You might also like
- Vidhya Finalised ThesisDocument84 pagesVidhya Finalised Thesisdr.vidhyaNo ratings yet
- English: Quarter 4 - Module 1: Using Appropriate Grammatical Signals or Expressions To Each Pattern of Idea DevelopmentDocument32 pagesEnglish: Quarter 4 - Module 1: Using Appropriate Grammatical Signals or Expressions To Each Pattern of Idea DevelopmentSherivieMendonza71% (7)
- Cochlear ImplantsDocument53 pagesCochlear ImplantsSovitJungBaralNo ratings yet
- Muscle Mag August 2014Document148 pagesMuscle Mag August 2014ElthonJeffrey100% (5)
- Bill of Qty. N.C. Sharma, BILSI, BadaunDocument47 pagesBill of Qty. N.C. Sharma, BILSI, BadaunNazim AliNo ratings yet
- Unidrive Classic User Guide PDFDocument195 pagesUnidrive Classic User Guide PDFkukaNo ratings yet
- Handling Silica in Cooling WaterDocument17 pagesHandling Silica in Cooling WaterLekhamani YadavNo ratings yet
- Final Research Paper On Prevalence of Failed Inductions at St. Paul's Hospital Millennium Medical College 2018 Daniel Garang Aluk Dinyo TelDocument44 pagesFinal Research Paper On Prevalence of Failed Inductions at St. Paul's Hospital Millennium Medical College 2018 Daniel Garang Aluk Dinyo TelDr. Daniel Garang Aluk50% (2)
- Assessing Nurses' Knowledge on Using Partographs During LaborDocument22 pagesAssessing Nurses' Knowledge on Using Partographs During Laborrevathidadam55555No ratings yet
- Research ProposalDocument45 pagesResearch ProposalBoruuf If GammachuuNo ratings yet
- First Draft Research Thesis Girma Huka Dukale 4122014 E.CDocument77 pagesFirst Draft Research Thesis Girma Huka Dukale 4122014 E.CGalchuu Tennoo AdulaaNo ratings yet
- Homepage: - : IntroductionDocument7 pagesHomepage: - : IntroductionIJAR JOURNALNo ratings yet
- Through Proper ChannelDocument7 pagesThrough Proper Channelcharles Aron TNo ratings yet
- Ojog 2023071715223408Document12 pagesOjog 2023071715223408Julien BwamaNo ratings yet
- Gram Stain Assessment of Laboratory ProfessionalsDocument58 pagesGram Stain Assessment of Laboratory ProfessionalsTenbite ErmiasNo ratings yet
- Ainggris Persepsi TriageDocument92 pagesAinggris Persepsi TriageFeryltriadi MohammedNo ratings yet
- Screenshot 2023-08-12 at 8.06.08 AMDocument7 pagesScreenshot 2023-08-12 at 8.06.08 AMTahseenNo ratings yet
- TerminologiaDocument21 pagesTerminologiaShirley AntezanaNo ratings yet
- 3rd Year Clinical Posting (2020 Batch) Batch J and DDocument1 page3rd Year Clinical Posting (2020 Batch) Batch J and DmasterNo ratings yet
- 1 s2.0 S0266613823000384 MainDocument7 pages1 s2.0 S0266613823000384 MainMayte Muñoz RejaNo ratings yet
- Kwawu Foster Kwesi - Breast Cancer, Knowledge, Attitudes and Perception Amongs Female Soldiers of The Ghana Armed Forces in The Greater Accra Region - 2009 PDFDocument93 pagesKwawu Foster Kwesi - Breast Cancer, Knowledge, Attitudes and Perception Amongs Female Soldiers of The Ghana Armed Forces in The Greater Accra Region - 2009 PDFNoraNo ratings yet
- Association Between Trimester and Outcomes After Cholecystectomy During PregnancyDocument9 pagesAssociation Between Trimester and Outcomes After Cholecystectomy During PregnancyElías MendezNo ratings yet
- JurnalObstetri 271 716 1 PBDocument9 pagesJurnalObstetri 271 716 1 PBChie SillentNo ratings yet
- Jurnal EmbrioDocument20 pagesJurnal Embriofamelalusu eaNo ratings yet
- DivyaradhaDocument117 pagesDivyaradhaFred OkelloNo ratings yet
- Welcome to the Obstetrics and Gynaecology Nursing DepartmentDocument57 pagesWelcome to the Obstetrics and Gynaecology Nursing DepartmentPriya SharmaNo ratings yet
- Werknesh BayeDocument46 pagesWerknesh BayeMohammed AhmedNo ratings yet
- Welo ResearchDocument49 pagesWelo ResearchTahir m. AbdelaNo ratings yet
- Rajiv Gandhi University of Health Sciences, Bangalore, Karnataka, Annexure-Ii Proforma For Registration of Subjects For DissertationDocument14 pagesRajiv Gandhi University of Health Sciences, Bangalore, Karnataka, Annexure-Ii Proforma For Registration of Subjects For DissertationJyotiNo ratings yet
- Comments On Your ProposalDocument39 pagesComments On Your Proposaljohntariku941No ratings yet
- Synopsis Format-1Document12 pagesSynopsis Format-1astha SinghNo ratings yet
- Belinda & AywakDocument74 pagesBelinda & AywakmwendaflaviushilelmutembeiNo ratings yet
- Tsegi Final ThesisDocument42 pagesTsegi Final Thesisprobby wubetuNo ratings yet
- College of Health Science Knowledge and Attitudes SurveyDocument62 pagesCollege of Health Science Knowledge and Attitudes SurveyMulugeta AbenehNo ratings yet
- Can The Nurse Do Folliculometry in Acceptable Agreement As Infertilityclinicians First Part of Ongoing Training ProgramDocument9 pagesCan The Nurse Do Folliculometry in Acceptable Agreement As Infertilityclinicians First Part of Ongoing Training Programrichardong lauNo ratings yet
- Bivariate AnalysisDocument65 pagesBivariate AnalysismelakuhunieasratieNo ratings yet
- Kassaye AhmedDocument75 pagesKassaye AhmedDNo ratings yet
- Breast Cancer Chapter 1-5Document63 pagesBreast Cancer Chapter 1-5Google MediaNo ratings yet
- ResearchDocument37 pagesResearchusamn ameenNo ratings yet
- Efficacy of An Ultrasound Trai PDFDocument15 pagesEfficacy of An Ultrasound Trai PDFAnida IzzNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument7 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- IDocument2 pagesIAllysa Megan OrpillaNo ratings yet
- Trial of Labor at The Maternity Department of The Sourosanou University Hospital (Chuss) : Clinical Aspects, The Maternal and Perinatal PrognosticsDocument8 pagesTrial of Labor at The Maternity Department of The Sourosanou University Hospital (Chuss) : Clinical Aspects, The Maternal and Perinatal PrognosticsIJAR JOURNALNo ratings yet
- Ijwh 13 395Document9 pagesIjwh 13 395Alfin AliaNo ratings yet
- ResearchDocument36 pagesResearchHarshini BaskaranNo ratings yet
- Metroplastia HisteroscopicaDocument8 pagesMetroplastia Histeroscopicaguerreroh38No ratings yet
- Association Between Cesarean Section and Placenta AccretaDocument6 pagesAssociation Between Cesarean Section and Placenta AccretaSenna mocaNo ratings yet
- Female Cosmetic Genital Surgery - Delivering What Women WantDocument6 pagesFemale Cosmetic Genital Surgery - Delivering What Women WantKelurahan Ppds Obsgyn SurabayaNo ratings yet
- Proposal Research, KimDocument32 pagesProposal Research, Kimfiraol mokonnenNo ratings yet
- Hamelmal BekeleDocument55 pagesHamelmal Bekeleidris EbrahimNo ratings yet
- Dr. HanFirst Draft Proposal PediDocument32 pagesDr. HanFirst Draft Proposal PediYasin TerraNo ratings yet
- Pregnant Women's Attitudes Toward UltrasoundDocument6 pagesPregnant Women's Attitudes Toward Ultrasoundelda zulkarnainNo ratings yet
- Arbaminch Univerisity School Ofgradute StudyDocument45 pagesArbaminch Univerisity School Ofgradute Studysinte beyuNo ratings yet
- Ugoh's ProjectDocument67 pagesUgoh's ProjectAvalanche AyomideNo ratings yet
- Ester-Final Report Dissertation 2017Document78 pagesEster-Final Report Dissertation 2017jimmy gheton100% (1)
- Nieto-Calvache. How To Differentiate Intraoperatively Between PAS and DU. BJOG 2023Document3 pagesNieto-Calvache. How To Differentiate Intraoperatively Between PAS and DU. BJOG 2023Devy JuárezNo ratings yet
- CV Albagir Mahdi AhmedDocument10 pagesCV Albagir Mahdi AhmedYasar HammorNo ratings yet
- REFERAT Induced AbortionDocument19 pagesREFERAT Induced AbortionFajar Akbar RamadhanNo ratings yet
- Ho Proposal - For MergeDocument25 pagesHo Proposal - For Mergefiraolab5No ratings yet
- CVDocument7 pagesCVmmmmder7No ratings yet
- No. 223-Content of A Complete Routine Second Trimester Obstetrical Ultrasound Examination and ReportDocument6 pagesNo. 223-Content of A Complete Routine Second Trimester Obstetrical Ultrasound Examination and ReportYolpa Figueroa PorrasNo ratings yet
- Guidelines for diagnosis and treatment of laparoscopy during pregnancyDocument13 pagesGuidelines for diagnosis and treatment of laparoscopy during pregnancyCecilia Quispe JaureguiNo ratings yet
- Example Icu CV PDFDocument6 pagesExample Icu CV PDFKeeranmayeeishraNo ratings yet
- Sadeq Saad Abd El Moghny, Ahmed Kaid Allow, Belqees Ahmed and Bracamonte MaryamDocument7 pagesSadeq Saad Abd El Moghny, Ahmed Kaid Allow, Belqees Ahmed and Bracamonte Maryamgamal attamNo ratings yet
- How Does SubchorionicDocument8 pagesHow Does SubchorionicNovi Nurlaeli Dwi PutriNo ratings yet
- Multiparametric Ultrasound Diagnosis of Breast DiseasesFrom EverandMultiparametric Ultrasound Diagnosis of Breast DiseasesGennady T. SukhikhNo ratings yet
- Agriculture (IAS 41)Document45 pagesAgriculture (IAS 41)Miljane Perdizo100% (1)
- Trainers ManualDocument31 pagesTrainers ManualtalilaNo ratings yet
- Practice Exercise - Nairobi - BlankDocument4 pagesPractice Exercise - Nairobi - BlanktalilaNo ratings yet
- Final ProposalDocument25 pagesFinal Proposaltalila0% (1)
- Practical Attachement FormDocument7 pagesPractical Attachement FormtalilaNo ratings yet
- New Melke TwoDocument62 pagesNew Melke TwotalilaNo ratings yet
- Dupont Heir Sexually Abuses DaughterDocument3 pagesDupont Heir Sexually Abuses DaughterJuandelaCruzNo ratings yet
- BKTK-2010, Failure in Material ConstructionsDocument17 pagesBKTK-2010, Failure in Material ConstructionsSorulay Way-neyNo ratings yet
- Sampling Methods for Terrestrial Amphibians and ReptilesDocument39 pagesSampling Methods for Terrestrial Amphibians and ReptilesBenzu Shawn100% (1)
- Online Pharmacy: Customer ProfilingDocument6 pagesOnline Pharmacy: Customer ProfilingGeorge SebastianNo ratings yet
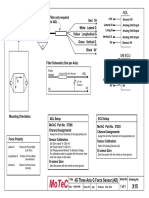
- Filter and wiring schematic for 3-axis ADL G-force sensorDocument1 pageFilter and wiring schematic for 3-axis ADL G-force sensorJuan Ramón Pérez LorenzoNo ratings yet
- 20090716FoxReiki PDFDocument40 pages20090716FoxReiki PDFAgustina RomeroNo ratings yet
- Ecl7000 enDocument2 pagesEcl7000 ensuchaya tupyangNo ratings yet
- FORM HSE MATRIX TRAINING (Contoh)Document1 pageFORM HSE MATRIX TRAINING (Contoh)Hifni GhazaliNo ratings yet
- MYK Grout Card 2Document2 pagesMYK Grout Card 2Abdul Raheem SyedNo ratings yet
- Name: Sport: Movement PrepDocument24 pagesName: Sport: Movement PrepS HNo ratings yet
- Working Length Determination in RCTDocument38 pagesWorking Length Determination in RCTDidar Sadiq Kwekha100% (1)
- A Study On Satisfaction Level of Employees With Special Reference Textile IndustryDocument12 pagesA Study On Satisfaction Level of Employees With Special Reference Textile Industrysai kiran bade100% (1)
- 465 886 1 SMDocument8 pages465 886 1 SM17Annisa Muthmainnah067No ratings yet
- CPR Team DynamicsDocument31 pagesCPR Team Dynamicsapi-205902640No ratings yet
- Different Mesh Sizes and Mesh To Micron ConversionDocument10 pagesDifferent Mesh Sizes and Mesh To Micron ConversionDevanandDongreNo ratings yet
- APC Symmetra PX-2Document8 pagesAPC Symmetra PX-2drastir_777No ratings yet
- Product Brochure-Electronically Controlled Air Dryer-ECA PDFDocument4 pagesProduct Brochure-Electronically Controlled Air Dryer-ECA PDFAnonymous O0T8aZZNo ratings yet
- Piriformis MuscleDocument3 pagesPiriformis MuscleBen CampbellNo ratings yet
- Cost Control ReviewerDocument13 pagesCost Control ReviewerMatthew Ivan HerreraNo ratings yet
- Rear Derailleur: Important Notice Names of PartsDocument1 pageRear Derailleur: Important Notice Names of PartsRyan MulyanaNo ratings yet
- Animal Names in English and Telugu - 20170912 - 182216545Document17 pagesAnimal Names in English and Telugu - 20170912 - 182216545karimulla goraNo ratings yet
- Ventilation System Comparison - Constant Air Volume (CAV) and Variable Air Volume (VAV)Document15 pagesVentilation System Comparison - Constant Air Volume (CAV) and Variable Air Volume (VAV)ankurNo ratings yet
- "Fish" From Gourmet RhapsodyDocument4 pages"Fish" From Gourmet RhapsodySean MattioNo ratings yet
- Measuring Instruments Temperature GuideDocument52 pagesMeasuring Instruments Temperature GuidemohammedhanafyNo ratings yet