Date: September 3, 2023. among transgender women: National HIV Behav- with human immunodeficiency virus. Ann Behav
DOI: https://doi.org/10.2105/AJPH.2023.307444 ioral Surveillance, 7 US cities, 2019–2020. Avail- Med. 2014;47(1):5–16. https://doi.org/10.1007/
able at: https://www.cdc.gov/hiv/pdf/library/ s12160-013-9565-8
reports/surveillance/cdc-hiv-surveillance-special- 16. Sevelius JM. Gender affirmation: a framework for
CONTRIBUTORS report-number-27.pdf. Accessed November 1, conceptualizing risk behavior among transgen-
S. D. Rhodes coconceptualized and supervised 2023. der women of color. Sex Roles. 2013;68(11–12):
the trial in partnership with colleagues from Triad 4. Sullivan PS, Mena L, Elopre L, Siegler AJ. Imple- 675–689. https://doi.org/10.1007/s11199-012-
Health Project, participated in intervention devel- mentation strategies to increase PrEP uptake 0216-5
opment and refinement; oversaw implementa- in the South. Curr HIV/AIDS Rep. 2019;16(4): 17. Wallerstein N, Duran B. Community-based partic-
tion; collected, analyzed, and interpreted the 259–269. https://doi.org/10.1007/s11904-019- ipatory research contributions to intervention re-
00447-4 search: the intersection of science and practice
data; and led article preparation. S. D. Rhodes,
5. Rhodes SD, Alonzo J, Mann-Jackson L, et al. A to improve health equity. Am J Public Health.
J. Alonzo, L. Refugio Aviles, and B. A. Reboussin
peer navigation intervention to prevent HIV 2010;100(suppl 1):S40–S46. https://doi.org/10.
participated in intervention implementation.
among mixed immigrant status Latinx GBMSM 2105/AJPH.2009.184036
J. Alonzo supervised data collection. J. Alonzo and
and transgender women in the United States: 18. Israel BA, Schulz AJ, Parker EA, Becker AB. Review
L. Refugio Aviles refined the intervention.
outcomes, perspectives and implications for of community-based research: assessing part-
J. Alonzo, L. Mann-Jackson, L. Refugio Aviles, PrEP uptake. Health Educ Res. 2020;35(3): nership approaches to improve public health.
C. A. Galindo, P. A. Bessler, C. Courtenay-Quirk, 165–178. https://doi.org/10.1093/her/cyaa010 Annu Rev Public Health. 1998;19:173–202. https://
M. Garcia, A. D. Sucaldito, B. D. Smart, T. Goldenberg, doi.org/10.1146/annurev.publhealth.19.1.173
6. Centers for Disease Control and Prevention. Pre-
and B. A. Reboussin assisted with data interpretation. exposure Prophylaxis for the Prevention of HIV 19. Rhodes SD, Mann L, Alonzo J, et al. CBPR to pre-
L. Mann-Jackson oversaw intervention implementa- Infection in the United States—2021 Update. A Clini- vent HIV within ethnic, sexual, and gender minor-
tion and participant randomization and tracking. cal Practice Guideline. 2021. Available at: https:// ity communities: successes with long-term
L. Refugio Aviles and M. Garcia assisted in www.cdc.gov/hiv/pdf/risk/prep/cdc-hiv-prep- sustainability. In: Rhodes SD, ed. Innovations in
Research Peer Reviewed Rhodes et al. 77
RESEARCH & ANALYSIS
HIV Prevention Research and Practice Through immigrant Latino men who utilize formal health-
Community Engagement. New York, NY: Springer; care services in rural North Carolina: baseline
2014:135–160. https://doi.org/10.1007/978-1- findings from the HoMBReS Study. J Natl Med
4939-0900-1_7 Assoc. 2008;100(10):1177–1185.
20. Bandura A. Social Foundations of Thought and 34. Friedman LM, Furberg CD, DeMets DL. Funda-
Action: A Social Cognitive Theory. Englewood Cliffs, mentals of Clinical Trials. 3rd ed. New York, NY:
NJ: Prentice-Hall; 1986. Springer-Verlag; 1998. https://doi.org/10.1007/
21. Freire P. Education for Critical Consciousness. New 978-1-4757-2915-3
York, NY: Seabury Press; 1973. 35. Wolfinger R, O’Connell M. Generalized linear
22. Neumann MS, Finlayson TJ, Pitts NL, Keatley J. mixed models: a pseudo-likelihood approach.
Comprehensive HIV prevention for transgender J Stat Comput Simul. 1993;48(3–4):233–243.
persons. Am J Public Health. 2017;107(2): https://doi.org/10.1080/00949659308811554
207–212. https://doi.org/10.2105/AJPH.2016. 36. Qasmieh S, Nash D, Gandhi M, et al. Self-reported
303509 use of HIV preexposure prophylaxis is highly accu-
23. Mizuno Y, Koenig LJ, Wilkes AL, et al. Utilization rate among sexual health clinic patients in New
of HIV prevention, care, and treatment services York City. Sex Transm Dis. 2022;49(11):790–793.
among young men who have sex with men and https://doi.org/10.1097/OLQ.0000000000001622
transgender persons of color in the US South:
a qualitative analysis. AIDS Educ Prev. 2022;34(6):
512–527. https://doi.org/10.1521/aeap.2022.34.
6.512
24. Rhodes SD, McCoy TP, Vissman AT, et al. A ran-
domized controlled trial of a culturally congruent
intervention to increase condom use and HIV
testing among heterosexually active immigrant
Latino men. AIDS Behav. 2011;15(8):1764–1775.
https://doi.org/10.1007/s10461-011-9903-4
25. Rhodes SD, Alonzo J, Mann L, et al. Small-group
randomized controlled trial to increase condom
January 2024, Vol. 114, No. 1
use and HIV testing among Hispanic/Latino gay,
bisexual, and other men who have sex with men.
Am J Public Health. 2017;107(6):969–976. https://
doi.org/10.2105/AJPH.2017.303814
26. Villarruel AM, Jemmott JB III, Jemmott LS, Ronis DL.
Predictors of sexual intercourse and condom use
intentions among Spanish-dominant Latino youth:
a test of the planned behavior theory. Nurs Res.
2004;53(3):172–181. https://doi.org/10.1097/
00006199-200405000-00004
AJPH
27. Perez-Brumer A, Hatzenbuehler ML, Oldenburg
CE, Bockting W. Individual- and structural-level
risk factors for suicide attempts among transgen-
der adults. Behav Med. 2015;41(3):164–171.
https://doi.org/10.1080/08964289.2015.1028322
28. Phinney J. The Multigroup Ethnic Identity Mea-
sure: a new scale for use with adolescents and
young adults from diverse groups. J Adolesc Res.
1992;7(2):156–176. https://doi.org/10.1177/
074355489272003
29. Gilbert PA, Rhodes SD. Psychometric perfor-
mance of a novel measure of social support
among Spanish-speaking immigrant Latino gay
men. Hisp J Behav Sci. 2012;34(3):491–504.
https://doi.org/10.1177/0739986312446290
30. O’Donnell L, Agronick G, San Doval A, Duran R,
Myint UA, Stueve A. Ethnic and gay community
attachments and sexual risk behaviors among
urban Latino young men who have sex with
men. AIDS Educ Prev. 2002;14(6):457–471. https://
doi.org/10.1521/aeap.14.8.457.24109
31. Vissman AT, Young AM, Wilkin AM, Rhodes SD.
Correlates of HAART adherence among immi-
grant Latinos in the Southeastern United States.
AIDS Care. 2013;25(3):356–363. https://doi.org/
10.1080/09540121.2012.701722
32. Hibbard JH, Mahoney ER, Stockard J, Tusler M.
Development and testing of a short form of
the patient activation measure. Health Serv Res.
2005;40(6, pt 1):1918–1930. https://doi.org/10.
1111/j.1475-6773.2005.00438.x
33. Rhodes SD, Hergenrather KC, Zometa C,
~ o J. Characteristics of
Lindstrom K, Montan
78 Research Peer Reviewed Rhodes et al.
You might also like
- Preventing Hiv Infection in High-Risk Adolescents Using Preexposure Prophylaxis (Prep)Document5 pagesPreventing Hiv Infection in High-Risk Adolescents Using Preexposure Prophylaxis (Prep)Edwin Morales CarboneNo ratings yet
- HIV KomunitasDocument10 pagesHIV KomunitasharisNo ratings yet
- Vaginal Ring Acceptability and Related Preferences Among Women in Low-And Middle-Income Countries: A Systematic Review and Narrative SynthesisDocument22 pagesVaginal Ring Acceptability and Related Preferences Among Women in Low-And Middle-Income Countries: A Systematic Review and Narrative Synthesislidwina143No ratings yet
- HIV Risk Factors Among Transgender PeopleDocument7 pagesHIV Risk Factors Among Transgender PeopleJuan MoralesNo ratings yet
- HHS Public AccessDocument11 pagesHHS Public AccessYTHNo ratings yet
- Association of Self-Reported Adherence and AntiretDocument2 pagesAssociation of Self-Reported Adherence and AntiretDavidNo ratings yet
- Research Project 1Document9 pagesResearch Project 1Sangeeta SahaNo ratings yet
- Comparison of Anal HPV Natural History Among Men by Country of Residence Brazil, Mexico, and The United StatesDocument13 pagesComparison of Anal HPV Natural History Among Men by Country of Residence Brazil, Mexico, and The United StatesLlamencio Kolotikpilli LlamaNo ratings yet
- Factors Influencing Intention To Obtain The HPV Vaccine in South East Asian and Western Pacific Regions: A Systematic Review and Meta-AnalysisDocument11 pagesFactors Influencing Intention To Obtain The HPV Vaccine in South East Asian and Western Pacific Regions: A Systematic Review and Meta-AnalysispangaribuansantaNo ratings yet
- Clinico-Pathological Features of Breast Cancer in PakistanDocument10 pagesClinico-Pathological Features of Breast Cancer in PakistanMurk NiazNo ratings yet
- Jkon 11 171Document8 pagesJkon 11 171pangaribuansantaNo ratings yet
- Predicting Adherence To Antiretroviral Therapy Among Pregnant Women in Guyana: Utility of The Health Belief ModelDocument10 pagesPredicting Adherence To Antiretroviral Therapy Among Pregnant Women in Guyana: Utility of The Health Belief ModelRiska Resty WasitaNo ratings yet
- Sander 2009Document6 pagesSander 2009Rika Yulizah GobelNo ratings yet
- Day 1 TasP PrEP_DitangcoDocument20 pagesDay 1 TasP PrEP_DitangcoRye CalderonNo ratings yet
- HIV Risks and Mental Health of Transgender PersonsDocument7 pagesHIV Risks and Mental Health of Transgender PersonsMaholy MaffaresNo ratings yet
- Linking Women Who Test HIV-positive in Pregnancy-Related Services To Long-Term HIV Care and Treatment Services: A Systematic ReviewDocument17 pagesLinking Women Who Test HIV-positive in Pregnancy-Related Services To Long-Term HIV Care and Treatment Services: A Systematic ReviewAnonymous ljo5ytNo ratings yet
- Treatment Adherence in HIV Stigmatized Environments in South Africa: Stigma Avoidance and Medication ManagementDocument9 pagesTreatment Adherence in HIV Stigmatized Environments in South Africa: Stigma Avoidance and Medication ManagementLeonardo RivagorzaNo ratings yet
- IJWH 9408 Gender Related Mortality For HIV Infected Patients On Highly 041110Document8 pagesIJWH 9408 Gender Related Mortality For HIV Infected Patients On Highly 041110Sex & Gender Women's Health CollaborativeNo ratings yet
- KAP Study on Cervical Cancer ScreeningDocument3 pagesKAP Study on Cervical Cancer ScreeningMominah MayamNo ratings yet
- 07articuloopinion02 (1) (1)Document6 pages07articuloopinion02 (1) (1)jose eduardo Galviz FlorezNo ratings yet
- HIV Risk Perception and Pre-Exposure Prophylaxis (PrEP)Document11 pagesHIV Risk Perception and Pre-Exposure Prophylaxis (PrEP)Óscar GarcíaNo ratings yet
- Christine Tagliaferri Rael Doyel Das Jose Bauermeister Cody Lentz Alex Carballo Diéguez Rebecca Giguere Rachel K. Scott Craig W. HendrixDocument19 pagesChristine Tagliaferri Rael Doyel Das Jose Bauermeister Cody Lentz Alex Carballo Diéguez Rebecca Giguere Rachel K. Scott Craig W. HendrixMichael DeniNo ratings yet
- Influence of Hormonal Contraceptive Use and Health Beliefs on Sexual Orientation Disparities in Papanicolaou Test Use.Document8 pagesInfluence of Hormonal Contraceptive Use and Health Beliefs on Sexual Orientation Disparities in Papanicolaou Test Use.Mayur SarodeNo ratings yet
- JurnalDocument16 pagesJurnalTrysna Ayu SukardiNo ratings yet
- Discover+Lancet+2020Document16 pagesDiscover+Lancet+2020JulianaCerqueiraCésarNo ratings yet
- 1 s2.0 S0140673622005384 MainDocument11 pages1 s2.0 S0140673622005384 Mainwahyuni yuniNo ratings yet
- Efficacy and Safety of Gonorrhea TreatmentsDocument9 pagesEfficacy and Safety of Gonorrhea TreatmentsSamuelRexyNo ratings yet
- Months After Licensure Human Papillomavirus Vaccination Practices: A Survey of US Physicians 18Document11 pagesMonths After Licensure Human Papillomavirus Vaccination Practices: A Survey of US Physicians 18api-30279712No ratings yet
- 10 1016@j Ypmed 2016 10 015Document6 pages10 1016@j Ypmed 2016 10 015Safitri MuhlisaNo ratings yet
- Nej Mo a 2212537Document16 pagesNej Mo a 2212537Zafran KhanNo ratings yet
- 1 s2.0 S0376871607005066 MainDocument9 pages1 s2.0 S0376871607005066 MainAmos AprekuNo ratings yet
- 1 s2.0 S0140673611618461 Main PDFDocument9 pages1 s2.0 S0140673611618461 Main PDFNur Amalina SafitriNo ratings yet
- Ni Hms 489962Document13 pagesNi Hms 489962Rio Surya SaputroNo ratings yet
- Referencias de AMBUDocument10 pagesReferencias de AMBUjosegarcia7No ratings yet
- High-Dose Rifapentine With Moxifloxacin For Pulmonary TuberculosisDocument10 pagesHigh-Dose Rifapentine With Moxifloxacin For Pulmonary TuberculosisSoleh SundawaNo ratings yet
- Original Research: Exposure To Latent Tuberculosis Treatment During PregnancyDocument11 pagesOriginal Research: Exposure To Latent Tuberculosis Treatment During PregnancyBrownNo ratings yet
- Validation of HPV questionnaire for Italian young womenDocument12 pagesValidation of HPV questionnaire for Italian young womenZega AgustianNo ratings yet
- PIIS0140673616309461Document9 pagesPIIS0140673616309461Jose Angel BarreraNo ratings yet
- A Study of The Attitude and Knowledge of Teenagers in The Pietermaritzburg Area Towards ContraceptionDocument4 pagesA Study of The Attitude and Knowledge of Teenagers in The Pietermaritzburg Area Towards Contraceptionjoe blowNo ratings yet
- Ferris - 4v HPV Vaccine in Preadolescents and Adolescents After 10 YearsDocument11 pagesFerris - 4v HPV Vaccine in Preadolescents and Adolescents After 10 YearsGillian Camille AbelloNo ratings yet
- Attitudestoward Theuseof Quarantine in A P Ublic Hea LTH Emergency in Four Cou Ntrie SDocument16 pagesAttitudestoward Theuseof Quarantine in A P Ublic Hea LTH Emergency in Four Cou Ntrie SVina SoumokilNo ratings yet
- 1 35Document8 pages1 35Saiful HudaNo ratings yet
- Jir 342Document4 pagesJir 342Hanifa AdaniNo ratings yet
- Rates and barriers of HIV status disclosure among women in developing countriesDocument9 pagesRates and barriers of HIV status disclosure among women in developing countriesTinkhaniMbichilaNo ratings yet
- Pre Exposure Prophylaxis For Hiv Infection As A Public Health ToolDocument5 pagesPre Exposure Prophylaxis For Hiv Infection As A Public Health ToolMin MinTheinNo ratings yet
- Association Between Contraceptive Implant Knowledge and Intent With Implant Uptake Among Postpartum Malawian Women: A Prospective Cohort StudyDocument16 pagesAssociation Between Contraceptive Implant Knowledge and Intent With Implant Uptake Among Postpartum Malawian Women: A Prospective Cohort StudyAyu WidnyaningsihNo ratings yet
- Factors Predicting Completion of the HPV Vaccine SeriesDocument6 pagesFactors Predicting Completion of the HPV Vaccine SeriesVeronica Cordoba SanchezNo ratings yet
- ACHA HIV PrEP Guidelines Jan2019Document13 pagesACHA HIV PrEP Guidelines Jan2019Bear DoctorNo ratings yet
- Hormonal Contraception and Sexual DesireDocument19 pagesHormonal Contraception and Sexual Desirebustanul aswatNo ratings yet
- Effectiveness of Highly Active Antiretroviral Therapy Among HIV-1 Infected WomenDocument7 pagesEffectiveness of Highly Active Antiretroviral Therapy Among HIV-1 Infected Womenujangketul62No ratings yet
- Contraceptive Use and Unplanned Pregnancy Among Female Sex Workers in ZambiaDocument7 pagesContraceptive Use and Unplanned Pregnancy Among Female Sex Workers in ZambiaNiki Rizqi rachmawatiNo ratings yet
- The Joint Philippine Society of Gastroenterology and Philippine Society of Digestive Endoscopy Consensus Guidelines PDFDocument16 pagesThe Joint Philippine Society of Gastroenterology and Philippine Society of Digestive Endoscopy Consensus Guidelines PDFaxxoNo ratings yet
- Chapter 2 (Abeleda)Document2 pagesChapter 2 (Abeleda)John Patrick AbeledaNo ratings yet
- 4-On 3-Off Journal Handout 3Document2 pages4-On 3-Off Journal Handout 3api-594366475No ratings yet
- Vol2issue2 Ijmrp 320-23Document4 pagesVol2issue2 Ijmrp 320-23Neerav DuttaNo ratings yet
- Development of A Natural Language Processing Algorithm To Identify A PDFDocument10 pagesDevelopment of A Natural Language Processing Algorithm To Identify A PDFKaumudi LiyanageNo ratings yet
- Jurnal Baru PSK 1 PDFDocument8 pagesJurnal Baru PSK 1 PDFsanta_pangaribuan_1No ratings yet
- HIV Prevention in Primary Care Practice: A PrEP PrimerFrom EverandHIV Prevention in Primary Care Practice: A PrEP PrimerNo ratings yet
- Birth in the Age of AIDS: Women, Reproduction, and HIV/AIDS in IndiaFrom EverandBirth in the Age of AIDS: Women, Reproduction, and HIV/AIDS in IndiaNo ratings yet
- Contraception for the Medically Challenging PatientFrom EverandContraception for the Medically Challenging PatientRebecca H. AllenNo ratings yet
- The Guardian Weekly - 0812Document64 pagesThe Guardian Weekly - 0812En DimunNo ratings yet
- Straight Talk, June 2008Document4 pagesStraight Talk, June 2008Straight Talk Foundation100% (2)
- Strengthening Organizations Serving Key PopulationsDocument54 pagesStrengthening Organizations Serving Key PopulationsBonike MustaqiemNo ratings yet
- Attempts On Her LifeDocument42 pagesAttempts On Her LifeGargi DatarNo ratings yet
- Guder Quarterly Report 2022Document7 pagesGuder Quarterly Report 2022mohammedamin oumerNo ratings yet
- Chapter 1 Writing2Document12 pagesChapter 1 Writing2Xuan ThuyNo ratings yet
- Supportive Supervision Check ListDocument6 pagesSupportive Supervision Check ListJoeYeshitellaNo ratings yet
- Should College Students Be Tested For AIDSx - Edited (1) .EditedDocument4 pagesShould College Students Be Tested For AIDSx - Edited (1) .EditedAllan MwangiNo ratings yet
- July 18 2014Document48 pagesJuly 18 2014fijitimescanadaNo ratings yet
- Dedication Speech - Princess DianaDocument2 pagesDedication Speech - Princess DianaAlexándra NicoleNo ratings yet
- SPI RRT Checklist User GuideDocument41 pagesSPI RRT Checklist User GuideUdofia Nicholas100% (1)
- NEPHAK Vacancy Data Clerk Position PDFDocument2 pagesNEPHAK Vacancy Data Clerk Position PDFDennis BondNo ratings yet
- 05 14 20 MagicPointsPress SJohnson Test Inter Xn7ojyDocument580 pages05 14 20 MagicPointsPress SJohnson Test Inter Xn7ojyVincent Leung100% (4)
- Introduction To HIV/AIDS Assignment: (Ii) (Iii) 1Document1 pageIntroduction To HIV/AIDS Assignment: (Ii) (Iii) 1VIJENDRA CHANDRANo ratings yet
- 2 17+-+Zimbabwe+CATS+-+long+form+-+1 13 18Document10 pages2 17+-+Zimbabwe+CATS+-+long+form+-+1 13 18Rumbidzai MurwisiNo ratings yet
- Cover LetterDocument1 pageCover LetterSileshi NegashNo ratings yet
- Participant List PDFDocument204 pagesParticipant List PDFPriyank M Desai100% (1)
- ALI MUMED INDIVIDUAL ASSINMENT TWO Socialpolicy - Short NotesDocument20 pagesALI MUMED INDIVIDUAL ASSINMENT TWO Socialpolicy - Short NotesDukkana BariisaaNo ratings yet
- Street ChildrenDocument2 pagesStreet ChildrenAmani Innerarity (Billy)No ratings yet
- Employment Application FormDocument3 pagesEmployment Application FormLenny PangNo ratings yet
- Improving GEND - GBV Data Quality To Enhance PEPFAR Program PerformanceDocument1 pageImproving GEND - GBV Data Quality To Enhance PEPFAR Program PerformanceAliNo ratings yet
- Jhpeigo Advert - Case Manager.Document2 pagesJhpeigo Advert - Case Manager.John EkerekeNo ratings yet
- Unit 2 HEALTH MAPEH 10Document5 pagesUnit 2 HEALTH MAPEH 10Aj AntonioNo ratings yet
- Turkey Position PaperDocument3 pagesTurkey Position PaperBill GatesNo ratings yet
- PROJECT PROPOSAL FOR THE VehackleDocument5 pagesPROJECT PROPOSAL FOR THE VehackleKalayu KirosNo ratings yet
- Ipcr NDPDocument1 pageIpcr NDPGABIETA MeshachNo ratings yet
- I Want For Young People and The Future GenerationsDocument8 pagesI Want For Young People and The Future GenerationsGlenn Lyndon FloresNo ratings yet
- RISE CEP Workshop - RISE Tanzania VMMC Project Overview - Handout - September 2022Document2 pagesRISE CEP Workshop - RISE Tanzania VMMC Project Overview - Handout - September 2022munna shabaniNo ratings yet
- National Aids Control ProgrammeDocument3 pagesNational Aids Control Programmearunjv1234No ratings yet
- Ideal Clinic Manual - Version 19 - Updated May 2021Document401 pagesIdeal Clinic Manual - Version 19 - Updated May 2021امير الضلام100% (3)