You might also like
- DSWD Eccd Child ProfileDocument2 pagesDSWD Eccd Child ProfileMaye Bacani78% (134)
- LRP 1 28 Pages in AllDocument28 pagesLRP 1 28 Pages in AllJeslie Del Ayre Luza97% (32)
- ECCD Soft Copy - Self MadeDocument14 pagesECCD Soft Copy - Self MadeOFW SF100% (1)
- Masterlist of ChildrenDocument8 pagesMasterlist of ChildrenJoena Balicao0% (1)
- Guidelines On Reg and Granting of Permit and Recog To Publ and Pte CDCs LCs Offering Early Childhood Prog For 0-4 Years Old CHNDocument85 pagesGuidelines On Reg and Granting of Permit and Recog To Publ and Pte CDCs LCs Offering Early Childhood Prog For 0-4 Years Old CHNMelona Barrientos100% (2)
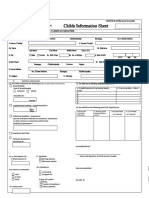
- Child Information Sheet: Male FemaleDocument2 pagesChild Information Sheet: Male FemaleBrgy. M. Parang86% (7)
- Forms For AccreditationDocument58 pagesForms For AccreditationAngelica Trono100% (2)
- Philippine Early Childhood Development Checklist: Child's Record Form 2Document1 pagePhilippine Early Childhood Development Checklist: Child's Record Form 2Jeremias De la Cruz100% (3)
- BHW Monthly Report FormDocument3 pagesBHW Monthly Report FormPearlCarylCatantan-Cadavis80% (5)
- Class D: Land Bank of The PhlippinesDocument2 pagesClass D: Land Bank of The PhlippinesDominic Pedrocillo50% (2)
- Learning Resource Guide No 2Document45 pagesLearning Resource Guide No 2JOVITA SARAOS100% (1)
- Master List of Women of Reproductive Age and Adolescent Women For Family Planning ServicesDocument19 pagesMaster List of Women of Reproductive Age and Adolescent Women For Family Planning ServicesAlawi Abdillah100% (1)
- I. Identifying Information NOTE Fields ( ) Asterisk Are Required Fields 1Document3 pagesI. Identifying Information NOTE Fields ( ) Asterisk Are Required Fields 1adoptify89% (28)
- Service ProviderDocument1 pageService ProviderBern Evora Alvis80% (15)
- SFP Masterlist, CNS Forms For LGUs NewDocument4 pagesSFP Masterlist, CNS Forms For LGUs NewJohny F. Villanueva0% (1)
- ECCD LOGO - STANDARDS AND GUIDELINES v4Document60 pagesECCD LOGO - STANDARDS AND GUIDELINES v4Fritz Maguinda67% (3)
- 8 BNS Form No. 4 FINAL RSB Mlav BNS Semestral Accomplishment Report SARDocument14 pages8 BNS Form No. 4 FINAL RSB Mlav BNS Semestral Accomplishment Report SARIvy Glady Alcantara Garcia83% (6)
- OPT Plus Form 1Document1 pageOPT Plus Form 1ApOlle Defiesta - DOminguezNo ratings yet
- 107 NLE Leadership and Management QuestionDocument4 pages107 NLE Leadership and Management QuestionMae Montesena Breganza100% (1)
- Antopina, Nethan YuriDocument2 pagesAntopina, Nethan YuriElsang Obera SanielNo ratings yet
- Children Served ProfileDocument1 pageChildren Served ProfileMonteza Dela Serna100% (4)
- Child Information SheetDocument2 pagesChild Information SheetKurt Steve Andrei Aquino100% (6)
- ECCD Facility ProfileDocument1 pageECCD Facility ProfileBern Evora Alvis100% (2)
- Pahintulot para Sa Day Care ServiceDocument9 pagesPahintulot para Sa Day Care ServiceKathleen Rose LibedNo ratings yet
- New Assessment Tool For The Granting of Recognition.Document36 pagesNew Assessment Tool For The Granting of Recognition.Maricho Magbanua Bentazal100% (1)
- Parents Committee Action PlanDocument3 pagesParents Committee Action PlanDodong G100% (5)
- SFP Form 2A & ACCOMPLISHMENT REPORTDocument2 pagesSFP Form 2A & ACCOMPLISHMENT REPORTMary Jane Martinez80% (5)
- List of Folders 21 PCS UpdatedDocument2 pagesList of Folders 21 PCS UpdatedLilibeth G. SacramentoNo ratings yet
- CDC HandbookDocument35 pagesCDC HandbookAngelica Sumaoang100% (1)
- Child Information Sheet DSWDDocument3 pagesChild Information Sheet DSWDRachel Balatucan100% (1)
- Annual Action PlanDocument2 pagesAnnual Action PlanPearl Angeli Quisido Canada91% (11)
- Accreditation For New ToolsDocument10 pagesAccreditation For New ToolsGlenda Ang BacomoNo ratings yet
- 0203 APPROVED FINAL VERSION On Assessment Tool For CDCs & LCs 2015Document73 pages0203 APPROVED FINAL VERSION On Assessment Tool For CDCs & LCs 2015ELlaii BadiLla Santianez100% (1)
- Weight Monitoring FormDocument1 pageWeight Monitoring FormChristopher Torres50% (2)
- Form 6 - Child Developmet Worker ProfileDocument3 pagesForm 6 - Child Developmet Worker ProfileHannah Naki Medina67% (3)
- New Accreditation Tool FoldersDocument1 pageNew Accreditation Tool FoldersJeanette Gonzales100% (2)
- List of Forms Per AreaDocument10 pagesList of Forms Per AreaLyle Guion PaguioNo ratings yet
- PDF Quarter 4 - CompleteDocument114 pagesPDF Quarter 4 - CompleteMerbert Pascua100% (2)
- Sagud Bahley-Parents-HandbookDocument14 pagesSagud Bahley-Parents-HandbookAira ReyesNo ratings yet
- Accomplishment Report For The Month of May 2021 City Camp Proper Child Development CenterDocument5 pagesAccomplishment Report For The Month of May 2021 City Camp Proper Child Development Centerkimberly fernandez100% (1)
- Weight For Height Boys GirlsDocument2 pagesWeight For Height Boys GirlsKristel Anne Mendoza75% (4)
- Early Childhood and Development (ECD) : ChecklistDocument6 pagesEarly Childhood and Development (ECD) : ChecklistRose Marie Prietos100% (1)
- Handwashing and ToothbrushingDocument5 pagesHandwashing and ToothbrushingLea RemorozaNo ratings yet
- HAPAG-ASA FILL UP FORM MANA PACK REPORT CabiraoanDocument2 pagesHAPAG-ASA FILL UP FORM MANA PACK REPORT CabiraoanJeferson SardengNo ratings yet
- Checklist: Early Childhood Care and Development (ECCD)Document2 pagesChecklist: Early Childhood Care and Development (ECCD)marivicbello100% (1)
- Master List Beneficiaries For School-Based Feeding Program (SBFP)Document12 pagesMaster List Beneficiaries For School-Based Feeding Program (SBFP)Altea Garcia100% (1)
- VAWC Monthly ReportDocument1 pageVAWC Monthly ReportMswdo Talavera100% (2)
- ECCD Checklist Child S Record 1Document24 pagesECCD Checklist Child S Record 1Noriz Jean Baldecasa100% (21)
- Eccd Facility Profile 10222020Document2 pagesEccd Facility Profile 10222020Geannjoy Herrera DelRosarioNo ratings yet
- Daycare CertificateDocument2 pagesDaycare Certificaterhenz villafuerteNo ratings yet
- Resolution No. 025 - BNC 2024Document3 pagesResolution No. 025 - BNC 2024Kimberly Bring100% (1)
- Home Center AgreementDocument1 pageHome Center AgreementMonteza Dela SernaNo ratings yet
- Center-Based Eccd PROGRAM Conducted in An Alternative Venue (CBPAV)Document24 pagesCenter-Based Eccd PROGRAM Conducted in An Alternative Venue (CBPAV)GenderAnd Development Mabalacat100% (5)
- Ra 7610Document65 pagesRa 7610Mikhayla KateNo ratings yet
- Gad Accomplishment Report FormDocument2 pagesGad Accomplishment Report FormArman Bentain92% (12)
- Eccd Front PageDocument1 pageEccd Front PageOFW SF100% (2)
- NCD Risk Assessment FormDocument1 pageNCD Risk Assessment Formruiza corcino100% (4)
- Child Information SheetDocument3 pagesChild Information SheetHaidi MeanaNo ratings yet
- SCDF V4b3Document3 pagesSCDF V4b3Sherwin BalladNo ratings yet
- Senior Citizen Data FormDocument2 pagesSenior Citizen Data FormLex Lee Matuan100% (2)
- Zoonotic Disease PreventionDocument48 pagesZoonotic Disease Preventionavenger 2100% (1)
- Assessment Hair Skin NailsDocument51 pagesAssessment Hair Skin Nailsclyde i amNo ratings yet
- Human Fascioliasis Infection Sources Their Diversity Incidence Factors Analytical Methods and Prevention Measures PDFDocument35 pagesHuman Fascioliasis Infection Sources Their Diversity Incidence Factors Analytical Methods and Prevention Measures PDFmuchlis syahnuddinNo ratings yet
- WORKSHEET NSTP EditedDocument30 pagesWORKSHEET NSTP EditedHannahbea LindoNo ratings yet
- Upper Gastrointestinal BleedingDocument32 pagesUpper Gastrointestinal BleedinglicservernoidaNo ratings yet
- PE - LVI - 13 - 270321 - Kanthi Swaroop, Joel LeeDocument8 pagesPE - LVI - 13 - 270321 - Kanthi Swaroop, Joel Leeveeveebakkup baccupNo ratings yet
- BAUTISTA, DYANNE G. - Adult NursingHypertension Case StudyDocument15 pagesBAUTISTA, DYANNE G. - Adult NursingHypertension Case StudyDyanne BautistaNo ratings yet
- Intertrochanteric Femur Fracture: Attum B, Pilson HDocument6 pagesIntertrochanteric Femur Fracture: Attum B, Pilson HEduardo Anaya DuranNo ratings yet
- Enhancing Germination of Bitter Cola (Garcinia Kola) Heckel: Prospects For Agroforestry Farmers in The Niger DeltaDocument8 pagesEnhancing Germination of Bitter Cola (Garcinia Kola) Heckel: Prospects For Agroforestry Farmers in The Niger DeltaAlvaroNo ratings yet
- Jurnal Mutiple StentDocument9 pagesJurnal Mutiple StentPrima Anggreini ArinNo ratings yet
- Inpatient Placement and Management of Nasogastric and Nasoenteric Tubes in Adults - UpToDateDocument25 pagesInpatient Placement and Management of Nasogastric and Nasoenteric Tubes in Adults - UpToDateDylanNo ratings yet
- HES 032 BSN Case Analysis Lecture P2 Exam 2Document5 pagesHES 032 BSN Case Analysis Lecture P2 Exam 2Nicole AntasudaNo ratings yet
- Ipe - Neuro - Kelompok 8aDocument20 pagesIpe - Neuro - Kelompok 8aHanis NandaNo ratings yet
- Guideline Anti TrombolitikDocument43 pagesGuideline Anti TrombolitikWahyulin Trisna SyafitriNo ratings yet
- Skin ConditionsDocument3 pagesSkin ConditionsAlyssa AmayaNo ratings yet
- Urban Search and Rescue TeamDocument5 pagesUrban Search and Rescue TeamMehmet hakki BilgitekinNo ratings yet
- Project Health and Safety Measures of EmployeeDocument83 pagesProject Health and Safety Measures of Employeeaurorashiva1No ratings yet
- Abnormal Sexuality and Sexual DysfunctionsDocument8 pagesAbnormal Sexuality and Sexual DysfunctionsIsabel CastilloNo ratings yet
- SBI3U Unit 1Document5 pagesSBI3U Unit 1Sara SNo ratings yet
- 7 Pediatric History and Physical ExaminationDocument45 pages7 Pediatric History and Physical ExaminationAmaetenNo ratings yet
- Bioactive PeptidesDocument16 pagesBioactive PeptidesOmotoyinbo SegunNo ratings yet
- G6 English LAS FINALIZEDDocument29 pagesG6 English LAS FINALIZEDJobette ExallieNo ratings yet
- Drug Tabulation orDocument23 pagesDrug Tabulation orChin Villanueva UlamNo ratings yet
- Learning Zone: Thyroidectomy: Post-Operative Care and Common ComplicationsDocument10 pagesLearning Zone: Thyroidectomy: Post-Operative Care and Common ComplicationsJan BularioNo ratings yet
- PCR COVID-19: Negative: If You Have Any Questions Regarding This Report Please Contact Your ProviderDocument1 pagePCR COVID-19: Negative: If You Have Any Questions Regarding This Report Please Contact Your ProviderLuis ReyesNo ratings yet
- Valentino Rački, Igor Vlatković, Mila Prskalo Daniela PetrićDocument1 pageValentino Rački, Igor Vlatković, Mila Prskalo Daniela PetrićIgor VlatkovićNo ratings yet
- Perhimpunan Kedokteran Nuklir Dan Teragnostik Molekuler IndonesiaDocument20 pagesPerhimpunan Kedokteran Nuklir Dan Teragnostik Molekuler IndonesiaolakasturiNo ratings yet
- Physio Lab CasesDocument4 pagesPhysio Lab CasesJoseph KimNo ratings yet
- Manual Cardiovascular SystemDocument5 pagesManual Cardiovascular SystemVynz Morales CosepNo ratings yet