You might also like
- The OTC Handbook: Allergy, Cough, Cold Medicine Advice Book. Medication Guide for symptoms related to Flu, GI, Skin & MORE!From EverandThe OTC Handbook: Allergy, Cough, Cold Medicine Advice Book. Medication Guide for symptoms related to Flu, GI, Skin & MORE!No ratings yet
- AAP Emergencies Ped Drug Doses PDFDocument20 pagesAAP Emergencies Ped Drug Doses PDFUlvionaNo ratings yet
- MILVv 10 N2Document3 pagesMILVv 10 N2garywall.ukNo ratings yet
- ASCIA Allergic Rhinitis Treatment Plan 2017 PDFDocument1 pageASCIA Allergic Rhinitis Treatment Plan 2017 PDFdregleavNo ratings yet
- ASCIA Allergic Rhinitis Treatment Plan 2017Document1 pageASCIA Allergic Rhinitis Treatment Plan 2017dregleavNo ratings yet
- FluticasoneDocument4 pagesFluticasonevanNo ratings yet
- EpinephrineDocument4 pagesEpinephrinegovind_soni_15No ratings yet
- Antiemetic Drug Use in Children What The.3Document6 pagesAntiemetic Drug Use in Children What The.3Zafitri AsrulNo ratings yet
- Basicsof Managementof Medical Emergenciesin Dental Officeand Emergency Drug KitDocument7 pagesBasicsof Managementof Medical Emergenciesin Dental Officeand Emergency Drug KitMahmoud TayseerNo ratings yet
- ASCIA Allergic Rhinitis Treatment Plan 2020Document1 pageASCIA Allergic Rhinitis Treatment Plan 2020BigPharma HealtcareNo ratings yet
- MILV8N8Document4 pagesMILV8N8garywall.ukNo ratings yet
- AtropinDocument9 pagesAtropinarfitaaaaNo ratings yet
- Eye Drops DefinitionDocument8 pagesEye Drops DefinitionEileen OoiNo ratings yet
- Airway Block DR HTDocument20 pagesAirway Block DR HTgheaastridgayatriNo ratings yet
- Pharmacology - Day 2 AssignmentDocument2 pagesPharmacology - Day 2 AssignmentStacey GwenNo ratings yet
- 37697239Document7 pages37697239DwityaOktinaDewiNo ratings yet
- 1920s Doctor's Bag 2Document9 pages1920s Doctor's Bag 2Stefan NowakowskiNo ratings yet
- Kasus Injeksi EpinephrinDocument3 pagesKasus Injeksi EpinephrinLilis MusthainahNo ratings yet
- Dentistry EmergenciesDocument5 pagesDentistry EmergenciesSofia PereiraNo ratings yet
- Pediatric Medical Emergencies Rev Oct 2016Document27 pagesPediatric Medical Emergencies Rev Oct 2016ElvisNo ratings yet
- Oral SurgeryDocument15 pagesOral Surgeryyahia salahNo ratings yet
- Allergic Disorders: Drugs ForDocument16 pagesAllergic Disorders: Drugs ForEliza SparkNo ratings yet
- Should Be Available at All Sites If Feasible, Include at Sites (Not Required)Document5 pagesShould Be Available at All Sites If Feasible, Include at Sites (Not Required)Ahmed QlhamdNo ratings yet
- HypersalivationDocument2 pagesHypersalivationosteoporosisclinicNo ratings yet
- Ambulance Pocket BookDocument36 pagesAmbulance Pocket BooknapoleonmNo ratings yet
- Understanding Emergency Equipment in DENTISTRYDocument15 pagesUnderstanding Emergency Equipment in DENTISTRYZahid AhmadNo ratings yet
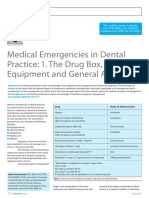
- Dent Update 2009 36 202-211Document6 pagesDent Update 2009 36 202-211Talal MazharNo ratings yet
- FUNDA Drug Computation AcenaDocument104 pagesFUNDA Drug Computation AcenaLawrence HanNo ratings yet
- Anaphylaxis Guidance CardsDocument2 pagesAnaphylaxis Guidance CardsElein Datu SeruNo ratings yet
- Table 1: Daniel - Haas@utoronto - Ca Other Sections I. Essential Emergency Drugs Ii. Additional Drugs ReferencesDocument6 pagesTable 1: Daniel - Haas@utoronto - Ca Other Sections I. Essential Emergency Drugs Ii. Additional Drugs ReferencesBasamat Ahmed SharfNo ratings yet
- Allergology InternationalDocument9 pagesAllergology Internationalvijay dagdiNo ratings yet
- Farmacos Emergencias MedicasDocument11 pagesFarmacos Emergencias MedicasAngélica Valenzuela AndrighiNo ratings yet
- Cabasis Drug StudyDocument3 pagesCabasis Drug StudyNick James CabasisNo ratings yet
- Crash Cart Supplies and DrugsDocument3 pagesCrash Cart Supplies and DrugsShrutiNo ratings yet
- Long-Acting Injectable AntipsychoticsDocument5 pagesLong-Acting Injectable AntipsychoticsDragutin PetrićNo ratings yet
- Long-Acting Injectable AntipsychoticsDocument5 pagesLong-Acting Injectable AntipsychoticsSiegfried CristoforNo ratings yet
- Case Study - LucyDocument10 pagesCase Study - LucykenataNo ratings yet
- Annex To The European Commission Guideline On Excipients in The Labelling and Package Leaflet of Medicinal Products For Human Use' (2019)Document21 pagesAnnex To The European Commission Guideline On Excipients in The Labelling and Package Leaflet of Medicinal Products For Human Use' (2019)janoscribdNo ratings yet
- Lab Activity PcolDocument15 pagesLab Activity PcolHannah VueltaNo ratings yet
- Drug Box ReviewDocument35 pagesDrug Box ReviewJustin MagillNo ratings yet
- Medical Management of Vaccine Reactions in Adults in A Community SettingDocument2 pagesMedical Management of Vaccine Reactions in Adults in A Community SettingByeah SansNo ratings yet
- The Most Common Drugs Used in The EarDocument4 pagesThe Most Common Drugs Used in The EarAzizurahmanNo ratings yet
- AdrenalineDocument2 pagesAdrenalinerazvan032006100% (1)
- Medical Emergencies: Made By: Nitin Shishodia B.D.S - Iii YearDocument29 pagesMedical Emergencies: Made By: Nitin Shishodia B.D.S - Iii YearDrNagendra Dutt SharmaNo ratings yet
- Allergology InternationalDocument9 pagesAllergology InternationalTazrian FarahNo ratings yet
- Anaph 5Document7 pagesAnaph 5Aprilihardini Laksmi100% (1)
- Anaphylaxis Wallchart 2018Document1 pageAnaphylaxis Wallchart 2018simranNo ratings yet
- GNU DOH Compliance Monitoring Sheet 1Document2 pagesGNU DOH Compliance Monitoring Sheet 1Sherilyn RodriguezNo ratings yet
- Emergency Tray PesentationDocument14 pagesEmergency Tray Pesentationgaladimawa2002No ratings yet
- AnticipatoryDocument8 pagesAnticipatorypkx5rgzrdwNo ratings yet
- Cara Membuat PUSH DOSE EpiDocument2 pagesCara Membuat PUSH DOSE EpiRoy LiemNo ratings yet
- Awake Fiber-Optic BronchosDocument60 pagesAwake Fiber-Optic BronchosManisha SagarNo ratings yet
- Pediatrics 1998 E13Document20 pagesPediatrics 1998 E13Jelai ParaisoNo ratings yet
- Anaphylaxis Articulo CompletoDocument6 pagesAnaphylaxis Articulo CompletoFrancelia Quiñonez RuvalcabaNo ratings yet
- Adecelin InjeksiDocument17 pagesAdecelin InjeksianipratiwiNo ratings yet
- Doctor Bag in 1920sDocument3 pagesDoctor Bag in 1920sMiguelDerasNo ratings yet
- The Crash CartDocument39 pagesThe Crash Cartpramod kumawat100% (1)
- Other Sections : Table 1Document5 pagesOther Sections : Table 1sandeepramanuj4No ratings yet
- Labelling FINALDocument10 pagesLabelling FINALpasupuleti familyNo ratings yet
- Inadvertent IV Administration of Epi and Not IMDocument4 pagesInadvertent IV Administration of Epi and Not IMsmith.kevin1420344No ratings yet
- Emsa Regs 2020 12 15Document195 pagesEmsa Regs 2020 12 15smith.kevin1420344No ratings yet
- 1-25 - EIB - ESB - Handbook - Final 2022Document98 pages1-25 - EIB - ESB - Handbook - Final 2022smith.kevin1420344No ratings yet
- 23-005A AMCAS Applicant Guide-FINAL.4 With Cover - AccessibleDocument104 pages23-005A AMCAS Applicant Guide-FINAL.4 With Cover - AccessibleAnge MarieNo ratings yet
- 5 - EIB Tasks CurrentDocument2 pages5 - EIB Tasks Currentsmith.kevin1420344No ratings yet
- Nfpa 1582 Examenes OcupacionalesDocument122 pagesNfpa 1582 Examenes Ocupacionalesabel0066No ratings yet
- Impacts of California Senate Bill 1152 On Homeless Discharge ProtocolDocument14 pagesImpacts of California Senate Bill 1152 On Homeless Discharge Protocolsmith.kevin1420344No ratings yet
- Nato SofDocument70 pagesNato Sofsmith.kevin1420344No ratings yet
- Wood - Army.mil JIJ4KA6EYARR2A6C5BA3ZNJJUA25ZG7ADocument41 pagesWood - Army.mil JIJ4KA6EYARR2A6C5BA3ZNJJUA25ZG7Asmith.kevin1420344No ratings yet
- Usaa 059Document4 pagesUsaa 059smith.kevin1420344No ratings yet
- Prehospitaltriageformasscasaultiesvol 2 Chapter 31Document9 pagesPrehospitaltriageformasscasaultiesvol 2 Chapter 31smith.kevin1420344No ratings yet
- EvolutionCombatMedic 2022Document17 pagesEvolutionCombatMedic 2022smith.kevin1420344100% (1)
- Emscommandorientation 2017Document37 pagesEmscommandorientation 2017smith.kevin1420344No ratings yet
- Mash FMDocument10 pagesMash FMsmith.kevin1420344No ratings yet
- MASH AppDocument4 pagesMASH Appsmith.kevin1420344No ratings yet
- Afh33 337 PDFDocument370 pagesAfh33 337 PDFTrader EliteNo ratings yet
- MASH CH 6Document56 pagesMASH CH 6smith.kevin1420344No ratings yet
- NurseCorps Part 5Document24 pagesNurseCorps Part 5smith.kevin1420344No ratings yet
- MASH CH 7Document30 pagesMASH CH 7smith.kevin1420344No ratings yet
- NurseCorps Part 10Document36 pagesNurseCorps Part 10smith.kevin1420344No ratings yet
- MASH CH 2Document30 pagesMASH CH 2smith.kevin1420344No ratings yet
- NurseCorps Part 4Document20 pagesNurseCorps Part 4smith.kevin1420344No ratings yet
- 68w Chapter 05Document28 pages68w Chapter 05smith.kevin1420344No ratings yet
- Govpub D101Document4 pagesGovpub D101smith.kevin1420344No ratings yet
- EMF Procedural Checklists (2021-2022)Document21 pagesEMF Procedural Checklists (2021-2022)smith.kevin1420344No ratings yet
- D D I 6130.03 M S A, E, I M SDocument49 pagesD D I 6130.03 M S A, E, I M Snour abdallaNo ratings yet
- 68w Chapter 01 - RevDocument7 pages68w Chapter 01 - Revsmith.kevin1420344No ratings yet
- 68w Chapter 02 - Rev - 09-13-22Document11 pages68w Chapter 02 - Rev - 09-13-22smith.kevin1420344No ratings yet
- 68W Perform A Medical Patient AssessmentDocument6 pages68W Perform A Medical Patient Assessmentsmith.kevin1420344No ratings yet
- Top Messages: Paediatric Life Support 2021Document6 pagesTop Messages: Paediatric Life Support 2021Mihai Ion GhioaldaNo ratings yet
- E003335 Full PDFDocument3 pagesE003335 Full PDFOmer FarooqNo ratings yet
- Burns Protocol PDFDocument18 pagesBurns Protocol PDFSai MaryNo ratings yet
- Basic Life Support Ncort HPD 2015Document31 pagesBasic Life Support Ncort HPD 2015lufiasNo ratings yet
- ASHI ACLS Form Field FlyerDocument1 pageASHI ACLS Form Field FlyerErwin RomeroNo ratings yet
- Ambulance BrochureDocument2 pagesAmbulance Brochureapi-494939117No ratings yet
- G, HJDocument5 pagesG, HJArif Rahman HakimNo ratings yet
- Ambulance InventoryDocument2 pagesAmbulance InventoryScarlet Marie CiubalNo ratings yet
- Umass Lowell PCRDocument1 pageUmass Lowell PCRdandude505No ratings yet
- E202 Medical Assessment PDFDocument1 pageE202 Medical Assessment PDFSyahidatul Kautsar NajibNo ratings yet
- Emergency Rescue DrillDocument13 pagesEmergency Rescue DrillbalasubramaniamNo ratings yet
- Emr Policy and ProcedureDocument7 pagesEmr Policy and Procedureapi-267965870No ratings yet
- 7mosby's EMT-Basic Textbook - Revised Reprint, 2nd EditionDocument22 pages7mosby's EMT-Basic Textbook - Revised Reprint, 2nd EditionKathrina AlfonsoNo ratings yet
- Paula Johnson Resume Updated 11-2014Document8 pagesPaula Johnson Resume Updated 11-2014pjohnson181No ratings yet
- Wilderness First Responder, W-EMT Module CourseDocument3 pagesWilderness First Responder, W-EMT Module CourseWilderness Medicine OutfittersNo ratings yet
- 8 - 4 Emd Comb Water and DrainageDocument3 pages8 - 4 Emd Comb Water and DrainageAcar Hakan BayramoğluNo ratings yet
- OEC Chapter 4Document10 pagesOEC Chapter 4Phil McLeanNo ratings yet
- Chapter 1Document27 pagesChapter 1Neil Adonis UsaragaNo ratings yet
- Basic (Level IV) Trauma Facility CriteriaDocument6 pagesBasic (Level IV) Trauma Facility CriteriaPiet Pogen PoelNo ratings yet
- Afghanistan Medical ResourcesDocument4 pagesAfghanistan Medical ResourcesJames GribbenNo ratings yet
- 9 12-OumDocument9 pages9 12-OumAre HidayuNo ratings yet
- Bookshelf NBK305685Document456 pagesBookshelf NBK305685taucci123No ratings yet
- My ResumeDocument3 pagesMy Resumeapi-283324936No ratings yet
- CV & Lampiran Usman Abdul Aziz 2022Document7 pagesCV & Lampiran Usman Abdul Aziz 2022Oezm-mhan JocamerzNo ratings yet
- Fire Safety Knowledge and Practices Among Residents of An Assisted Living FacilityDocument5 pagesFire Safety Knowledge and Practices Among Residents of An Assisted Living FacilityNorma Alejandra AbrenaNo ratings yet
- Committee On Trauma Presents: Thermal InjuriesDocument35 pagesCommittee On Trauma Presents: Thermal InjuriesAlfina Aulia RizkiNo ratings yet
- U L S E C - Usls Bl1-P: Ltrasound IFE Upport Ntry OurseDocument9 pagesU L S E C - Usls Bl1-P: Ltrasound IFE Upport Ntry Oursesaraswaty710No ratings yet
- Smart Technology Ambulance..Document12 pagesSmart Technology Ambulance..Aarya RatnaparkhiNo ratings yet
- First Aid Box Inspection Checklist-NewDocument16 pagesFirst Aid Box Inspection Checklist-NewSafety DeptNo ratings yet
- A Modeling Framework For Facility Location of Medical Services For Large Scale Emergencies PDFDocument16 pagesA Modeling Framework For Facility Location of Medical Services For Large Scale Emergencies PDFiV32No ratings yet