You might also like
- Sensitive On-Site Detection of SARS-CoV-2 by ID NOW COVID-19Document12 pagesSensitive On-Site Detection of SARS-CoV-2 by ID NOW COVID-19luis.achaNo ratings yet
- 2020.02.26.20028373v1.fullDocument14 pages2020.02.26.20028373v1.fullhogirimmunologyNo ratings yet
- Title: Antigen Rapid Tests, Nasopharyngeal PCR and Saliva PCR To Detect Sars-Cov-2: A Prospective Comparative Clinical TrialDocument16 pagesTitle: Antigen Rapid Tests, Nasopharyngeal PCR and Saliva PCR To Detect Sars-Cov-2: A Prospective Comparative Clinical Trialorkut verificationNo ratings yet
- Improtant Neeed To Know When CovidDocument3 pagesImprotant Neeed To Know When Covid12194-Yazan Maan HijaziNo ratings yet
- Detecting Sars-Cov-2 at Point of Care: Preliminary Data Comparing Loop-Mediated Isothermal Amplification (Lamp) To Polymerase Chain Reaction (PCR)Document8 pagesDetecting Sars-Cov-2 at Point of Care: Preliminary Data Comparing Loop-Mediated Isothermal Amplification (Lamp) To Polymerase Chain Reaction (PCR)Prita Amira Windy AsmaraNo ratings yet
- Highly Accurate and Sensitive Diagnostic Detection of Sars-Cov-2 by Digital PCRDocument23 pagesHighly Accurate and Sensitive Diagnostic Detection of Sars-Cov-2 by Digital PCRJosé ManriqueNo ratings yet
- Journal Pre-Proof: Journal of Clinical VirologyDocument14 pagesJournal Pre-Proof: Journal of Clinical VirologyMajlinda HalitiNo ratings yet
- L'Helgouach-2020-EasyCOV - LAMP Based Rapid deDocument14 pagesL'Helgouach-2020-EasyCOV - LAMP Based Rapid deGerman MadrigalNo ratings yet
- Genoamp® Real-Time PCR Tests For Detection of Covid-19: Mahtas Covid-19 Rapid Evidence UpdatesDocument5 pagesGenoamp® Real-Time PCR Tests For Detection of Covid-19: Mahtas Covid-19 Rapid Evidence UpdatesDesmond KhorNo ratings yet
- Comparison of Seven Commercial RT-PCR Diagnostic Kits For COVID-19Document6 pagesComparison of Seven Commercial RT-PCR Diagnostic Kits For COVID-19Simona VisanNo ratings yet
- Diagnostic Aspect of COVIDDocument8 pagesDiagnostic Aspect of COVIDYanMardianNo ratings yet
- Genes 11 00664 v2Document13 pagesGenes 11 00664 v2Monika GonzalezNo ratings yet
- Clinical Applications of PCR for COVID-19 DetectionDocument5 pagesClinical Applications of PCR for COVID-19 Detectionاحمد مثنىNo ratings yet
- Side by SideDocument31 pagesSide by SideYosua Butar ButarNo ratings yet
- SARS-CoV-2 Specific Antibody Responses in Covid-19 PatientsDocument18 pagesSARS-CoV-2 Specific Antibody Responses in Covid-19 PatientsSaifuddin HaswareNo ratings yet
- Control of Covid-19: Martin L. Nelwan, PHDDocument18 pagesControl of Covid-19: Martin L. Nelwan, PHDShikha GuptaNo ratings yet
- Evaluation of Antibody Testing For Sars-Cov-2 Using Elisa and Lateral Flow ImmunoassaysDocument24 pagesEvaluation of Antibody Testing For Sars-Cov-2 Using Elisa and Lateral Flow ImmunoassaysAbhinavNo ratings yet
- Journal Pone 0260087Document17 pagesJournal Pone 0260087Steve Vladimir Acedo LazoNo ratings yet
- Artic - Covid 19Document19 pagesArtic - Covid 19cristinaNo ratings yet
- 2020 04 24 20078949v1 FullDocument14 pages2020 04 24 20078949v1 FullAbay SisayNo ratings yet
- Swab Pooling For Large-Scale RT-QPCR Screening of Sars-Cov-2Document22 pagesSwab Pooling For Large-Scale RT-QPCR Screening of Sars-Cov-2popov357No ratings yet
- Design of A Novel Multiplex Real Time RT-PCR Assay For Sars-Cov-2 DetectionDocument16 pagesDesign of A Novel Multiplex Real Time RT-PCR Assay For Sars-Cov-2 DetectionHasna Mirda AmazanNo ratings yet
- Journal Pre-Proof: Journal of Clinical VirologyDocument12 pagesJournal Pre-Proof: Journal of Clinical Virologyamer khanNo ratings yet
- JurnalDocument6 pagesJurnalDaffa AthaNo ratings yet
- Covid 19 UpdateDocument43 pagesCovid 19 UpdateSanjay BhattacharyaNo ratings yet
- The Detection Dogs Test Is More Sensitive Than Real-Time PCR in Screening For SARS-CoV-2Document7 pagesThe Detection Dogs Test Is More Sensitive Than Real-Time PCR in Screening For SARS-CoV-2Alejandro MerelesNo ratings yet
- A Role For Biofoundries in Rapid Development and Validation of Automated Sars-Cov-2 Clinical DiagnosticsDocument11 pagesA Role For Biofoundries in Rapid Development and Validation of Automated Sars-Cov-2 Clinical DiagnosticsRicardoPeixotoNo ratings yet
- The COVID-19 RT-PCR Test - How To Mislead All Humanity. Using A Test To Lock Down SocietyDocument11 pagesThe COVID-19 RT-PCR Test - How To Mislead All Humanity. Using A Test To Lock Down SocietyCarlCordNo ratings yet
- Predicting Infectious Severe Acute Respiratory Syndrome Coronavirus 2 From Diagnostic SamplesDocument4 pagesPredicting Infectious Severe Acute Respiratory Syndrome Coronavirus 2 From Diagnostic SamplesmikhaelyosiaNo ratings yet
- 1 s2.0 S1386653220302420 MainDocument4 pages1 s2.0 S1386653220302420 MainZahira SafouanNo ratings yet
- Jurnal IntropDocument4 pagesJurnal IntropnadaNo ratings yet
- 10.1007@s11033 020 05889 3Document9 pages10.1007@s11033 020 05889 3phamnguyenthaovy3101No ratings yet
- 12 10 1Document7 pages12 10 1Phuong NguyenNo ratings yet
- PCR Diagnostic Testing For Sars-Cov-2Document2 pagesPCR Diagnostic Testing For Sars-Cov-2Matibar RahmanNo ratings yet
- Presence of Mismatches Between Diagnostic PCR Assays and Coronavirus Sars-Cov-2 GenomeDocument17 pagesPresence of Mismatches Between Diagnostic PCR Assays and Coronavirus Sars-Cov-2 GenomeYulaimy BatistaNo ratings yet
- Emergency Response For Evaluating Sars-Cov-2 Immune Status, Seroprevalence and Convalescent Plasma in ArgentinaDocument28 pagesEmergency Response For Evaluating Sars-Cov-2 Immune Status, Seroprevalence and Convalescent Plasma in ArgentinaCesar AlonsoNo ratings yet
- Arévalo, A. (2020) ELIPSE-COL A Novel ELISA Test Based On Rational Envisioned Synthetic Peptides For Detection of SARS-CoV-2 Infection in ColombiaDocument14 pagesArévalo, A. (2020) ELIPSE-COL A Novel ELISA Test Based On Rational Envisioned Synthetic Peptides For Detection of SARS-CoV-2 Infection in ColombiaDiana PachónNo ratings yet
- Real-Time RT-PCR For COVID-19 Diagnosis: Challenges and ProspectsDocument3 pagesReal-Time RT-PCR For COVID-19 Diagnosis: Challenges and ProspectsAnthony StackNo ratings yet
- PIIS1198743X20306972Document4 pagesPIIS1198743X20306972KARLA PATRICIA DIAZ LOPEZNo ratings yet
- Makalah Biologi MolekulerDocument11 pagesMakalah Biologi MolekulerSarah PanjaitanNo ratings yet
- Real Time RT PCR in COVID 19 Detection Issues Affecting The ResultsDocument3 pagesReal Time RT PCR in COVID 19 Detection Issues Affecting The ResultsBruno FicaNo ratings yet
- Covid19 Methods PDFDocument14 pagesCovid19 Methods PDFSulieman OmarNo ratings yet
- Corman-Drosten Review ReportDocument38 pagesCorman-Drosten Review ReportBuzzUrbiaNo ratings yet
- RTLAMPDocument15 pagesRTLAMPAndrea GarciaNo ratings yet
- Covid-19 A Panoramic View (Part 3) : European Journal of Pharmaceutical and Medical ResearchDocument10 pagesCovid-19 A Panoramic View (Part 3) : European Journal of Pharmaceutical and Medical ResearchRuchiNo ratings yet
- 2022 01 06 21268555v1 FullDocument24 pages2022 01 06 21268555v1 FullJaakko MeriläinenNo ratings yet
- Antibody Tests in Detecting SARS-CoV-2 MetanalisisDocument18 pagesAntibody Tests in Detecting SARS-CoV-2 MetanalisisRenato DesideriNo ratings yet
- Paramyxoviridae Family (1) - The Disease Is Enzootic: Open AccessDocument6 pagesParamyxoviridae Family (1) - The Disease Is Enzootic: Open Accessinvestbiz optionstarNo ratings yet
- Week 1.4 Covid19Document36 pagesWeek 1.4 Covid19Azalea BitchNo ratings yet
- Up Date Diagnosis Laboratorium Pada Pedoman: Pencegahan Dan Pengendalian COVID-19 Revisi Ke-5Document65 pagesUp Date Diagnosis Laboratorium Pada Pedoman: Pencegahan Dan Pengendalian COVID-19 Revisi Ke-5Muhammad NurfiantoroNo ratings yet
- Validasi Rapid AntigenDocument6 pagesValidasi Rapid Antigengaki telitiNo ratings yet
- 1 s2.0 S0033350620301141 MainDocument3 pages1 s2.0 S0033350620301141 MainFedrik Monte Kristo LimbongNo ratings yet
- ATMP PadleyDocument11 pagesATMP PadleyAboubakar SidickNo ratings yet
- Detection of Sars-Cov-19 Delta Mutant by RT-PCR: A. Sample CollectionDocument4 pagesDetection of Sars-Cov-19 Delta Mutant by RT-PCR: A. Sample CollectionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Epidemiological Description and Analysis of RDRP, E and N Genes Dynamic by RT-PCR of SARS-CoV-2 in Moroccan Population - Experience of The National Reference Laboratory (LNR) - UM6SSDocument12 pagesEpidemiological Description and Analysis of RDRP, E and N Genes Dynamic by RT-PCR of SARS-CoV-2 in Moroccan Population - Experience of The National Reference Laboratory (LNR) - UM6SSolfianyNo ratings yet
- The Appropriate Use of Testing For COVID-19Document4 pagesThe Appropriate Use of Testing For COVID-19newazNo ratings yet
- Predicting Infectious Severe Acute Respiratory Syndrome Coronavirus 2 From Diagnostic SamplesDocument4 pagesPredicting Infectious Severe Acute Respiratory Syndrome Coronavirus 2 From Diagnostic SamplesArum Rahmawatie VirgieNo ratings yet
- Journal Pre-Proof: Trends in Plant ScienceDocument17 pagesJournal Pre-Proof: Trends in Plant ScienceMUGDHA MITTALNo ratings yet
- CoronavirusTestRealTime RTPCR - MUSABSMT1BDocument4 pagesCoronavirusTestRealTime RTPCR - MUSABSMT1BJuhany MusaNo ratings yet
- SARS-CoV-2 Viral Outbreak Investigation: Laboratory Perspective: Clinical Updates in COVID-19From EverandSARS-CoV-2 Viral Outbreak Investigation: Laboratory Perspective: Clinical Updates in COVID-19Rating: 3 out of 5 stars3/5 (1)
- Single-Stranded DNA (ssDNA) Production in DNA Aptamer GenerationDocument9 pagesSingle-Stranded DNA (ssDNA) Production in DNA Aptamer GenerationPetr CiglerNo ratings yet
- REVIEW Janus Particles - Design, Preparation, and Biomedical ApplicationsDocument19 pagesREVIEW Janus Particles - Design, Preparation, and Biomedical ApplicationsPetr CiglerNo ratings yet
- Inhibition of HSV-1 Attachment, Entry Etc-ProofsDocument10 pagesInhibition of HSV-1 Attachment, Entry Etc-ProofsPetr CiglerNo ratings yet
- Tailored Synthesis of Octopus-Type Janus Nanoparticles - Angewandte SUPPLDocument12 pagesTailored Synthesis of Octopus-Type Janus Nanoparticles - Angewandte SUPPLPetr CiglerNo ratings yet
- Hvaa029 PDFDocument7 pagesHvaa029 PDFAditya NobelNo ratings yet
- ! Self-Propelled Nanomotors For Thermomechanically Percolating Cell MembraneDocument5 pages! Self-Propelled Nanomotors For Thermomechanically Percolating Cell MembranePetr CiglerNo ratings yet
- Janus Nanoparticles in Cancer Diagnosis, TherapyDocument14 pagesJanus Nanoparticles in Cancer Diagnosis, TherapyPetr CiglerNo ratings yet
- Diamond & Related MaterialsDocument22 pagesDiamond & Related MaterialsPetr Cigler100% (1)
- DNA-based Self-Assembly of Fluorescent NanodiamondsDocument4 pagesDNA-based Self-Assembly of Fluorescent NanodiamondsPetr CiglerNo ratings yet
- Silicon and Germanium Nanocrystals - Properties and CharacterizationDocument8 pagesSilicon and Germanium Nanocrystals - Properties and CharacterizationPetr CiglerNo ratings yet
- Structural and Optical Properties of DNA Layers On NDDocument26 pagesStructural and Optical Properties of DNA Layers On NDPetr CiglerNo ratings yet
- Germanium Nanoparticles From Solvated Atoms - Synthesis and CharacterizationDocument8 pagesGermanium Nanoparticles From Solvated Atoms - Synthesis and CharacterizationPetr CiglerNo ratings yet
- Janus Nanoparticles - Recent AdvancesDocument20 pagesJanus Nanoparticles - Recent AdvancesPetr CiglerNo ratings yet
- Inhibition of HIV Fusion With Multivalent Gold NanoparticlesDocument10 pagesInhibition of HIV Fusion With Multivalent Gold NanoparticlesPetr CiglerNo ratings yet
- Synthetic DNA Delivery Systems - Review NatureBiotech 2000Document5 pagesSynthetic DNA Delivery Systems - Review NatureBiotech 2000Petr CiglerNo ratings yet
- Functionalization of Ultradispersed Diamond For DNA DetectionDocument7 pagesFunctionalization of Ultradispersed Diamond For DNA DetectionPetr CiglerNo ratings yet
- Srep07372 PDFDocument6 pagesSrep07372 PDFPetr CiglerNo ratings yet
- DNA-Modified Diamond SurfacesDocument5 pagesDNA-Modified Diamond SurfacesPetr CiglerNo ratings yet
- Polylysine-Coated Diamond Nanocrystals For MALDI of OligosDocument5 pagesPolylysine-Coated Diamond Nanocrystals For MALDI of OligosPetr CiglerNo ratings yet
- Single-Cell Injection of Functionalized ND PDFDocument8 pagesSingle-Cell Injection of Functionalized ND PDFPetr CiglerNo ratings yet
- RNAi Therapeutics - A Potential New Class of Pharmaceutical Drugs - Nat Chem Biol 2011 PDFDocument9 pagesRNAi Therapeutics - A Potential New Class of Pharmaceutical Drugs - Nat Chem Biol 2011 PDFPetr CiglerNo ratings yet
- Lee Et Al. - 2011 - PEGylated Polyethyleneimine Grafted Silica NanoparDocument11 pagesLee Et Al. - 2011 - PEGylated Polyethyleneimine Grafted Silica NanoparPetr CiglerNo ratings yet
- Gene Therapy Needs Robust Synthetic Nonviral PlatformDocument3 pagesGene Therapy Needs Robust Synthetic Nonviral PlatformPetr CiglerNo ratings yet
- Grappa HandbookDocument66 pagesGrappa HandbookPetr CiglerNo ratings yet
- Micelle-Like NanoparticlesDocument9 pagesMicelle-Like NanoparticlesPetr CiglerNo ratings yet
- Linking Words and PhrasesDocument4 pagesLinking Words and PhrasesAntonio ImperiNo ratings yet
- Nanodiamonds As Vehicles For Gene Delivery - ACS Nano 2009Document9 pagesNanodiamonds As Vehicles For Gene Delivery - ACS Nano 2009Petr CiglerNo ratings yet
- Hydroxamic Acids As A Novel Family of Serine Racemase Inhibitors - JMedChem 2009Document25 pagesHydroxamic Acids As A Novel Family of Serine Racemase Inhibitors - JMedChem 2009Petr CiglerNo ratings yet
- Elicitation of An Intact Medical Plant - Kuzel 2009Document5 pagesElicitation of An Intact Medical Plant - Kuzel 2009Petr CiglerNo ratings yet
- Design of Potent HIV Protease Inhibitors Based On Inorganic Polyhedral MetallacarboranesDocument26 pagesDesign of Potent HIV Protease Inhibitors Based On Inorganic Polyhedral MetallacarboranesPetr CiglerNo ratings yet
- Test Bank For Human Heredity Principles and Issues 11th Edition CummingsDocument3 pagesTest Bank For Human Heredity Principles and Issues 11th Edition CummingsChristopher Urbina100% (30)
- Amoeba Sisters BiomoleculesDocument2 pagesAmoeba Sisters Biomoleculesapi-34233421650% (6)
- DNA EXTRACTION From ANIMAL TISSUESDocument24 pagesDNA EXTRACTION From ANIMAL TISSUESSahara Nesli GonzagaNo ratings yet
- Overview of Biochemical EndocrinologyDocument20 pagesOverview of Biochemical EndocrinologyGauri KashyapNo ratings yet
- BrightStar BioDetect Kit (Ambion)Document15 pagesBrightStar BioDetect Kit (Ambion)espla001No ratings yet
- JERICO JHON SALUDAGA - Physical Science Worksheet 3Document5 pagesJERICO JHON SALUDAGA - Physical Science Worksheet 3JERICO JHON SALUDAGANo ratings yet
- TOP 250 Pharma CompaniesDocument7 pagesTOP 250 Pharma CompaniesadityakhadkeNo ratings yet
- PhetDocument4 pagesPhetCarlos Matute NeavesNo ratings yet
- Neuroreceptor Mechanisms in BrainDocument488 pagesNeuroreceptor Mechanisms in BrainFRANCISCO ELI LEZAMA GUTIERREZNo ratings yet
- Protien ASDocument25 pagesProtien ASRabia RafiqueNo ratings yet
- Cell Organeeles IDocument7 pagesCell Organeeles ISaumya GopalNo ratings yet
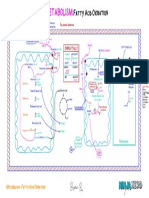
- Fatty Acid Oxidation Part Two Illustration AtfDocument1 pageFatty Acid Oxidation Part Two Illustration AtfDivyaa VisvalingamNo ratings yet
- Cell organelle functions and transport mechanismsDocument10 pagesCell organelle functions and transport mechanismsjuju on the beatNo ratings yet
- Baculogold Rbaculovirus ProtocolDocument2 pagesBaculogold Rbaculovirus Protocolk swetha kumariNo ratings yet
- Sentence Outline ExampleDocument7 pagesSentence Outline ExampleOneil Shuga Stick Martin100% (2)
- IPR For BiotechnologyDocument7 pagesIPR For BiotechnologynovaNo ratings yet
- Fundamentals of Immunology - Death by Friendly FireDocument145 pagesFundamentals of Immunology - Death by Friendly FireAngel FeresiaNo ratings yet
- Membership StatewiseDocument16 pagesMembership StatewiseMithilesh VaddadiNo ratings yet
- Chemical Synthesis of Oligonucleotides PDFDocument12 pagesChemical Synthesis of Oligonucleotides PDFMuhammad AhmedNo ratings yet
- Genbio 2Document4 pagesGenbio 2Mhariane MabborangNo ratings yet
- Bacterial Transformation LabDocument11 pagesBacterial Transformation Labapi-306568509100% (1)
- Introduction To Cns PharmacologyDocument40 pagesIntroduction To Cns Pharmacologydave_11280% (1)
- ID LncRNA CARD8-AS1Document8 pagesID LncRNA CARD8-AS1Samuel Salinas AguirreNo ratings yet
- Genetics and Plant Breeding Question BankDocument4 pagesGenetics and Plant Breeding Question BankVivek Ponnusamy50% (2)
- RNA Structure and FunctionsDocument13 pagesRNA Structure and FunctionsalexlagerhoffNo ratings yet
- Acceptance LetterDocument3 pagesAcceptance LetterRufaq UllahNo ratings yet
- Biochem Lec Transes (Week 4)Document6 pagesBiochem Lec Transes (Week 4)Juren LasagaNo ratings yet
- AP Bio Unit 4 FRQDocument8 pagesAP Bio Unit 4 FRQJiyo ChangNo ratings yet
- Bioprocessing Solutions: Rapid Analytical Solutions For In-Process and Lot-Release TestingDocument13 pagesBioprocessing Solutions: Rapid Analytical Solutions For In-Process and Lot-Release TestingrezaNo ratings yet
- Environmental Microbiology and BiotechnologyDocument20 pagesEnvironmental Microbiology and BiotechnologyRuben MarquezNo ratings yet