You might also like
- Tut - Implantable and Ingestible Antenna Systems From Imagination To Realization BioelectromagneticsDocument14 pagesTut - Implantable and Ingestible Antenna Systems From Imagination To Realization BioelectromagneticsJAYESH HARLALKANo ratings yet
- R - Implantable Antennas For Bio-Medical ApplicationsDocument13 pagesR - Implantable Antennas For Bio-Medical ApplicationsJAYESH HARLALKANo ratings yet
- Implantable Antennas For Bio-Medical ApplicationsDocument14 pagesImplantable Antennas For Bio-Medical ApplicationsPratik GundigaraNo ratings yet
- Implantable Antennas For Bio-Medical ApplicationsDocument16 pagesImplantable Antennas For Bio-Medical ApplicationseladNo ratings yet
- A Comprehensive Review of In-Body Biomedical Antennas Design, Challenges and Applications - Micromachines-14-01472-V3-1Document4 pagesA Comprehensive Review of In-Body Biomedical Antennas Design, Challenges and Applications - Micromachines-14-01472-V3-1Generation GenerationNo ratings yet
- RF, and Microwaves in Medicine and Biology, (Doi:: 10.1109/JERM.2020.3026588Document16 pagesRF, and Microwaves in Medicine and Biology, (Doi:: 10.1109/JERM.2020.3026588Generation GenerationNo ratings yet
- Enabling Technologies for Emerging Bioelectromagnetics ApplicationsDocument28 pagesEnabling Technologies for Emerging Bioelectromagnetics ApplicationsGoutham N GowdaNo ratings yet
- A Comprehensive Review of In-Body Biomedical Antennas Design, Challenges and Applications - Micromachines-14-01472-V3Document1 pageA Comprehensive Review of In-Body Biomedical Antennas Design, Challenges and Applications - Micromachines-14-01472-V3Generation GenerationNo ratings yet
- 07879807Document28 pages07879807Sharmili Nukapeyi NNo ratings yet
- Integrated Circuits and Electrode Interfaces For Noninvasive Physiological Monitoring 2014 5GDocument16 pagesIntegrated Circuits and Electrode Interfaces For Noninvasive Physiological Monitoring 2014 5GnailsssNo ratings yet
- Dual-Band Two-Port MIMO Antenna For Biomedical Deep Tissue Communication Design Characterization and Performance AnalysisDocument11 pagesDual-Band Two-Port MIMO Antenna For Biomedical Deep Tissue Communication Design Characterization and Performance AnalysisJamal Abdul NasyirNo ratings yet
- Intelligent Security Performance Prediction For Iot-Enabled Healthcare Networks Using Improved CNNDocument10 pagesIntelligent Security Performance Prediction For Iot-Enabled Healthcare Networks Using Improved CNNMoin SyedNo ratings yet
- Ap2108 1659Document1 pageAp2108 1659Generation GenerationNo ratings yet
- A Review On Antennas For Biomedical Implants Used For Iot Based Health CareDocument9 pagesA Review On Antennas For Biomedical Implants Used For Iot Based Health CarerezaNo ratings yet
- 1-s2.0-S266591742300185X-mainDocument11 pages1-s2.0-S266591742300185X-maindatapot465No ratings yet
- Final Year Project Proposal: Project Title: Early Warning and Health Monitoring System Using Wireless Sensor NetworksDocument7 pagesFinal Year Project Proposal: Project Title: Early Warning and Health Monitoring System Using Wireless Sensor NetworksMaryam BabarNo ratings yet
- A Compact Implantable MIMO Antenna For High-Data-Rate Biotelemetry ApplicationsDocument10 pagesA Compact Implantable MIMO Antenna For High-Data-Rate Biotelemetry Applicationsgf.msaniNo ratings yet
- Design of A Wearable MIMO Antenna Deployed With An Inverted U-Shaped Ground Stub For Diversity Performance EnhancementDocument11 pagesDesign of A Wearable MIMO Antenna Deployed With An Inverted U-Shaped Ground Stub For Diversity Performance EnhancementengrkskNo ratings yet
- 2010-Wireless Sensor Network Based E-Health SystemDocument8 pages2010-Wireless Sensor Network Based E-Health Systemsm2nictNo ratings yet
- SIM HUMaLaOR2Document17 pagesSIM HUMaLaOR2Avishek ChakrabortyNo ratings yet
- Irs IsacDocument37 pagesIrs IsacOsama AL TayarNo ratings yet
- Flexible Tri-Band Dual-Polarized MIMO Belt Strap Antenna Toward Wearable Applications in Intelligent Internet of Medical ThingsDocument12 pagesFlexible Tri-Band Dual-Polarized MIMO Belt Strap Antenna Toward Wearable Applications in Intelligent Internet of Medical Thingsgf.msaniNo ratings yet
- KGiSL ECE Project Reviews MyMedi Post Hospital Monitoring SystemDocument14 pagesKGiSL ECE Project Reviews MyMedi Post Hospital Monitoring SystemRAHUL BTNo ratings yet
- The Internet of Things For Applications in WearablDocument17 pagesThe Internet of Things For Applications in WearablTanay JainNo ratings yet
- Investigation On Wireless Link For Medical Telemetry Including Impedance Matching of Implanted Antennas - Sensors-21-01431-V3Document17 pagesInvestigation On Wireless Link For Medical Telemetry Including Impedance Matching of Implanted Antennas - Sensors-21-01431-V3Generation GenerationNo ratings yet
- Liu 2020Document10 pagesLiu 2020Sofia BouchenakNo ratings yet
- Towards Smart Wireless Communications Via Intelligent Reflecting Surfaces: A Contemporary SurveyDocument33 pagesTowards Smart Wireless Communications Via Intelligent Reflecting Surfaces: A Contemporary SurveyKhánh lêNo ratings yet
- Sar at Near DistanceDocument11 pagesSar at Near DistanceShashi KumarNo ratings yet
- Biometric Behavior Authentication Exploiting Propagation Characteristics of Wireless ChannelDocument8 pagesBiometric Behavior Authentication Exploiting Propagation Characteristics of Wireless ChannelFizaNo ratings yet
- A Bimodal Detection-Based Tremor Suppression System For Vascular Interventional Surgery RobotsDocument13 pagesA Bimodal Detection-Based Tremor Suppression System For Vascular Interventional Surgery RobotsAbdulkareem 99No ratings yet
- Smartphone-Based Pedestrian NLOS Positioning Based On Acoustics and IMU Parameter EstimationDocument14 pagesSmartphone-Based Pedestrian NLOS Positioning Based On Acoustics and IMU Parameter Estimationelaheh.hassanzadeh6No ratings yet
- Experimental Investigation of 3-D Human Body Localization Using Wearable Ultra-Wideband AntennasDocument10 pagesExperimental Investigation of 3-D Human Body Localization Using Wearable Ultra-Wideband AntennasPadmavathy VelayudhamNo ratings yet
- Engineering The Internet of Things: Wearables and Medical DevicesDocument4 pagesEngineering The Internet of Things: Wearables and Medical DevicesOscar ChilcaNo ratings yet
- Wireless Sensor Networks Application Centric DesignDocument504 pagesWireless Sensor Networks Application Centric Designaminkhan830% (1)
- Wireless Body Area Network Research PapersDocument6 pagesWireless Body Area Network Research Paperslxeikcvnd100% (1)
- Synopsys Wearable RajkumarDocument17 pagesSynopsys Wearable RajkumarrajkumarNo ratings yet
- Recent Advances in Communications and IT TechnologiesDocument6 pagesRecent Advances in Communications and IT Technologiessurajpb1989No ratings yet
- 00tmc00-Santagati-2561277.pdf - 7463487-AamDocument1 page00tmc00-Santagati-2561277.pdf - 7463487-AamGeneration GenerationNo ratings yet
- 7251-Article Text-12948-1-10-20210607Document7 pages7251-Article Text-12948-1-10-20210607Generation GenerationNo ratings yet
- Wireless Body Area Network (WBAN) : A Survey On Architecture, Technologies, Energy Consumption, and Security ChallengesDocument34 pagesWireless Body Area Network (WBAN) : A Survey On Architecture, Technologies, Energy Consumption, and Security ChallengesNischal KataraNo ratings yet
- Wireless Technologies For Implantable DevicesDocument19 pagesWireless Technologies For Implantable DevicesSaran SNo ratings yet
- Final PresentationDocument34 pagesFinal PresentationVaishali WaghmodeNo ratings yet
- Design & Simulation of Optical Fiber Bragg Grating Pressure Sensor For Minimum Attenuation CriteriaDocument16 pagesDesign & Simulation of Optical Fiber Bragg Grating Pressure Sensor For Minimum Attenuation CriteriaSaverio AvinoNo ratings yet
- Acousto-Optic Catheter Tracking Sensor For Interventional MRI ProceduresDocument7 pagesAcousto-Optic Catheter Tracking Sensor For Interventional MRI ProceduresasifnewazuccNo ratings yet
- Patient Monitoring System Using BeaconDocument7 pagesPatient Monitoring System Using BeaconIJRASETPublicationsNo ratings yet
- RF and Microwave Technology Challenges For Internet-of-Things ApplicationsDocument2 pagesRF and Microwave Technology Challenges For Internet-of-Things Applicationsmmk040891No ratings yet
- A Review On Recent Progress of Portable Short-Range Noncontact Microwave Radar SystemsDocument15 pagesA Review On Recent Progress of Portable Short-Range Noncontact Microwave Radar SystemsAhmed HussainNo ratings yet
- Wireless Sensor NetworksDocument5 pagesWireless Sensor NetworksRubén Isaac Guevara ManzanoNo ratings yet
- Wearable Sensors and ImplantsDocument17 pagesWearable Sensors and ImplantsAhad Ali100% (1)
- Hardware Architecture For Nanorobot Application in Cancer TherapyDocument7 pagesHardware Architecture For Nanorobot Application in Cancer TherapyCynthia CarolineNo ratings yet
- Measurement SensorsDocument6 pagesMeasurement SensorsBeulah JacksonNo ratings yet
- Health Monitoring SystemDocument8 pagesHealth Monitoring SystemElizabeth HarrisNo ratings yet
- Hussain - 2020 - IOP - Conf. - Ser. - Mater. - Sci. - Eng. - 745 - 012087Document2 pagesHussain - 2020 - IOP - Conf. - Ser. - Mater. - Sci. - Eng. - 745 - 012087Generation GenerationNo ratings yet
- Sensing of Life Activities at The Human-Microwave FrontierDocument13 pagesSensing of Life Activities at The Human-Microwave FrontierNicholas FeatherstonNo ratings yet
- Cmos Image SensorDocument14 pagesCmos Image SensorAhmed MosaNo ratings yet
- Published I Eee Access AdelDocument19 pagesPublished I Eee Access AdelZalan RadiNo ratings yet
- Leung 2013Document36 pagesLeung 2013Kim RomanoNo ratings yet
- Integrated Sensing and Communications Toward Dual-Functional Wireless Networks For 6G and BeyondDocument40 pagesIntegrated Sensing and Communications Toward Dual-Functional Wireless Networks For 6G and Beyondaliakber2k10No ratings yet
- A Context-Aware Data Fusion Approach For Health-IoTDocument5 pagesA Context-Aware Data Fusion Approach For Health-IoTAlain Gómez CabreraNo ratings yet
- RF, and Microwaves in Medicine and Biology, (Doi:: 10.1109/JERM.2020.3026588Document16 pagesRF, and Microwaves in Medicine and Biology, (Doi:: 10.1109/JERM.2020.3026588Generation GenerationNo ratings yet
- Torture and The Cruel, Inhuman and Degrading Treatment of Detainees The Effectiveness and Consequences of 'Enhanced' InterrogationDocument39 pagesTorture and The Cruel, Inhuman and Degrading Treatment of Detainees The Effectiveness and Consequences of 'Enhanced' InterrogationGeneration GenerationNo ratings yet
- Wireless Issues and Spectrum ReformDocument107 pagesWireless Issues and Spectrum ReformGeneration GenerationNo ratings yet
- 1 s2.0 S0013935120307854 MainDocument10 pages1 s2.0 S0013935120307854 MainMaya NettaNo ratings yet
- !!!FDAVaccines Can Be Approved Even If They Do Not Prevent Infection or Transmission April 2023Document33 pages!!!FDAVaccines Can Be Approved Even If They Do Not Prevent Infection or Transmission April 2023Generation GenerationNo ratings yet
- Fulltext01Document5 pagesFulltext01Generation GenerationNo ratings yet
- Neurosurg Focus Article PE10 1Document8 pagesNeurosurg Focus Article PE10 1Generation GenerationNo ratings yet
- Fneur 13 880814Document18 pagesFneur 13 880814Generation GenerationNo ratings yet
- ! - Katalog - Gesamt - 2011 - GB - 1.qxd - 1674904Document2 pages! - Katalog - Gesamt - 2011 - GB - 1.qxd - 1674904Generation GenerationNo ratings yet
- Part1 Medical Device Networking For Smarter Healthcare WPDocument1 pagePart1 Medical Device Networking For Smarter Healthcare WPGeneration GenerationNo ratings yet
- Mainstream Brain-Computer Interfaces Are Coming - Just Ask Synchron, Neuralink, Paradromics, and HackerBCIDocument6 pagesMainstream Brain-Computer Interfaces Are Coming - Just Ask Synchron, Neuralink, Paradromics, and HackerBCIGeneration GenerationNo ratings yet
- 246544159-AWY-9400-ManualDocument1 page246544159-AWY-9400-ManualGeneration GenerationNo ratings yet
- A Compact Dual-Band Implantable Antenna For Wireless Biotelemetry in Arteriovenous GraftsDocument1 pageA Compact Dual-Band Implantable Antenna For Wireless Biotelemetry in Arteriovenous GraftsGeneration GenerationNo ratings yet
- Neurosurg Focus Article PE10 1Document8 pagesNeurosurg Focus Article PE10 1Generation GenerationNo ratings yet
- The Missing Manuscript of Dr. Jose Delgado S Radio Controlled Bulls - June-15-R29Document2 pagesThe Missing Manuscript of Dr. Jose Delgado S Radio Controlled Bulls - June-15-R29Generation GenerationNo ratings yet
- Bocan TissueModels IEEESensorsDocument2 pagesBocan TissueModels IEEESensorsGeneration GenerationNo ratings yet
- Diffusion Tensor Imaging, Intra-Operative Neurophysiological Monitoring and Small Craniotomy: Results in A Consecutive Series of 103 GliomasDocument11 pagesDiffusion Tensor Imaging, Intra-Operative Neurophysiological Monitoring and Small Craniotomy: Results in A Consecutive Series of 103 GliomasGeneration GenerationNo ratings yet
- Fneur 13 880814Document18 pagesFneur 13 880814Generation GenerationNo ratings yet
- A High Performance Delta-Sigma Modulator For Neurosensing - Sensors-15-19466-1Document2 pagesA High Performance Delta-Sigma Modulator For Neurosensing - Sensors-15-19466-1Generation GenerationNo ratings yet
- A Compact Wireless Power Transfer System at 915 MHZ With Supercapacitor For Optogenetics Applications - ScienceDirectDocument7 pagesA Compact Wireless Power Transfer System at 915 MHZ With Supercapacitor For Optogenetics Applications - ScienceDirectGeneration GenerationNo ratings yet
- Research Article Small Triple-Band Meandered PIFA For Brain-Implantable Biotelemetric Systems: Development and Testing in A Liquid PhantomDocument1 pageResearch Article Small Triple-Band Meandered PIFA For Brain-Implantable Biotelemetric Systems: Development and Testing in A Liquid PhantomGeneration GenerationNo ratings yet
- Decoding Raw Frames - Generic - Libre Space CommunityDocument7 pagesDecoding Raw Frames - Generic - Libre Space CommunityGeneration GenerationNo ratings yet
- A New Wireless-Enabled Audio Processor For Hearing Aids and Cochlear Implants - NewsDocument7 pagesA New Wireless-Enabled Audio Processor For Hearing Aids and Cochlear Implants - NewsGeneration GenerationNo ratings yet
- A Brief Review On Implantable Antennas FDocument16 pagesA Brief Review On Implantable Antennas FMai VũNo ratings yet
- 802.15.4 Traffic Monitoring (Wireshark) - Troubleshooting - ParticleDocument5 pages802.15.4 Traffic Monitoring (Wireshark) - Troubleshooting - ParticleGeneration GenerationNo ratings yet
- Encore 29901 Programmer and CareLink 2090 Programmer MedtronicDocument7 pagesEncore 29901 Programmer and CareLink 2090 Programmer MedtronicGeneration GenerationNo ratings yet
- Passive Impedance Matching For Implanted Brain-Electrode InterfacesDocument8 pagesPassive Impedance Matching For Implanted Brain-Electrode InterfacesGeneration GenerationNo ratings yet
- Biology and HealthDocument6 pagesBiology and HealthGeneration GenerationNo ratings yet
- A Fully Implantable Wireless ECoG 128-Channel Recording Device For Human Brain-Machine Interfaces W-HERBS - Fnins-12-00511Document11 pagesA Fully Implantable Wireless ECoG 128-Channel Recording Device For Human Brain-Machine Interfaces W-HERBS - Fnins-12-00511Generation GenerationNo ratings yet
- Bypassing Software Update Package Encryption - Extracting The Lexmark MC3224i Printer Rmware (Part 1)Document38 pagesBypassing Software Update Package Encryption - Extracting The Lexmark MC3224i Printer Rmware (Part 1)Generation GenerationNo ratings yet
- CD-BA1500H: Service ManualDocument52 pagesCD-BA1500H: Service ManualmrudzinskasNo ratings yet
- Validation of The FLIGHTLAB - Virtual Engineering Toolset by RonDocument37 pagesValidation of The FLIGHTLAB - Virtual Engineering Toolset by RonAnubhavNo ratings yet
- Grounding or Earthing Scheme in DCS or PLC Systems (39Document3 pagesGrounding or Earthing Scheme in DCS or PLC Systems (39Vraja KisoriNo ratings yet
- ExercisesDocument11 pagesExercisestomrannosaurusNo ratings yet
- Department of Electrical Engineering EE-211: Electrical Network Analysis Lab 7: Capacitive Phase Shift and Reactive PowerDocument6 pagesDepartment of Electrical Engineering EE-211: Electrical Network Analysis Lab 7: Capacitive Phase Shift and Reactive PowerWaleed BajwaNo ratings yet
- KSEB Technical SPec PDFDocument279 pagesKSEB Technical SPec PDFTravis WoodNo ratings yet
- 1.5 Inverse Functions & LogarithmsDocument11 pages1.5 Inverse Functions & Logarithms郭大維No ratings yet
- Exhaust Base Vam Tonnage CalculationDocument9 pagesExhaust Base Vam Tonnage CalculationMagical RiyaNo ratings yet
- TSD-3Document3 pagesTSD-3Deepankar Sadhan BanikNo ratings yet
- Koordinasi Proteksi Saluran Udara TinggiDocument68 pagesKoordinasi Proteksi Saluran Udara TinggiHendy KurniawanNo ratings yet
- Premium Industrial NDT SolutionsDocument16 pagesPremium Industrial NDT SolutionsSiva ShankarNo ratings yet
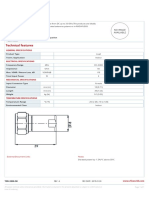
- Technical Features: Load, N Male, 2 WattDocument1 pageTechnical Features: Load, N Male, 2 WattLuciano Silvério LeiteNo ratings yet
- NEET-CHEMISTRY-VOL-III 14TH GROUP ELEMENTSDocument16 pagesNEET-CHEMISTRY-VOL-III 14TH GROUP ELEMENTSkrish masterjeeNo ratings yet
- International Standard: Norme InternationaleDocument11 pagesInternational Standard: Norme InternationaleĐức Huấn ĐỗNo ratings yet
- 01 Service Manual SV600 V4.0 enDocument384 pages01 Service Manual SV600 V4.0 enLuis Felipe Romero100% (3)
- Lighting SystemsDocument67 pagesLighting SystemsSuzette BinongcalNo ratings yet
- EDC DTS MV015 Earthing EquipmentDocument53 pagesEDC DTS MV015 Earthing EquipmentJoe bilouteNo ratings yet
- Auto-Tuning Rotor Resistance Identification of Induction Motor Considering Iron LossDocument4 pagesAuto-Tuning Rotor Resistance Identification of Induction Motor Considering Iron LossNickNo ratings yet
- Andersen 2009Document23 pagesAndersen 2009Lucas MartinsNo ratings yet
- Mechanical Professional ElectiveDocument310 pagesMechanical Professional ElectivearunrajNo ratings yet
- B.E./B.Tech. Course File: St. Xavier's Catholic College of EngineeringDocument25 pagesB.E./B.Tech. Course File: St. Xavier's Catholic College of EngineeringMICHEL RAJ MechNo ratings yet
- RRZZVV-65B-R6H4: Electrical SpecificationsDocument5 pagesRRZZVV-65B-R6H4: Electrical SpecificationsСтанислав НиколовNo ratings yet
- FM2 (4th) May2019Document2 pagesFM2 (4th) May2019Parminder SinghNo ratings yet
- NWJ s2 Yousra ZghoundiDocument10 pagesNWJ s2 Yousra ZghoundioussamaNo ratings yet
- Gaussian Pulse PropagationDocument3 pagesGaussian Pulse PropagationfawalNo ratings yet
- Usman Public School System: Class ViiiDocument1 pageUsman Public School System: Class ViiiZaib ZaibNo ratings yet
- Curriculum Vitae: Hamad MushtaqDocument3 pagesCurriculum Vitae: Hamad MushtaqUzair IjazNo ratings yet
- Inversor Monofasico Puente Completo PDFDocument3 pagesInversor Monofasico Puente Completo PDFAlexander Jimenez NivarNo ratings yet
- Power Plant: Better Life Created by SteelDocument4 pagesPower Plant: Better Life Created by SteelAlejandro Jose Garcia FernandezNo ratings yet
- Problem Set #6 AnswersDocument3 pagesProblem Set #6 AnswersStefan BamNo ratings yet
- A Brief History of Time: From the Big Bang to Black HolesFrom EverandA Brief History of Time: From the Big Bang to Black HolesRating: 4 out of 5 stars4/5 (2193)
- Knocking on Heaven's Door: How Physics and Scientific Thinking Illuminate the Universe and the Modern WorldFrom EverandKnocking on Heaven's Door: How Physics and Scientific Thinking Illuminate the Universe and the Modern WorldRating: 3.5 out of 5 stars3.5/5 (64)
- A Beginner's Guide to Constructing the Universe: The Mathematical Archetypes of Nature, Art, and ScienceFrom EverandA Beginner's Guide to Constructing the Universe: The Mathematical Archetypes of Nature, Art, and ScienceRating: 4 out of 5 stars4/5 (51)
- Dark Matter and the Dinosaurs: The Astounding Interconnectedness of the UniverseFrom EverandDark Matter and the Dinosaurs: The Astounding Interconnectedness of the UniverseRating: 3.5 out of 5 stars3.5/5 (69)
- The Physics of God: How the Deepest Theories of Science Explain Religion and How the Deepest Truths of Religion Explain ScienceFrom EverandThe Physics of God: How the Deepest Theories of Science Explain Religion and How the Deepest Truths of Religion Explain ScienceRating: 4.5 out of 5 stars4.5/5 (23)
- The Tao of Physics: An Exploration of the Parallels between Modern Physics and Eastern MysticismFrom EverandThe Tao of Physics: An Exploration of the Parallels between Modern Physics and Eastern MysticismRating: 4 out of 5 stars4/5 (500)
- Quantum Spirituality: Science, Gnostic Mysticism, and Connecting with Source ConsciousnessFrom EverandQuantum Spirituality: Science, Gnostic Mysticism, and Connecting with Source ConsciousnessRating: 4 out of 5 stars4/5 (6)
- Summary and Interpretation of Reality TransurfingFrom EverandSummary and Interpretation of Reality TransurfingRating: 5 out of 5 stars5/5 (5)
- Lost in Math: How Beauty Leads Physics AstrayFrom EverandLost in Math: How Beauty Leads Physics AstrayRating: 4.5 out of 5 stars4.5/5 (125)
- Packing for Mars: The Curious Science of Life in the VoidFrom EverandPacking for Mars: The Curious Science of Life in the VoidRating: 4 out of 5 stars4/5 (1395)
- Black Holes: The Key to Understanding the UniverseFrom EverandBlack Holes: The Key to Understanding the UniverseRating: 4.5 out of 5 stars4.5/5 (13)
- Quantum Physics for Beginners Who Flunked Math And Science: Quantum Mechanics And Physics Made Easy Guide In Plain Simple EnglishFrom EverandQuantum Physics for Beginners Who Flunked Math And Science: Quantum Mechanics And Physics Made Easy Guide In Plain Simple EnglishRating: 4.5 out of 5 stars4.5/5 (18)
- The Magick of Physics: Uncovering the Fantastical Phenomena in Everyday LifeFrom EverandThe Magick of Physics: Uncovering the Fantastical Phenomena in Everyday LifeNo ratings yet
- Quantum Physics: What Everyone Needs to KnowFrom EverandQuantum Physics: What Everyone Needs to KnowRating: 4.5 out of 5 stars4.5/5 (48)
- The Holographic Universe: The Revolutionary Theory of RealityFrom EverandThe Holographic Universe: The Revolutionary Theory of RealityRating: 4.5 out of 5 stars4.5/5 (76)
- The Power of Eight: Harnessing the Miraculous Energies of a Small Group to Heal Others, Your Life, and the WorldFrom EverandThe Power of Eight: Harnessing the Miraculous Energies of a Small Group to Heal Others, Your Life, and the WorldRating: 4.5 out of 5 stars4.5/5 (54)
- Bedeviled: A Shadow History of Demons in ScienceFrom EverandBedeviled: A Shadow History of Demons in ScienceRating: 5 out of 5 stars5/5 (5)
- In Search of Schrödinger’s Cat: Quantum Physics and RealityFrom EverandIn Search of Schrödinger’s Cat: Quantum Physics and RealityRating: 4 out of 5 stars4/5 (380)
- The End of Everything: (Astrophysically Speaking)From EverandThe End of Everything: (Astrophysically Speaking)Rating: 4.5 out of 5 stars4.5/5 (155)
- Midnight in Chernobyl: The Story of the World's Greatest Nuclear DisasterFrom EverandMidnight in Chernobyl: The Story of the World's Greatest Nuclear DisasterRating: 4.5 out of 5 stars4.5/5 (409)