You might also like
- Sample of Psychological ReportDocument4 pagesSample of Psychological ReportRochelle Joyce Olmilla Bersamin67% (3)
- Scalar Wave Morphogenetic Field Mechanic PDFDocument135 pagesScalar Wave Morphogenetic Field Mechanic PDFMokhtar Mohd100% (7)
- Bowen Family TheoryDocument320 pagesBowen Family Theorytonifieraru100% (14)
- 1000 Calorie ChallengesDocument25 pages1000 Calorie ChallengesFrancesco Iavarone100% (3)
- First Certificate OrganiserDocument212 pagesFirst Certificate OrganiserMarta OsésNo ratings yet
- Antiepileptic Drug Interactions - A Clinical Guide 2nd Ed. (2013)Document464 pagesAntiepileptic Drug Interactions - A Clinical Guide 2nd Ed. (2013)Apróné Török IbolyaNo ratings yet
- Princples of Drug AdministrationDocument90 pagesPrincples of Drug Administrationcoosa liquorsNo ratings yet
- Braden ScaleDocument2 pagesBraden ScaleAJ Tuban CompelioNo ratings yet
- Questions DRDocument8 pagesQuestions DRRosalie Valdez EspirituNo ratings yet
- Fmu Trainging ModuleDocument23 pagesFmu Trainging ModulesamNo ratings yet
- Your Health Book - Sampler by Joseph Pilates PDFDocument28 pagesYour Health Book - Sampler by Joseph Pilates PDFMacsim Alexandra50% (2)
- Pediatrics in ReviewDocument16 pagesPediatrics in ReviewMaria3 Juliao3No ratings yet
- Enoxaparin (Lovenox)Document1 pageEnoxaparin (Lovenox)ENo ratings yet
- Health Regulation of Dietary SupplementsDocument22 pagesHealth Regulation of Dietary SupplementsApróné Török IbolyaNo ratings yet
- IVD Medical Device V2Document44 pagesIVD Medical Device V2Vadi VelanNo ratings yet
- Business Result Reading File 1Document2 pagesBusiness Result Reading File 1Daniela Stroie100% (1)
- CalculationsDocument9 pagesCalculationssantthana100% (1)
- Directions: Choose The Letter of The Correct Answer. Write Your Answer On A Separate Sheet. STRICTLY NO Erasures and Write Capital Letters Only!Document3 pagesDirections: Choose The Letter of The Correct Answer. Write Your Answer On A Separate Sheet. STRICTLY NO Erasures and Write Capital Letters Only!Diane CiprianoNo ratings yet
- Check Unit 555 November Immunology V3 PDFDocument25 pagesCheck Unit 555 November Immunology V3 PDFdragon66No ratings yet
- EndocryneDocument29 pagesEndocryneAlupului AniNo ratings yet
- Jama Shenoy 2019 RV 180010Document12 pagesJama Shenoy 2019 RV 180010GustavoCalderinNo ratings yet
- Type III Hypersensitivity Reaction To Subcutaneous Insulin Preparations in A Type 1 DiabeticDocument5 pagesType III Hypersensitivity Reaction To Subcutaneous Insulin Preparations in A Type 1 DiabeticFeni Nurmia PutriNo ratings yet
- Fimmu 08 01472Document11 pagesFimmu 08 01472Mohammed GazoNo ratings yet
- 10 1111@pan 13703Document9 pages10 1111@pan 13703vladvladut112No ratings yet
- Insulin Allergy Can Be Successfully Managed by A Systematic ApproachDocument6 pagesInsulin Allergy Can Be Successfully Managed by A Systematic Approachjames antonyNo ratings yet
- OIT BurksDocument8 pagesOIT Burksa1765874No ratings yet
- Analysis: The Antibiotic Course Has Had Its DayDocument5 pagesAnalysis: The Antibiotic Course Has Had Its Daysimx88No ratings yet
- DM Tipo1Document15 pagesDM Tipo1SixtoIñaguazoNo ratings yet
- HHS Public Access: Controversies in Drug Allergy: Testing For Delayed ReactionsDocument16 pagesHHS Public Access: Controversies in Drug Allergy: Testing For Delayed ReactionsВалерия НикитинаNo ratings yet
- The Link Between The Clinical Features o PDFDocument2 pagesThe Link Between The Clinical Features o PDFwulanNo ratings yet
- HHS Public Access: Food Allergy: Immune Mechanisms, Diagnosis and ImmunotherapyDocument43 pagesHHS Public Access: Food Allergy: Immune Mechanisms, Diagnosis and ImmunotherapyLeonardo AzevedoNo ratings yet
- Clinical Practice: Drug Desensitization in ChildrenDocument5 pagesClinical Practice: Drug Desensitization in ChildrenangsetNo ratings yet
- Bjgpopen17x100653 FullDocument3 pagesBjgpopen17x100653 Fullaulia nurNo ratings yet
- Togias 2017Document16 pagesTogias 2017Jessica LópezNo ratings yet
- Ranitidine DoseDocument1 pageRanitidine Dosejaka SusilaNo ratings yet
- Association of Food and Drug Allergy With Anti-Tuberculosis Drug Related Hepatitis or Skin Reactions: A Case Control StudyDocument6 pagesAssociation of Food and Drug Allergy With Anti-Tuberculosis Drug Related Hepatitis or Skin Reactions: A Case Control StudyPutri YingNo ratings yet
- ASCIA HP Clinical Update Antibiotic Allergy 2014Document6 pagesASCIA HP Clinical Update Antibiotic Allergy 2014kkkssbbNo ratings yet
- AIJPMS - Volume 3 - Issue 1 - Pages 96-104Document9 pagesAIJPMS - Volume 3 - Issue 1 - Pages 96-104Eman MahmoudNo ratings yet
- Antibiotic Allergy When To Test Challenge or Desensitise 2161 0703 1000234Document7 pagesAntibiotic Allergy When To Test Challenge or Desensitise 2161 0703 1000234Heba HanyNo ratings yet
- Diagnostics 12 01681Document13 pagesDiagnostics 12 01681dhayson silveiraNo ratings yet
- Probiotics For Children With Type 1 DiabetesDocument9 pagesProbiotics For Children With Type 1 DiabetesMahesh JayaramanNo ratings yet
- Kushchayeva 2019Document13 pagesKushchayeva 2019pelinNo ratings yet
- High-Dose Versus Standard-Dose Amoxicillin/ Clavulanate For Clinically-Diagnosed Acute Bacterial Sinusitis: A Randomized Clinical TrialDocument15 pagesHigh-Dose Versus Standard-Dose Amoxicillin/ Clavulanate For Clinically-Diagnosed Acute Bacterial Sinusitis: A Randomized Clinical TrialHendra EfendiNo ratings yet
- 2011 NIAIDSponsored 2010 Guidelines For Managing Food Allergy Applications in The Pediatric PopulationDocument13 pages2011 NIAIDSponsored 2010 Guidelines For Managing Food Allergy Applications in The Pediatric PopulationLily ChandraNo ratings yet
- HipersensibilitateDocument6 pagesHipersensibilitateAndreea RacovitaNo ratings yet
- Epidemiology and Clinical Predictors of Biphasic Reactions in Children With AnaphylaxisDocument9 pagesEpidemiology and Clinical Predictors of Biphasic Reactions in Children With AnaphylaxisPrihanant BayuNo ratings yet
- Alergia A Penicilinas NEJMDocument14 pagesAlergia A Penicilinas NEJMJacinto RamonNo ratings yet
- Oral Presentations 26 September 2019 I7Document2 pagesOral Presentations 26 September 2019 I7dentsavvyNo ratings yet
- Food Allergy Immunotherapy - Oral Immunotherapy andDocument10 pagesFood Allergy Immunotherapy - Oral Immunotherapy anda1765874No ratings yet
- 10 36516-Jocass 1246401-2933495Document5 pages10 36516-Jocass 1246401-2933495yyyyx842No ratings yet
- MIB 0b013e31828f5198Document9 pagesMIB 0b013e31828f5198canaltempolivreNo ratings yet
- Allergy and Related DisordersDocument63 pagesAllergy and Related DisordersavisenicNo ratings yet
- Probiotics in Late Infancy Reduce The Incidence of Eczema: A Randomized Controlled TrialDocument6 pagesProbiotics in Late Infancy Reduce The Incidence of Eczema: A Randomized Controlled TrialarditaNo ratings yet
- Atención de Los Niños Con Alergias A FármacosDocument5 pagesAtención de Los Niños Con Alergias A FármacosHugo RoldanNo ratings yet
- 07 Intravenous Immunoglobulin Replacement Therapy in Children With Primary Immunodeficiency Diseases A Nurse S GuideDocument9 pages07 Intravenous Immunoglobulin Replacement Therapy in Children With Primary Immunodeficiency Diseases A Nurse S GuidekiminoooNo ratings yet
- New Schatz2018 OldDocument44 pagesNew Schatz2018 Oldabhijeet abhijeetNo ratings yet
- Probiotics and Prebiotics in Atopic Dermatitis: Pros and Cons (Review)Document8 pagesProbiotics and Prebiotics in Atopic Dermatitis: Pros and Cons (Review)larissaNo ratings yet
- Olfu Finals BSN ReviewerDocument101 pagesOlfu Finals BSN ReviewerEdnalyn QuimboNo ratings yet
- Food Allergies Current and Future Treatments 2020Document13 pagesFood Allergies Current and Future Treatments 2020KarlaNo ratings yet
- The Management of Peanut Allergy: Katherine Anagnostou, Andrew ClarkDocument6 pagesThe Management of Peanut Allergy: Katherine Anagnostou, Andrew Clarksilvio da costa guerreiroNo ratings yet
- Pediatric Allergy Immunology - 2018 - Kidon - EAACI ENDA Position Paper Diagnosis and Management of HypersensitivityDocument12 pagesPediatric Allergy Immunology - 2018 - Kidon - EAACI ENDA Position Paper Diagnosis and Management of HypersensitivityEdy NoveryNo ratings yet
- Cze-Ja Food Dependent Exercise Induced AnaphylaxisDocument9 pagesCze-Ja Food Dependent Exercise Induced AnaphylaxisOlivia McCuskerNo ratings yet
- Immunotherapy - What Lies BeyondDocument8 pagesImmunotherapy - What Lies BeyondSagar Das ChoudhuryNo ratings yet
- Alergia AlimentariaDocument18 pagesAlergia AlimentariaLUIS PARRANo ratings yet
- Abses PayudaraDocument18 pagesAbses Payudaragastro fkikunibNo ratings yet
- PIIS1939455119301723Document5 pagesPIIS1939455119301723Yeol LoeyNo ratings yet
- Evaluation of Antibiotic Allergy, The Role of Skin TestsDocument9 pagesEvaluation of Antibiotic Allergy, The Role of Skin TestsGilang Sumiarsih PramanikNo ratings yet
- Resistencia A La Insulina - 14-1149239Document24 pagesResistencia A La Insulina - 14-1149239Marcelo TrNo ratings yet
- Evaluation of Antibiotic Sensitivity Pattern in Acute TonsillitisDocument5 pagesEvaluation of Antibiotic Sensitivity Pattern in Acute TonsillitisyoanaNo ratings yet
- Gene Therapy: DiabetesDocument5 pagesGene Therapy: DiabetesIson, Marc Ervin A.No ratings yet
- Insulin Resistance: Childhood Precursors of Adult DiseaseFrom EverandInsulin Resistance: Childhood Precursors of Adult DiseasePhilip S. ZeitlerNo ratings yet
- Adverse Reaction To Amoxicillin: A Case ReportDocument4 pagesAdverse Reaction To Amoxicillin: A Case Reportlia primasariNo ratings yet
- Pruritic Metastatic Crohn'sDocument3 pagesPruritic Metastatic Crohn'sHerald Scholarly Open AccessNo ratings yet
- 323 323 1 PBDocument9 pages323 323 1 PBjimejaikelNo ratings yet
- 1 s2.0 S2376060523001700 MainDocument3 pages1 s2.0 S2376060523001700 MainValentinaNo ratings yet
- Antibiotic Allergy in Pediatrics: A B A, B, C, D, e FDocument17 pagesAntibiotic Allergy in Pediatrics: A B A, B, C, D, e FВалерия НикитинаNo ratings yet
- Inhibition of NR2B Phosphorylation Restores Alterations in NMDA Receptor Expression and Improves Functional Recovery Following Traumatic Brain Injury in Mice (2008)Document13 pagesInhibition of NR2B Phosphorylation Restores Alterations in NMDA Receptor Expression and Improves Functional Recovery Following Traumatic Brain Injury in Mice (2008)Apróné Török IbolyaNo ratings yet
- Intrinsic and Extrinsic Wiring of CA3 - Indications For Connectional Heterogeneity (2007)Document10 pagesIntrinsic and Extrinsic Wiring of CA3 - Indications For Connectional Heterogeneity (2007)Apróné Török IbolyaNo ratings yet
- The Basal Forebrain Cholinergic Projection System in Mice - Chapter 28Document35 pagesThe Basal Forebrain Cholinergic Projection System in Mice - Chapter 28Apróné Török IbolyaNo ratings yet
- Neto1 and Neto2 - Auxiliary Subunits That Determine Key Properties of Native Kainate Receptors (2012)Document7 pagesNeto1 and Neto2 - Auxiliary Subunits That Determine Key Properties of Native Kainate Receptors (2012)Apróné Török IbolyaNo ratings yet
- Exciting Times Beyond The Brain: Metabotropic Glutamate Receptors in Peripheral and Non-Neural TissuesDocument24 pagesExciting Times Beyond The Brain: Metabotropic Glutamate Receptors in Peripheral and Non-Neural TissuesAndi WijayaNo ratings yet
- Neurotransmitter Review (3) - Alcohol and Glutamate (1997)Document8 pagesNeurotransmitter Review (3) - Alcohol and Glutamate (1997)Apróné Török IbolyaNo ratings yet
- Cell Signalling Biology - Ion Channels (2012)Document72 pagesCell Signalling Biology - Ion Channels (2012)Apróné Török IbolyaNo ratings yet
- Zinc Inhibits Protein Synthesis in Neurons (1999)Document6 pagesZinc Inhibits Protein Synthesis in Neurons (1999)Apróné Török IbolyaNo ratings yet
- Natural Products For Neurodegenerative Diseases (Neurosignals) (2005)Document84 pagesNatural Products For Neurodegenerative Diseases (Neurosignals) (2005)Apróné Török IbolyaNo ratings yet
- A Novel Method For Marking Microinjection Sites Using Methylene Blue and Diaminobenzidine (2003)Document5 pagesA Novel Method For Marking Microinjection Sites Using Methylene Blue and Diaminobenzidine (2003)Apróné Török IbolyaNo ratings yet
- List of ContributorsDocument776 pagesList of ContributorsApróné Török IbolyaNo ratings yet
- Structure, Function, and Plasticity of Hippocampal Dentate Gyrus Microcircuits (2015)Document134 pagesStructure, Function, and Plasticity of Hippocampal Dentate Gyrus Microcircuits (2015)Apróné Török IbolyaNo ratings yet
- Cell Proliferation and Cytogenesis in The Mouse Hippocampus (1991)Document90 pagesCell Proliferation and Cytogenesis in The Mouse Hippocampus (1991)Apróné Török IbolyaNo ratings yet
- AD and Epilepsy - Insight From Animal Models - Scharfman2012FutNeurolDocument16 pagesAD and Epilepsy - Insight From Animal Models - Scharfman2012FutNeurolApróné Török IbolyaNo ratings yet
- Biochemical and Biophysical Research Communications: Takafumi Ohtsuka, Masato Yano, Hideyuki OkanoDocument6 pagesBiochemical and Biophysical Research Communications: Takafumi Ohtsuka, Masato Yano, Hideyuki OkanoApróné Török IbolyaNo ratings yet
- Zinc in The Retina (2001)Document31 pagesZinc in The Retina (2001)Apróné Török IbolyaNo ratings yet
- Acute and Chronic Responses To The Convulsant Pilocarpine in DBA2J and AJ Mice (2007)Document11 pagesAcute and Chronic Responses To The Convulsant Pilocarpine in DBA2J and AJ Mice (2007)Apróné Török IbolyaNo ratings yet
- Variability in The Subcellular Distribution of Ion Channels Increases Neuronal DiversityDocument8 pagesVariability in The Subcellular Distribution of Ion Channels Increases Neuronal DiversityApróné Török IbolyaNo ratings yet
- Zinc Transporter 3 Immunohistochemical Tracing of Sprouting Mossy Fibres (2008)Document5 pagesZinc Transporter 3 Immunohistochemical Tracing of Sprouting Mossy Fibres (2008)Apróné Török IbolyaNo ratings yet
- Vagus Nerve Stimulation and Magnet Use Optimizing Benefits (2009)Document4 pagesVagus Nerve Stimulation and Magnet Use Optimizing Benefits (2009)Apróné Török IbolyaNo ratings yet
- Vagus Nerve Stimulation and Magnet Use - Optimizing Benefits (2009)Document4 pagesVagus Nerve Stimulation and Magnet Use - Optimizing Benefits (2009)Apróné Török IbolyaNo ratings yet
- Writing Letters 1 4 TasksDocument3 pagesWriting Letters 1 4 TasksmjusdNo ratings yet
- Izabella Szilvás - Exam Fright KillerDocument235 pagesIzabella Szilvás - Exam Fright KillerBálintNagyNo ratings yet
- Writing Letters 5 7 TasksDocument2 pagesWriting Letters 5 7 TasksmjusdNo ratings yet
- Health 10 Q1W1Document25 pagesHealth 10 Q1W1Gladys Pangasinan AngalaNo ratings yet
- VP Hospital Nursing Executive in Atlanta GA Resume Margaret SterbenzDocument5 pagesVP Hospital Nursing Executive in Atlanta GA Resume Margaret SterbenzMargaretSterbenzNo ratings yet
- Perbedaan Kadar Hbsag Sampel Serum Dan Plasma Metode Clia Pada PendonorDocument7 pagesPerbedaan Kadar Hbsag Sampel Serum Dan Plasma Metode Clia Pada PendonorAAK DHGRiski MaulanaNo ratings yet
- Module IIIDocument128 pagesModule IIIJoan Clarice CorlaNo ratings yet
- Laboratory Test Report: Test Name Result Biological Reference Interval Fasting Plasma Glucose: 102Document3 pagesLaboratory Test Report: Test Name Result Biological Reference Interval Fasting Plasma Glucose: 102Ramesh KumarNo ratings yet
- VA DoD Management of Concussion Mild Traumatic Brain InjuryDocument112 pagesVA DoD Management of Concussion Mild Traumatic Brain InjurycirtestNo ratings yet
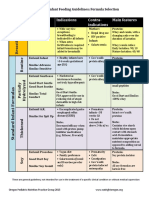
- Formula Selection OPNPGDocument2 pagesFormula Selection OPNPGRina PratiwiNo ratings yet
- AA Dermatologia in MCC 2018Document61 pagesAA Dermatologia in MCC 2018marviNo ratings yet
- Health Beliefs in Bali SlidesDocument18 pagesHealth Beliefs in Bali SlidesAwik WardaniNo ratings yet
- Myomodulation With Facial Fillers A ComprehensiveDocument13 pagesMyomodulation With Facial Fillers A ComprehensiveThiago MouraNo ratings yet
- Advise Patients Not To Exceed The Recommended Dose or Frequency of AdministrationDocument3 pagesAdvise Patients Not To Exceed The Recommended Dose or Frequency of AdministrationPrincess M Viznar BalolotNo ratings yet
- Abeba Final Thesis After DefenceDocument112 pagesAbeba Final Thesis After DefenceYayew MaruNo ratings yet
- Cognitive Behavioral Guided Self Help For The Treatment Od Recurrent Binge EatingDocument19 pagesCognitive Behavioral Guided Self Help For The Treatment Od Recurrent Binge EatingIsmael RodriguezNo ratings yet
- Congestive Heart FailureDocument4 pagesCongestive Heart FailureENo ratings yet
- Lab Scientist Job DescriptionDocument3 pagesLab Scientist Job DescriptionRajeev PareekNo ratings yet
- Global Developmental DelayDocument2 pagesGlobal Developmental DelayAtlerNo ratings yet
- Supraspinatus Tendon Pathomechanics: A Current Concepts ReviewDocument12 pagesSupraspinatus Tendon Pathomechanics: A Current Concepts Reviewgia purnamaNo ratings yet
- Quantitative Estimation of Phytoconstituents of Caesalpinia PulcherrimaDocument5 pagesQuantitative Estimation of Phytoconstituents of Caesalpinia PulcherrimaSriArthiNo ratings yet